17 January 2022: Articles 
Severe Anion Gap Metabolic Acidosis Resulting from Combined Chronic Acetaminophen Toxicity and Starvation Ketosis: A Case Report
Challenging differential diagnosis, Adverse events of drug therapy, Rare coexistence of disease or pathology
Thomas Kalinoski1ABCDEF*DOI: 10.12659/AJCR.934410
Am J Case Rep 2022; 23:e934410






Abstract
BACKGROUND: Chronic acetaminophen toxicity has been known to cause an anion gap metabolic acidosis (AGMA) due to accumulation of 5-oxoproline metabolites. This diagnosis requires a high index of suspicion when evaluating a patient with AGMA as occasional acetaminophen use is very common among patients, whom oftentimes are not entirely truthful about the extent of ingestion and have multiple comorbid conditions complicating diagnosis.
CASE REPORT: A 68-year-old male with multiple medical comorbidities presented to the emergency room with recurrent generalized weakness. On all occasions the patient denies focal weakness or infectious symptoms. The patient also denies ingestions other than his routine prescribed medications, including acetaminophen 325mg as needed, which he describes taking “a couple times” a day. His prior visits were notable for profound anion-gap metabolic acidosis, hypernatremia, acute kidney injury, and positive urine ketones. As the patient’s blood urea nitrogen (BUN), blood sugar, liver function tests, lactic acid, and serum osmolality were normal, the patient received a diagnosis of “starvation ketosis” and received supportive care each time. Further investigation at his final admission revealed an extremely elevated 5-oxoproline level revealing a delayed diagnosis of chronic acetaminophen toxicity
CONCLUSIONS: This report emphasizes the need for a high index of suspicion related to chronic acetaminophen toxicity and other ingestions contributing to a metabolic acidosis in at-risk populations, even when routine history is unrevealing. Furthermore, severe acidosis should prompt more extensive investigation when out of proportion to obvious routine etiologies.
Keywords: Acetaminophen, Acid-Base Equilibrium, ketosis, Acidosis, Analgesics, Non-Narcotic, Humans, Male
Background
Metabolic acidosis results from a reduction in serum bicarbonate concentration, with a usual secondary drop in arterial carbon dioxide concentration and reduction in blood pH [1]. Metabolic acidosis often results from the overproduction of organic acids, resulting in an elevated serum anion gap. This is defined as the sum of serum chloride and bicarbonate concentrations subtracted from the serum sodium concentration, with the upper limit of normal dependent on the laboratory [1,2]. Anion-gap metabolic acidosis (AGMA) commonly results from a decreased clearance of organic acids in chronic renal failure. Another often seen condition causing AGMA is lactic acidosis, resulting from an overproduction or decreased clearance of L-lactate in conditions such as sepsis or liver failure or excess accumulation of D-lactate in short-gut syndrome. This condition can also result from increased production of keto-acids seen in the conditions diabetic and alcoholic ketoacidosis and starvation ketosis. Starvation ketosis AGMA includes ingestion of exogenous organic acids (eg, methanol, glycols, and salicylates) and the most recently recognized 5-oxopro-line, a metabolite of acetaminophen [2,3].
Case Report
A 68-year-old man with a history of myelodysplastic syndrome, cerebrovascular accident, prostate cancer, chronic low back pain, hypertension, and depression presented to the Emergency Department (ED) with recurrent generalized weakness. The patient had been seen in the ED 3 times prior in the past 6 months for the same clinical presentation. The patient had associated mild confusion, but no new focal weakness or other neurologic changes were apparent by history and neurological examination at each of these visits, and an infectious evaluation was unremarkable. The weakness was of insidious onset each time, with gradual decline over several weeks. He denied any history of alcohol or drug use and denied any ingestions other than his prescribed medications. Of note, the patient was prescribed acetaminophen 325 mg as needed, which he described taking “1 to 2 pills a couple times a day.”
