10 March 2021: Articles 
An Unusual Presentation of ST Elevation Myocardial Infarction Complicated with Cardiogenic Shock Due to Myxedema Coma: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care
Nabil Braiteh1ABCDEF*, Godson D. Senyondo2ABCDEF, Mohammed Faraaz Rahman3ABEF, Raheel Chaudhry2ABEF, Hisham Kashou1ACDDOI: 10.12659/AJCR.929573
Am J Case Rep 2021; 22:e929573






Abstract
BACKGROUND: Myxedema coma is an endocrine emergency with a high mortality rate, defined as a severe hypothyroidism leading to hypotension, bradycardia, decreased mental status, hyponatremia, hypoglycemia, and cardiogenic shock. Although hypothyroidism and cardiac disease has been interlinked, ST elevation myocardial infarction in the setting of myxedema coma have not been reported previously.
CASE REPORT: We report the case of a 70-year-old man who presented to the Emergency Department with chest pain and confusion. He also reported fatigue for the past week, which was progressively worsening. His past medical history was significant for renal cell carcinoma with metastatic bone disease being treated with chemotherapy (axitinib and pembrolizumab). In the Emergency Department, an ECG revealed inferior ST elevations. Shortly after presentation, the patient’s blood pressure was decreasing, he became bradycardic (sinus), and his mental status was getting worse, so he was intubated for airway protection and was taken emergently for a cardiac catheterization, which failed to reveal an acute coronary occlusion. TSH was 60.6 mIU/L (0.465-4.680) mIU/ML, and free T4 0.3 ng/dL (0.8-2.2) ng/dL. The cardiac index was calculated to be 0.8 L/min/m² (normal range 2.6-4.2 L/min/m²), which confirmed cardiogenic shock due to myxedema coma. He was treated with levothyroxine (T4), liothyronine (T3), hydrocortisone, and multiple vasopressors but failed to respond and died 13 h after admission to the hospital.
CONCLUSIONS: Because of its rarity and high mortality, early diagnosis of myxedema coma and initiation of treatment by cardiologists requires a high level of suspicion, especially when patients with a history of hypothyroidism present with a cardiac complaint (ie, acute coronary syndrome, or bradycardia) that does not completely fit the clinical picture. It is of utmost importance for physicians to keep a wide differential diagnosis of other causes of ST elevation and/or persistent cardiogenic shock.
Keywords: acute coronary syndrome, Hypothyroidism, Shock, Cardiogenic, Coma, Myxedema, ST elevation myocardial infarction, thyroxine
Background
Myxedema coma is primarily a disorder of the thyroid gland, which eventually leads to slower functioning of multiple organs and is a medical emergency with a high mortality rate [1]. It is a form of severe hypothyroidism that leads to hypotension, bradycardia, decreased mental status, hyponatremia, and hypoglycemia [2]. Cardiac effects include decreased myocardial contractility and low cardiac output leading to hypotension. Pericardial effusion can also be present, but left ventricular ejection fraction is rarely affected.
Decreased cardiac output occurs in hypothyroidism due to increase in vascular resistance and change in gene expression [3]. Vascular resistance is increased due to lack of T4 effect on initiating the release of endothelial-derived relaxing factor [4].
Thyroid disease and the cardiovascular system have an intricate relationship. Although patients with known stable angina will have less symptoms when they are in a hypothyroid state due to decreased activity and less oxygen demand, it is presumed that hypothyroidism is associated with accelerated coronary artery disease due to increased homocysteine levels, dyslipidemia, elevated concentrations of C-reactive protein, endothelial dysfunction, and increase in diastolic blood pressure [3,4].
To the best of our knowledge, a direct association between acute myocardial infarction and myxedema coma has not been previously reported. Herein, we report the case of a 70-year-old man who presented with ST elevation myocardial infarction complicated with cardiogenic shock due to myxedema coma.
Case Report
A 70-year-old man presented to the Emergency Department with chest pain and confusion. The pain started 1 day prior to presentation, was centrally located, and radiated to his bilateral shoulders. He also reported fatigue for the past week, which was progressively getting worse.
