29 September 2021: Articles 
Lemierre’s Syndrome in an Elderly Female Patient with Polycythemia Vera: Does Polycythemia Vera Predispose to Lemierre’s Syndrome?
Unusual clinical course, Challenging differential diagnosis
Sanchit V. Kundal1ABCDEF*, Jasmine Lee2BDEF, Mazin Khalid3DEF, Jacob Shani3DEF, Gerald M. Hollander3DEF, Zhou Ping1EF, Chun Maung2EF, Vijay S. Shetty1DEFDOI: 10.12659/AJCR.933587
Am J Case Rep 2021; 22:e933587






Abstract
BACKGROUND: Lemierre’s syndrome (LS), a potentially fatal condition, is characterized by thrombophlebitis of a head or neck vein secondary to a head or neck infection, most commonly involving Fusobacterium necrophorum. Its association with polycythemia vera (PV) is not well reported despite the predisposition to thrombogenesis.
CASE REPORT: We present the case of a 66-year-old woman with a known history of polycythemia vera (PV) who presented with 4 days of worsening right-sided neck pain and odynophagia. The physical examination revealed poor oral dentition, mild erythema of the posterior pharyngeal mucosa, and non-erythematous tonsils without exudate. A computed tomography with i.v. contrast of the neck revealed complete thrombosis of the right internal jugular vein (IJV). Treatment was initiated with i.v. antibiotics and anticoagulation, with symptoms improving rapidly within 24 h. She was eventually discharged on apixaban and clindamycin and was encouraged to follow up with her hematologist.
CONCLUSIONS: PV predisposes patients to a hyper-viscous and prothrombotic state, which may warrant a stronger suspicion of Lemierre’s syndrome. In addition, lack of aspirin use for prophylaxis of thrombosis and undiagnosed oral infection are factors to consider when assessing risk factors for Lemierre’s syndrome in PV patients.
Keywords: Lemierre Syndrome, Polycythemia vera, Thrombophlebitis, Chest Pain, Female, Fusobacterium necrophorum, Humans, Jugular Veins
Background
Lemierre’s syndrome (LS) is a rare condition with an incidence of around 1 in 1 000 000, classically described as a thrombophlebitis of the internal jugular vein (IJV) secondary to an oropharyngeal infection. It is usually seen among the adolescent and young adult populations [1]. A rare and often initially overlooked disease, LS can have mortality rates of over 90% if left untreated [2]. Even treated cases have a mortality rate of 5–18% in the advanced stages [1]. It is not yet known whether there are any predisposing conditions that can make a person susceptible to acquiring this disease. As our case shows, one such condition could be polycythemia vera (PV). It is a neoplastic proliferation of red blood cells, known to cause hyperviscosity of the blood along with thrombocytosis, and is associated with an increased risk of arterial and venous thrombosis [3–5]. In PV, thrombotic events manifest most commonly as deep vein thrombosis (27.8%), acute coronary syndrome (27.8%), and stroke (24.5%) [6]. To the best of our knowledge, this report is the first to demonstrate LS in a polycythemia vera patient.
Case Report
A 66-year-old woman with a past medical history of paroxysmal atrial fibrillation (PAF) and PV presented to the Emergency Department (ED) for worsening right-sided neck pain for 4 days, associated with intermittent rigors and chills. The pain was also accompanied with trismus and odynophagia, as a result of which she was unable to eat or drink. The patient denied any recent fevers, trauma, or dental procedures. One day prior to presentation, she was seen by an otolaryngologist, who had prescribed antibiotics in hopes of treating a suspected dental infection. The patient also reported that she was not compliant with her aspirin (prescribed by a hematologist as a measure against thrombosis in PV) or apixaban (for PAF) and was managing her PV exclusively by therapeutic phlebotomy every 3–4 months. On arrival to the ED, she was afebrile, with other vital signs within normal limits. On the initial encounter, a physical examination revealed a nontoxic-appearing middle aged woman who was alert and oriented to time, place, and person. Inspection of the neck showed a swelling, noted just below the right mandibular angle, with associated erythema of the skin. On palpation, tenderness was elicited over the entire right sternocleidomastoid region, but no palpable lymphadenopathy, fluctuance, or abscess was discovered. Trismus was noted on the affected side, with inability to fully open the mouth due to pain. Examination of the oral cavity revealed poor oral dentition, multiple caries, and mild erythema of the posterior pharyngeal mucosa, with non-erythematous tonsils, without any exudate. Results of pulmonary and cardiovascular examinations were unremarkable.