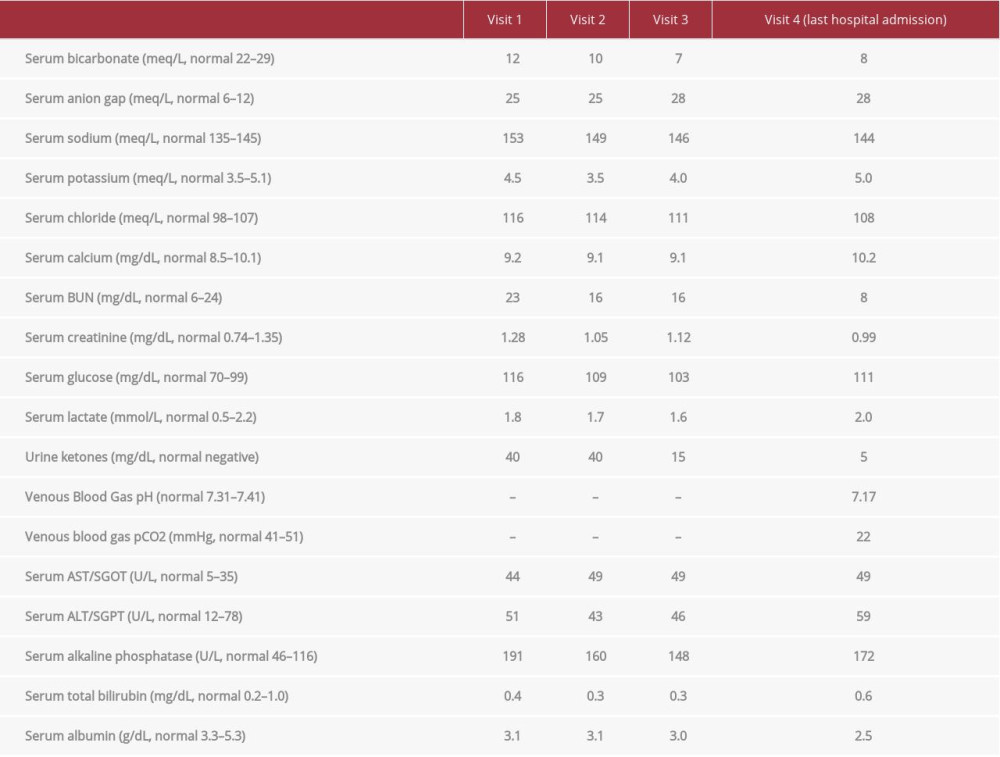
The patient was found to have anion gap metabolic acidosis at each of these visits, with a serum bicarbonate as low as 7 meq/L, anion gap as high as 28 meq/L, and a venous blood gas pH of 7.17 with a pCO2 of 22 mmHg. His laboratory studies were also notable for varying degrees of hypernatremia up to 153 meq/L and acute kidney injuries, with up to 0.4 mg/dL creatinine elevation above his baseline. On these occasions, urine ketones were variably elevated (as high as 40 mg/dL), although serum beta-hydroxybutyrate was normal when checked at his last presentation. At every visit, the patient’s serum lactate was within the reference range of less than or equal to 2.0 mmol/L, as were his blood urea nitrogen (BUN), blood sugar, liver function tests, and serum osmolality (Table 1).
Upon each visit to the ED, the patient was admitted to the hospital for further management. The patient was diagnosed with starvation ketosis at one of the visits, assuming that his positive urine ketones were at least in part related to his acidosis.
Other hospitalizations arrived at no definitive diagnosis. With each hospitalization, however, the patient did improve, both symptomatically and by laboratory evaluation, with the administration of intravenous fluids (usually 5% dextrose with 0.45% sodium chloride) over 2 to 3 days. The patient was always discharged home with primary care follow-up.