His past medical history was significant for renal cell carcinoma with metastatic bone disease being treated with chemo-therapy (axitinib and pembrolizumab), a recent diagnosis of hypothyroidism, chronic kidney disease stage 2, benign essential hypertension, and paroxysmal atrial fibrillation.
His past surgical history was significant for a total nephrectomy. He denied tobacco, alcohol, or illicit drug abuse. His home medications were intravenous pembrolizumab 200 milligrams every 3 weeks, oral axitinib 7 milligrams twice daily, oral carvedilol 12.5 milligrams twice daily, and oral levothyroxine 25 micrograms once daily.
Upon presentation to the Emergency Department, his vitals were significant for a blood pressure of 93/52 mmHg, heart rate of 96 beats per minute (bpm), oral temperature was 37.2 degrees Celsius with a 96% saturation on room air. Physical exam was significant for being altered, lethargic, and not oriented to time, place, and date, with a Glasgow coma scale of 11. Cardiac and lung exams were unremarkable. A 12-lead ECG showed ST elevations in leads II, III, and aVF, and a sinus rhythm with a first-degree AV block at a rate of 98 bpm (Figure 1). Shortly after presentation, the patient’s blood pressure was decreasing, he became bradycardic (sinus), and his mental status was getting worse, so he was intubated for airway protection. He was given 1 dose of 0.5 milligrams of intravenous atropine and was started on a norepinephrine and dopamine drip. Subsequently a STEMI code was called and he was started on acute coronary syndrome treatment and was transferred to the cardiac catheterization lab.
Prior to dispatch to the cardiac catheterization lab, the patient had a brief episode of cardiac arrest preceded with sinus bradycardia that required a total of 2 min of cardiopulmonary resuscitation, and 1 dose of 0.5 milligrams intravenous epinephrine until return of spontaneous circulation was achieved.
Left and right heart catheterization was performed. A coronary angiogram showed no evidence of atherosclerotic coronary disease in the left main, left anterior descending artery, and in the left circumflex artery. There was evidence of a 60% concentric lesion in the distal right coronary artery (Figure 2) that was disproportionate to the clinical picture, so no intervention was done. The cardiac index was calculated to be 0.8 L/min/m2 (normal range 2.6–4.2 L/min/m2). During the procedure, the patient had another episode of cardiac arrest preceded by torsade de pointes that was treated with unsynchronized cardioversion with 150 Joules and 2 grams of intravenous magnesium.
A transthoracic echocardiogram was performed, which revealed a normal ejection fraction estimated at 50–55% and a small pericardial effusion measuring 0.9 cm (Figure 3), with no significant valvular heart disease. His ST elevations resolved gradually within 2–3 h after admission. Laboratory data are listed in Table 1.
Arterial blood gas revealed a pH of 7.26 (7.35–7.55), PaCo2 33.8 (35.0–45.0) MMHG, PaO2 92 (80–100) MMHG, HCo3 14.6 (22.0–24.0) MEQ/L, saturation of 91.7% (92.0–100.0)% on assisted control mode ventilation, tidal volume of 550 ml, Fio2 of 100%, and respiratory rate of 16/min.
A diagnosis of myxedema coma was immediately made, and 400 micrograms of intravenous levothyroxine (T4) and 20 micrograms of intravenous liothyronine (T3) were given first. Then, 100 milligrams of intravenous hydrocortisone were administered. The patient continued to deteriorate, requiring more vasopressors at high dosages (dopamine at 20 mcg/kg/min, norepinephrine at 200 mcg/min, epinephrine 100 mcg/min, and phenylephrine at 200 mcg/min). He was also started on empiric antibiotic treatment pending blood and urine culture results. Another transthoracic echocardiogram was performed 6 h after hospitalization, which did not show any new changes, with stable pericardial effusion.
Despite all the above measures, the patient was not responding, and he dies 13 h after hospital admission.
