03 September 2021: Articles 
Central Venous Sinus Thrombosis with Subarachnoid Hemorrhage Following an mRNA COVID-19 Vaccination: Are These Reports Merely Co-Incidental?
Unusual clinical course, Unusual or unexpected effect of treatment, Unexpected drug reaction
Khezar Syed1ABDEF*, Haseeb Chaudhary1ABDEF, Anthony Donato1EDOI: 10.12659/AJCR.933397
Am J Case Rep 2021; 22:e933397






Abstract
BACKGROUND: Multiple vaccines have been developed against COVID-19 as a collaborative worldwide effort. On March 18, 2021 the European Medicines Agency reported a serious and rare adverse effect of thrombosis with thrombocytopenia syndrome (TTS) after receiving the ChAdOx1 nCoV-19 vaccine; most of these cases were associated with cerebral venous sinus thrombosis (CVST). To date, there are no cases of TTS-related CVST reported after receipt of either of the 2 mRNA COVID-19 vaccines authorized for use in the United States. We report a case of CVST with the Moderna mRNA vaccine.
CASE REPORT: A healthy 45-year-old male patient without any risk factors presented with new-onset seizures 8 days after the receipt of the 2nd dose of Moderna (mRNA-1273), with concomitant SAH as a complication. One day prior to admission, he noted headaches and neck pain unrelieved by over-the-counter analgesics. Computed tomography (CT) scan brain without contrast revealed a left frontal lobe intracerebral hemorrhage (ICH) along with subarachnoid hemorrhage (SAH). A subsequent contrast-enhanced magnetic resonance imaging (MRI) brain confirmed the CT findings as well as anterior superior sagittal sinus thrombosis. He had normal platelet count with a negative thrombophilia work-up and cancer screening. He was successfully anticoagulated with heparin and discharged on warfarin without neurological sequelae or further seizures. The case was reported to the US Vaccine Surveillance System.
CONCLUSIONS: mRNA vaccine-related CVST is an extremely rare phenomenon. More data are needed to establish causality and understand the role of vaccine-related immune response resulting in thrombotic events with or without TTS.
Keywords: COVID-19 vaccine, Intracranial Hemorrhages, Sagittal Sinus Thrombosis, 2019-nCoV Vaccine mRNA-1273, COVID-19, COVID-19 Vaccines, Humans, RNA, Messenger, Sinus Thrombosis, Intracranial, Subarachnoid Hemorrhage, United States, Vaccination
Background
Almost a year and a half into the pandemic, not only did we decode the responsible pathogen but had vaccines designed, tested in clinical trials, globally manufactured, and distributed against the deadly virus. This is a testament to human ingenuity and greatness achieved through science and collaboration across society [1].
On December 10, 2020, the FDA granted EUA (Emergency Use Authorization) to the first messenger RNA (mRNA) vaccine: the Pfizer-BioNTech (BNT162b2) COVID-19 vaccine [2]. It was quickly succeeded by a second mRNA vaccine, mRNA-1273 (Moderna), on December 18, 2020 [3]. The Ad26.COV2.S COVID-19 vaccine (Janssen/Johnson) was the third COVID-19 vaccine, approved for EUA on February 27, 2021. It was the first non-mRNA-based COVID-19 vaccine in the USA using a human adenoviral vector [4].
The European Medicines Agency reported a serious adverse effect of thrombosis with thrombocytopenia syndrome (TTS) after receiving the ChAdOx1 nCoV-19 vaccine (Oxford/AstraZeneca) on March 18, 2021. This vaccine used a recombinant replication-deficient chimpanzee adenovirus vector [5,6]. Several other cases of TTS from these recombinant human adenoviral vector Covid-19 vaccines have since been reported through post-marketing surveillance in both viral-vector vaccines. The reported cases of TTS to the Vaccine Adverse Event Reporting System (VAERS) were 7.0 cases per million administered to women aged 18–49 years and 0.9 per million to women aged ≥50 years from the Janssen COVID-19 vaccine [8]. Cerebral venous sinus thrombosis (CVST) was present in most of them. On April 13, 2021, the CDC and FDA recommended a pause on the Janssen/ Johnson vaccine as the number of TTS- related CVST cases were being reported to VAERS (Vaccine Adverse Effects Reporting System) [7]. The CDC’s Advisory Committee on Immunization Practices (ACIP) re-emphasized the benefits of Ad26.COV2.S COVID-19 vaccine in adults 18 and above on April 23, 2021 [8].