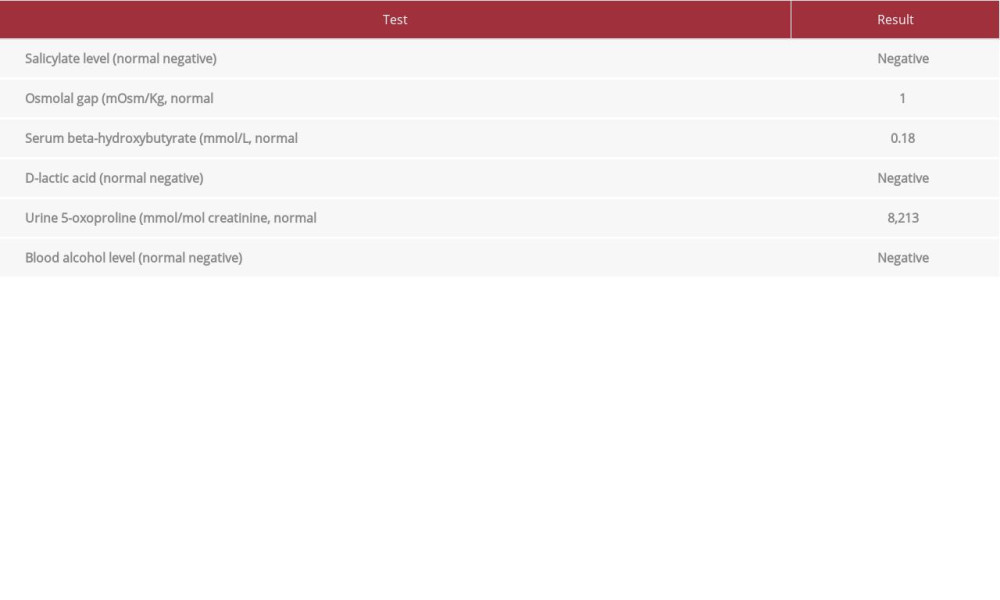
At the most recent presentation, the patient’s vital signs were normal, other than tachypnea to 28 breaths/min. The physical examination was notable for Kussmaul breathing pattern and slight confusion; otherwise, the cardiopulmonary and neurologic examinations were normal. He was found to have a serum bicarbonate level of 8 meq/L, anion gap of 28 meq/L, pH of 7.20, and sodium of 140 meq/L. His lactic acid level was 2.0 mmol/L, serum osmolality was 290 mOsm/kg (with an osmolal gap of 1.0 mOsm/kg), and urine ketones were 5 mg/dL, with a serum beta-hydroxybutyrate level normal at 0.18 mmol/L. His electrocardiogram revealed normal sinus rhythm. On admission, further analysis revealed a salicylate level of less than 5.0 mg/ dL, a negative D-lactic acid and blood alcohol level, but a urine 5-oxoproline level of 8213 mmol/mol creatinine, with the reference range <62 mmol/mol creatinine (Table 2). The latter 2 tests required samples to be sent to a specialized outside laboratory. The patient’s acetaminophen was held, and he was counseled extensively on cessation of use, with alternatives agents proposed for pain control. The patient’s acidosis corrected with removal of the offending agent and administration of intravenous 5% dextrose with sodium bicarbonate over 3 days. The patient’s mental status and breathing returned to normal by the second day of hospitalization. The patient’s generalized weakness improved, although it was not back to baseline at the end of hospitalization 1 week later, and he was discharged to a swing bed facility for further rehabilitation.
Discussion
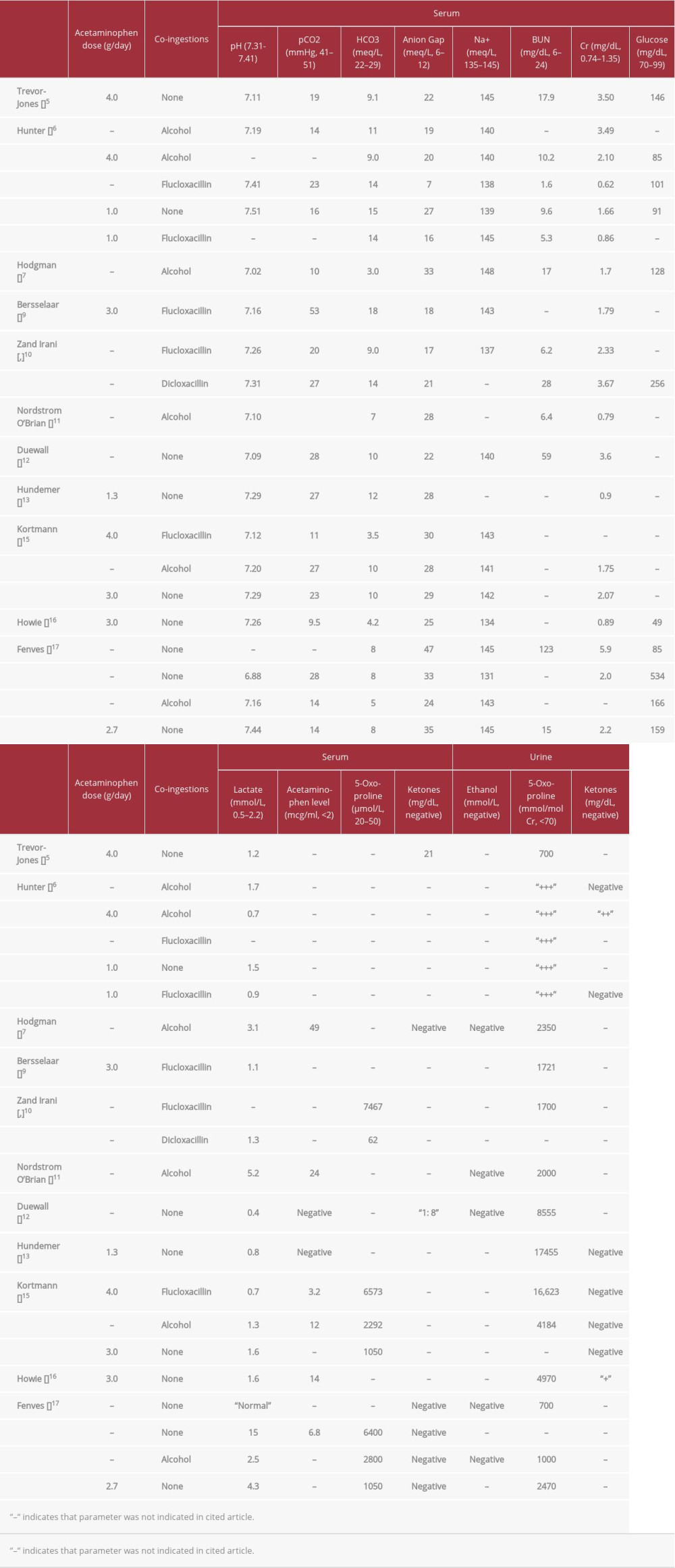
Acquired 5-oxoproline toxicity was first recognized in association with chronic acetaminophen ingestion and anion gap metabolic acidosis in 1990, although the diagnosis remains challenging in part owing to patient reliability and lack of test availability [4]. In the cases reported in the literature, patients shared a history of chronic acetaminophen ingestion, although not at doses usually considered toxic (Table 3). Interestingly, the doses of the reviewed cases, when known, were all under 4 g of acetaminophen total per day [5,6,9,13,15,16], and acetaminophen levels were not in the toxic range [4,5,11–13,15–17]. Some of these patients had an increased risk for acetaminophen toxicity with the concomitant use of alcohol or penicillins, but excluding these cases, the most common risk factors included advanced age, female sex, malnutrition, kidney dys-function, and/or multiple chronic illnesses [4–17]. The common thread uniting all of these risks is thought to be glutathione depletion or relative deficiency [4].