Discussion
A review of the literature did not identify any reported cases of acute myocardial infarction occurring in the setting of myxedema coma, which is thought to be a rather rare occurrence. Our patient had been on chemotherapy with Axitinib and Pembrolizumab for advanced renal cell cancer, which is likely the explanation of his new-onset worsening hypothyroidism, for which he was treated with a suboptimal dose of 25 micrograms of oral levothyroxine.
Although the combination of pembrolizumab plus axitinib has proven to be effective in the treatment of advanced renal cell carcinoma in comparison to other alternatives, this combination has been strongly linked to hypothyroidism [5].
Our patient presented with an inferior STEMI complicated with cardiogenic shock and bradycardia, leading to cardiac arrest, all in the setting of myxedema coma. The question to be answered is whether this was a coincidence or whether the myxedema coma led to the STEMI.
There are 2 hypotheses that could explain the patient’s presentation. First, the patient already had a chronic moderate-severe distal RCA lesion, which had progressed into a total occlusion in the setting of plaque rupture due to the stressful metabolic state of the body caused by myxedema coma. Likely, the plaque had dislodged peripherally or was broken. Intravenous ultrasound would have been useful to evaluate this further to rule out a plaque rupture; however, it was not done as the patient was in critical condition and it may not have changed outcome. We think that this theory is less likely since there was no evidence of inferior wall hypokinesis and no evidence of distal RCA thrombus by angiography.
The second hypothesis is that the patient already had a chronic moderate distal RCA lesion (60% occlusion) as identified by the coronary angiogram (Figure 2), and the stress of myxedema coma led to an acute coronary spasm in the RCA, causing inferior STEMI. This is the more likely theory considering that the coronary angiogram showed no evidence of atherosclerosis in other arteries, along with resolution of ST elevations. Known triggers of coronary spasm include thyroid dysfunction, collagen disorders, smoking, and abuse of drugs such as amphetamines and cocaine [6].
In addition, the mechanism of ST elevations would change management significantly. If it were due to a plaque rupture, then the patient should be treated with an acute coronary syndrome protocol that includes aspirin, P2Y12 inhibitors, anticoagulation, and percutaneous coronary intervention, while coronary spasm should be treated by reversing the inciting factor and the use of calcium channel blockers or nitrates.
Our patient had severe bradycardia requiring a temporary transvenous pacer, small pericardial effusion, cardiogenic shock (cardiac index of 0.8 L/min/m2), severe lethargy leading to a comatose state, hyponatremia, evidence of severe hypothyroidism (TSH 60.6 mIU/L, free T4 of 0.3 mcg/dL), and secondary adrenal insufficiency (cortisol of 2.0 mcg/dl), all due to myxedema coma. In patients suspected to be in a myxedema coma, the history-taking should be focused on any new medications, treatments, and newly diagnosed diseases such as cancer. There are myriads of new chemotherapy medications and physicians should make an attempt to focus on serious life-threatening adverse effects of these drugs. Moreover, other causes of shock, such as infectious, cardiac, or hypovolemic factors, should be ruled out.
Our patient was started on intravenous levothyroxine after coronary angiography, which was due to late diagnosis of myxedema coma considering the 2 life-threatening events. We recommend initiation of treatment with both intravenous levothyroxine and coronary angiography simultaneously in this scenario if both were diagnosed in a timely manner. However, the presence of STEMI can alter management due to its high mortality and the emergent need for cardiac catheterization.
When myxedema coma is suspected, treatment should be initiated without waiting for laboratory confirmation. It is a medical emergency that carries a high mortality rate of 50–60% [7]. Treatment consists of thyroid hormone replacement, supportive measures, management of coexisting problems (ie, infection), and steroids (until coexisting adrenal insufficiency has been excluded) [8].
Conclusions
Our case adds new data on cardiac complications of severe hypothyroidism (ie, myxedema coma) and presents a novel relationship between myxedema coma and ST elevation myocardial infarction. It also sets a platform for future research and publications exploring rare cardiac complications of thyroid disease.