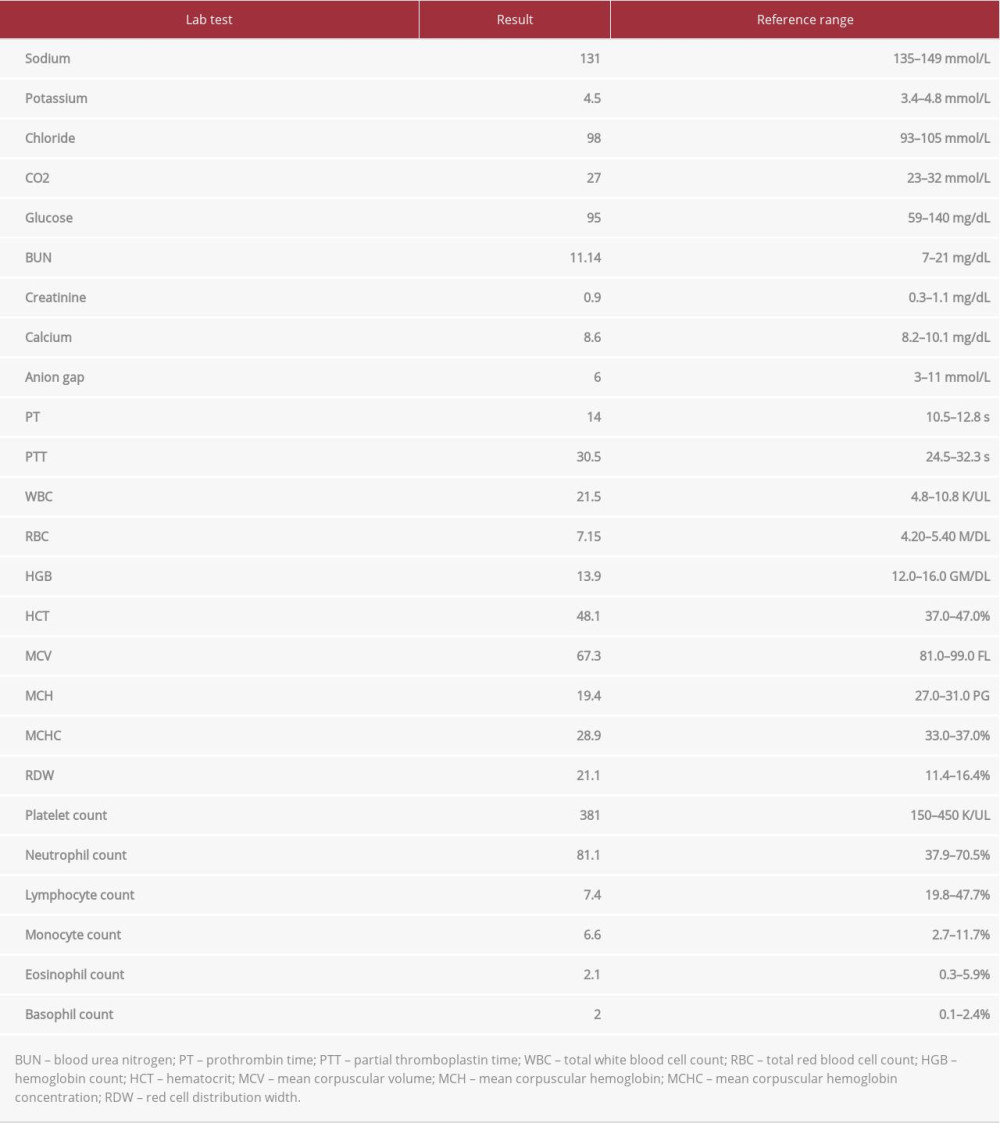
Her initial complete blood count revealed a total white blood cell count of 21 500/mm3, with a differential count showing 81.1% neutrophils, hemoglobin of 13.9 g/dL, hematocrit 48.1%, and platelet count of 381 000/uL (Table 1). The comprehensive metabolic panel showed electrolytes and kidney function were within normal reference ranges (Table 1). Throat and blood cultures did not grow any organisms. Computed tomography with i.v. contrast of the neck showed complete thrombosis of the right internal jugular vein, extending into the superior portion of the SVC, with partial occlusion of the superior segment of the superior vena cava at the junction of the right subclavian and right internal jugular veins (Figure 1).
Keeping in mind the clinical presentation coupled with the laboratory and imaging data, the patient was diagnosed with Lemierre’s syndrome and was admitted for treatment with i.v. antibiotics and anticoagulation. She was treated with therapeutic doses of enoxaparin and also received i.v. metronidazole and ceftriaxone. During the course of her stay, she remained afebrile and her symptoms improved rapidly, with excellent resolution of her swelling within 24 h and return of ability to chew and swallow adequately. She was eventually discharged on apixaban and clindamycin and was encouraged to maintain compliance with her medications and to follow up regularly with her hematologist. On speaking to the patient 3 months after discharge, we learned that she was advised by both her hematologist and cardiologist (for PAF) to continue apixaban therapy indefinitely to prevent the possibility of further thrombotic events resulting from PV or PAF.