By May 28, 2021, 123 479 196 doses of the Moderna vaccine had been administered in the US [9]. So far, 8 cases have been reported to VAERS for CVST possibly due to Moderna vaccination. The CDC has not yet endorsed any cases to the 2 mRNA vaccines. We report one such case of CVST with hemorrhagic transformation leading to subarachnoid hemorrhage (SAH), which may be a rare adverse effect associated with mRNA vaccines, and calls for a continued post-marketing surveillance and understanding of non-TTS-related thrombosis.
Case Report
A 45-year-old man with a background history of diabetes mellitus presented to the emergency room with an altered mental state after a witnessed seizure. He had no prior history of a seizure disorder or head trauma. He had received his second dose of mRNA-1273 on 04/30/2021, 28 days after his first dose. For the first few days, he had local adverse effects, including soreness on the site of injection and arm pain. Seven days after the day of vaccination, he started having headaches and neck pain that did not relieve with over-the-counter analgesics. On the day of presentation (day 8 after receiving the vaccine), he had worsening headache, with a tonic-clonic seizure witnessed by his partner. This was followed by another episode on arrival of the emergency medical services (EMS). The patient was found to be in a postictal state accompanied by tachypnea. He was hypertensive with a blood pressure of 147/48 mmHg with a heart rate of 140 bpm and a respiratory rate of 40 breaths per minute, and oxygen saturation of 86% on room air, which improved with jaw thrust and a nasal trumpet to 96%. His Glasgow coma scale (GCS) was 3. His blood glucose was 237 mg/dL. The rhythm strip revealed sinus tachycardia. He received 4 mg i.v. lorazepam and was transferred to the Emergency Department with a nasal airway.
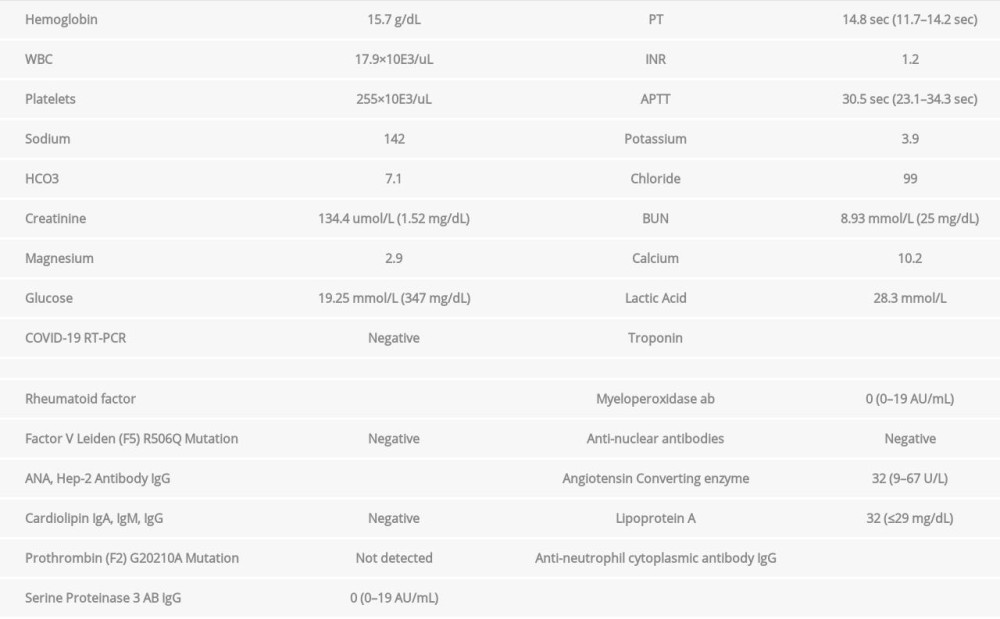
The patient was transferred to the Emergency Department (ED), where blood pressure on arrival was 198/98 mmHg, and heart rate of 157 bpm with a respiratory rate of 42 bpm. His GCS on arrival to the ED had improved to 6/15. He was immediately intubated for airway protection. An urgent blood gas analysis revealed a pH of 7.32, PO2 168, PCO234, HCO3 18, with lactic acid of 28 mmol/L (Table 1). EKG on arrival did not reveal any acute ST-T changes, and a chest X-ray was normal. An urgent computed tomography (CT) scan brain without contrast revealed a left frontal lobe intracerebral hemorrhage (ICH) along with subarachnoid hemorrhage (SAH) (Figure 1).
The patient was transferred to the Intensive Care Unit (ICU) under the care of the neurocritical care team for management of ICH with SAH. The patient initially received intravenous esmolol 50 mcg/kg/min infusion and nimodipine 60 mg Q4 hourly; levetiracetam 500 mg twice daily was added for seizure prophylaxis. He subsequently underwent a contrast-enhanced magnetic resonance imaging (MRI) brain, which revealed intracranial hemorrhage within the anterior left frontal lobe without a definitive underlying enhancing mass, bifrontal subarachnoid hemorrhage, and anterior superior sagittal sinus thrombosis (Figures 2, 3).