It is of utmost importance for physicians to keep a wide differential diagnosis of other causes of ST elevation and/or persistent cardiogenic shock when a coronary angiogram and a transthoracic echocardiogram both fail to explain the full clinical picture. Obtaining a thorough history was key in pursuing another diagnosis (ie, myxedema coma) in our case.
Figures
Tables
Table 1.. Laboratory data.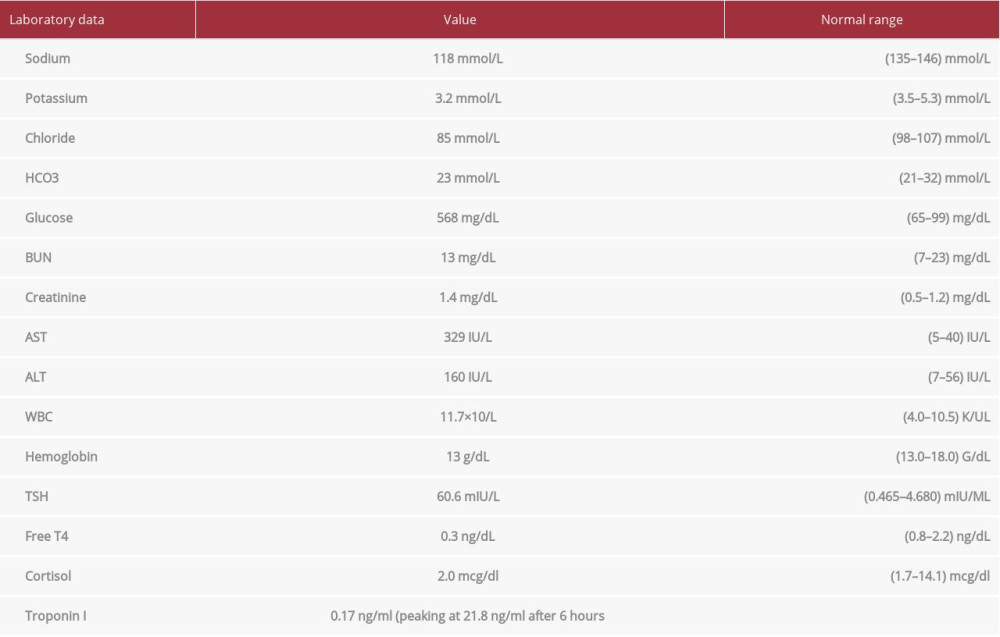
References:
1.. Elshimy G, Correa R, Myxedema: StatPearls, 2020, Treasure Island (FL), StatPearls Publishing [Internet].
2.. Klein I, Thyroid hormone and the cardiovascular system: Am J Med, 1990; 88(6); 631-37
3.. Klein I, Danzi S, Thyroid disease and the heart: Circulation, 2007; 116(15); 1725-35
4.. Taddei S, Caraccio N, Virdis A, Impaired endothelium-dependent vasodilatation in subclinical hypothyroidism: beneficial effect of levothyroxine therapy: J Clin Endocrinol Metab, 2003; 88(8); 3731-37
5.. Atkins MB, Plimack ER, Puzanov I, A non-randomised, open-label, dose-finding, and dose-expansion phase 1b trial: Lancet Oncol, 2018; 19(3); 405-15
6.. Hadi H, D’souza S, El-Omar M, Hypovolemia-induced severe coronary spasm leading to acute myocardial infarction: Exp Clin Cardiol, 2012; 17(2); 74-76
7.. Ono Y, Ono S, Yasunaga H, Clinical characteristics and outcomes of myxedema coma: outcomes of myxedema coma: Analysis of a national inpatient database in Japan: J Epidemiol, 2017; 27(3); 117-22
8.. Kwaku MP, Burman KD, Myxedema coma: J Intensive Care Med, 2007; 22; 224
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.949976
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950290
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950607
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950985
Most Viewed Current Articles
07 Dec 2021 : Case report
17,691,734
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  164,491
164,491
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
113,090
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
59,175
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133