Discussion
Conventionally, clinical diagnosis of LS is based on 3 criteria: (1) history of a head or neck infection, (2) thrombosis or thrombophlebitis of a head or neck vein, or metastatic lesions, and (3) isolation of
Interestingly, our patient was not in the age group in which LS is usually seen (19–22 years) [1]. Additionally, although she had poor orodental hygiene, she did not have any obvious neck infection on clinical exam or on CT imaging. She was also afebrile, with sterile throat and blood cultures. However, it is difficult to completely rule out oral infection since she was already on antibiotics for 1 day before presenting to us. Given this clinical profile, it is reasonable to say that she had an interesting presentation of LS, which makes us wonder if it is important to consider the role of polycythemia vera as a risk factor in her development of LS. There is evidence of a 20–50% chance of thrombotic events in PV patients [8], but to the best of our knowledge there are no reported cases of LS or IJV thrombosis with PV.
Her predisposition to thrombosis in the setting of PV may also be due to certain risk factors specific to PV, such as age >60 years old and with elevated hematocrit [9]. PV patients can reduce the risk of thrombosis by keeping the hematocrit below 45% [9], but our patient’s hematocrit upon admission was 48.1%. Another factor, leukocytosis, also poses a major risk for thrombosis in PV patients [9,10], and our patient’s WBC count was initially 21 500 and reached a maximum of 30 300 on day 2 of hospitalization.
Low-dose aspirin has been shown to decrease the risk of thrombosis among PV patients [11]. It is also noteworthy that our patient discontinued her low-dose aspirin for 2 weeks before this event, subjecting her to a hypercoagulable state. An analysis of this patient’s many risk factors is summarized in Figure 2.
Standard management of LS includes prompt empiric therapy with an i.v. beta-lactamase-resistant beta lactam antibiotic for coverage of
A recent meta-analysis by Adedeji et al reported that anticoagulation among LS patients is both safe and efficacious with DOACs (direct oral anticoagulants) for a suggested duration of 6–12 weeks [12]. However, among all cases included in the meta-analyses, the initial anticoagulation therapy was parenteral (heparin, Lovenox, or fondaparinux) while the patient was in the hospital [12].
Conclusions
PV predisposes patients to a hyper-viscous and prothrombotic state, which may warrant a stronger suspicion of Lemierre’s disease in symptomatic presentations. In addition, lack of aspirin use for prophylaxis of thrombosis and undiagnosed oral infection are factors to consider when assessing risk factors for Lemierre’s syndrome in PV patients. However, further research is needed to confirm this suspicion, which may be a challenge given the rarity of LS.
Figures
References:
1.. Allen BW, Anjum F, Bentley TP: Lemierre syndrome, StatPearls Published December 4, 2020. Accessed May 16, 2021https//www.ncbi.nlm.nih.gov/books/NBK499846/
2.. Coultas JA, Bodasing N, Horrocks P, Cadwgan A, Lemierre’s syndrome: Recognising a typical presentation of a rare condition: Case Rep Infect Dis, 2015; 2015; 797415
3.. Barbui T, Carobbio A, Rumi E, In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology: Blood, 2014; 124(19); 3021-23
4.. Marchioli R, Finazzi G, Landolfi R, Vascular and neoplastic risk in a large cohort of patients with polycythemia vera: J Clin Oncol, 2005; 23(10); 2224-32
5.. Marchioli R, Finazzi G, Specchia G, Cardiovascular events and intensity of treatment in polycythemia vera: N Engl J Med, 2013; 368(1); 22-33
6.. Kaifie A, Kirschner M, Wolf D, Bleeding, thrombosis, and anticoagulation in myeloproliferative neoplasms (MPN): Analysis from the German SAL-MPN-registry: J Hematol Oncol, 2016; 9; 18
7.. Valerio L, Corsi G, Sebastian T, Barco S, Lemierre syndrome: Current evidence and rationale of the Bacteria-Associated Thrombosis, Thrombophlebitis and Lemierre syndrome (BATTLE) registry: Thromb Res, 2020; 196; 494-99
8.. Pearson TC, The risk of thrombosis in essential thrombocythemia and polycythemia vera: Semin Oncol, 2002; 29(3 Suppl. 10); 16-21
9.. Griesshammer M, Kiladjian JJ, Besses C, Thromboembolic events in polycythemia vera: Ann Hematol, 2019; 98(5); 1071-82
10.. Landolfi R, Di Gennaro L, Barbui T, Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera: Blood, 2006; 109(6); 2446-52
11.. Landolfi R, Marchioli R, Kutti J, Efficacy and safety of low-dose aspirin in polycythemia vera: N Engl J Med, 2004; 350(2); 114-24
12.. Adedeji A, Chukwura O, Obafemi T, Anticoagulation strategies in the management of Lemierre syndrome: A systematic review of the literature: Ann Pharmacother, 2021; 55(5); 658-65
Figures
In Press
16 Mar 2024 : Case report ")
Am J Case Rep In Press; DOI: 10.12659/AJCR.943214
16 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943010
16 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943687
17 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943070
Most Viewed Current Articles
07 Mar 2024 : Case report
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report 
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250