For confirmation, the patient underwent diagnostic cerebral angiography, which revealed an absence of opacification in the anterior 1/2 of the superior sagittal sinus, consistent with acute venous sinus thrombosis with collateral drainage through the cavernous sinus (Figure 4).
Upon confirmation of CVST, anticoagulation was started with intravenous heparin and later transitioned to coumadin, with a goal INR of 2–3. He underwent a CT scan of the chest, abdomen, and pelvis, which ruled out any occult malignancies or other thrombosis. His echocardiogram showed a normal ejection fraction, no septal defects, and no intracardiac clots or valvular pathologies. A complete hypercoagulable panel (Table 1) was within normal limits.
He was successfully treated and discharged with no neurological sequelae, with a follow-up in the vascular neurology clinic in 4 weeks with no recurrence.
His case was reported to the VAERS, E-Report Number: 515068)
Discussion
The symptoms concerning CVST are a new-onset headache that has minimal response to analgesia, exacerbation of bending or lying down and/or associated with neurological deficits. Isolated headache may be the only presentation of a CVST occurring in 6–23% of the patients [10]. Similar warnings have been issued by ACIP for recipients of adenovirus vector-based vaccines [11]. The diagnosis can be missed initially if a contrast-enhanced imaging is not performed. Our case had a hemorrhagic transformation with involvement of the subarachnoid space from venous thrombosis, which led to more sophisticated imaging on an urgent basis and helped in establishing the diagnosis earlier in the disease course. The complication of SAH with CVST is rare but well established and has been previously described in several cases [12]. It is believed to occur from the increased venous pressure in the cortical veins affected by thrombosis causing rupture of these fragile vessels with subsequent parenchymal hemorrhage that enters the adjacent subarachnoid space [13,14]. Our index case did not have a known risk factor to develop CVST, with a normal platelet count of 255x10 3/uL and negative complete thrombophilia and autoimmune work-up.
Most reported cases of CVST from COVID-19 vaccines are attributed to the development of TTS. TTS, also referred to as vaccine-induced immune thrombotic thrombocytopenia (VITT), is a rare syndrome that can involve acute venous or arterial thrombosis with a new-onset thrombocytopenia in the absence of exposure to heparin [15]. Most post-authorization cases of TTS following Ad26.COV2.S COVID-19 (Jansen) and ChAdOx1 nCoV-19 (Astra-Zeneca) vaccines occurred in female recipients, with CVST as the most common site across Europe and the USA [8,15]. The median age of these cases was 37 years (18–59 years), and the median interval from vaccination to symptom onset was 8 days (6–15 days) in the United States, which is consistent with the data from other parts of the world proposing younger population at risk (<50 years) with a range of onset of symptoms from 4 to 20 days according to a recent report from the Global Advisory Committee on Vaccine Safety [6]. The mechanism remains poorly understood but it is postulated to be similar to heparin-induced thrombocytopenia (HIT) with IgG antibodies that recognize platelet factor 4, causing activation of platelets in most of the reported cases [4]. This has significant bearing, as the management of these cases involves non-heparin-based anticoagulation and/or immunoglobin therapy. Although these 2 vaccines differ substantially based on their viral-vector and use separate host-receptors to exert their response [16], the exact mechanism behind generation of these antibodies is unknown.
In general, the pandemic-afflicted population at large carries a higher risk of having a thrombotic event as cases related to CVST continue to emerge from active COVID-19 infections. In a large retrospective study of 537 913 patients, the incidence of CVST within 2 weeks of COVID-19 diagnosis was 42.8 per million people (95% CI 28.5–64.2) [17]. The risk was significantly higher compared to the matched mRNA vaccine control cohort, where the incidence of CVT was compatible with the lowest estimate of the baseline rate in the USA of 0.53 per million people in any 2-week period.
To date there are no cases of TTS-related CVST reported after receipt of either of the 2 mRNA COVID-19 vaccines authorized for use in the United States [18]. The report by the Advisory Committee on Immunization Practices (ACIP) on May, 12 2021 also mentioned a total of 11 cases of CVST following mRNA vaccines, of which 3 were from Pfizer-BioNTech and 8 from Moderna [18]. Only 6 of these were potential incident cases and none of them had thrombocytopenia. Our patient did not have an evidence of thrombocytopenia, as well, which may suggest a mechanism other than TTS that may be responsible if similar cases continue to emerge.
Owing to the small number of patients experiencing vaccine-related thrombosis, these reports are not designed to prove causality due to the lack of statistical power. However, these findings continue to add to the body of evidence for clinicians caring for patients with underlying medical conditions or risk factors for hypercoagulability, and will help recognize such rare events early. At present, the consensus strongly suggests the benefits far outweigh potential harm as collaborative worldwide vaccination efforts continue to reduce the healthcare burden and mortality from COVID-19 [19].
Conclusions
mRNA-related CVST is extremely rare. More data are needed to establish causality, along with collaborative efforts to understand the role of vaccine-related immune response resulting in thrombotic events with or without TTS.
Figures
References:
1.. Baden LR, El Sahly HM, Essink B, Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine: N Engl J Med, 2021; 384(5); 403-16
2.. Hinton D, Pfizer-BioNTech COVID-19 vaccine EUA letter of authorization re-issued 05-10 2021: U.S. Food & Drug Administration website Accessed May 28,2021. https://www.fda.gov/media/144412/download
3.. Hinton D, Moderna COVID-19 vaccine EUA letter of authorization: U.S. Food & Drug Administration website Accessed May 28,2021. https://www.fda.gov/media/144636/download
4.. See I, Su JR, Lale A, US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26.COV2.S vaccination, March 2 to April 21, 2021: JAMA, 2021; 325(24); 2448-56
5.. , COVID-19 Vaccine AstraZeneca: Benefits still outweigh the risks despite possible link to rare blood clots with low blood platelets Accessed April 20, 2021https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots
6.. , Global Advisory Committee on Vaccine Safety (GACVS) review of latest evidence of rare adverse blood coagulation events with AstraZeneca COVID-19 Vaccine (Vaxzevria and Covishield) Accessed May 28 2021https://www.who.int/news/item/1604-2021-global-advisory-committee-on-vaccine-safety-(gacvs)-review-of-latest-evidence-of-rare-adverse-blood-coagulation-events-with-astrazeneca-covid-19-vaccine-(vaxzevria-and-covishield)
7.. , Joint CDC FDA statement on Johnson & Johnson COVID-19 vaccine April 13, 2021 Accessed April 19, 2021https://www.cdc.gov/media/releases/2021/s0413-JJ-vaccine.html
8.. MacNeil JR, Su JR, Broder KR, Updated Recommendations from the Advisory Committee on Immunization Practices for Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine After Reports of Thrombosis with Thrombocytopenia Syndrome Among Vaccine Recipients – United States, April 2021: MMWR Morb Mortal Wkly Rep, 2021; 70(17); 651-56
9.. , Centers for Disease Control and Prevention Accessed May 28, 2021//covid.cdc.gov/covid-data-tracker/#vaccinationshttps:
10.. Mehta A, Danesh J, Kuruvilla D, Cerebral venous thrombosis headache: Curr Pain Headache Rep, 2019; 23(7); 47
11.. Oliver S, Thrombocytopenic thrombosis after Janssen Vaccine: Work Group Interpretation ACIP Meeting April 14, 2021 Accessed May 28, 2021. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-04/05-COVID-Oliver-508.pdf
12.. Boukobza M, Crassard I, Bousser MG, Chabriat H, Radiological findings in cerebral venous thrombosis presenting as subarachnoid hemorrhage: A series of 22 cases: Neuroradiology, 2016; 58(1); 11-16
13.. Pradhan S, Yadav R, Diwakar H, Phadke RV, Subarachnoid hemorrhage following chronic dural venous sinus thrombosis: Angiology, 2007; 58(4); 498-501
14.. Kato Y, Takeda H, Furuya D, Subarachnoid hemorrhage as the initial presentation of cerebral venous thrombosis: Intern Med, 2010; 49(5); 467-70
15.. Greinacher A, Thiele T, Warkentin TE, Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination: N Engl J Med, 2021; 384(22); 2092-101
16.. Sadoff J, Davis K, Douoguih M, Thrombotic thrombocytopenia after Ad26. COV2.S Vaccination – response from the manufacturer: N Engl J Med, 2021; 384(20); 1965-66
17.. Taquet M, COVID-19 and cerebral venous thrombosis: A retrospective co-hort study of 513,284 confirmed COVID-19 cases [Internet]: OSF, 2021 Available from: osf.io/h2mt7
18.. Shimabukuro T, Thrombosis with thrombocytopenia syndrome (TTS) following Janssen COVID-19 vaccine [Internet] . 2021 [cited 2021 May 30] Available from: Cdc.gov
19.. Hunter PR, Thrombosis after COVID-19 vaccination: BMJ, 2021; 373; n958
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953049
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952567
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953259
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953110
Most Viewed Current Articles
07 Dec 2021 : Case report
22,744,454
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report
175,030
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,056
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,026
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133