Of the cases reviewed, toxic encephalopathy was the most common presenting symptom, although many patients remained asymptomatic [5–17]. All had varying levels of AGMA and diagnosis achieved through urinary or plasma 5-oxoproline levels. Patients generally had low or negative lactic acid and BUN levels. No patients were reported to have hypernatremia, and only 2 patients had concomitant ketosis diagnosed through urine studies [6,12].
Other than female sex and other drug or substance use, our patient encompassed all of the risk factors described above. Although he did not report excess acetaminophen use, he was at risk for chronic toxicity due to these comorbidities. What made this case more challenging was the ketosis observed on 3 out of 4 urinalysis specimens. As the patient’s blood glucose was normal, he denied alcohol use, and was not on an SGLT2 inhibitor, this finding was diagnosed as starvation ketosis. The ketosis, as well as the patient’s documented hyper-natremia, were likely in part a result of unattainable hydration and nutrition brought on by his encephalopathy and profound weakness while acetaminophen toxic. As such, these laboratory abnormalities may have been an indirect consequence of his acetaminophen ingestion. However, as it is thought that chronic malnutrition can be a risk factor for acetaminophen toxicity, the relationship can go both ways, and this patient’s clinical picture may have been multifactorial [4]. While certainly contributing to this patient’s acidosis, starvation ketosis is not usually expected to produce a profound acidosis to the degree seen in this patient [18], and thus, an exploration of other contributing factors was necessary. A possible way to infer the presence of 5-hydroxyproline toxicity would be to obtain urinary electrolytes to calculate a urine anion gap. However, the presence of other organic ions with this patient’s known ketosis may have lowered the diagnostic utility in this case, and urinary electrolytes were unfortunately not collected.
Conclusions
Acquired 5-oxoproline toxicity related to chronic acetaminophen ingestion is an increasingly recognized etiology of AGMA. As the risk factors related to chronic acetaminophen toxicity, even at moderate doses, often overlap with those causing starvation ketosis, co-occurrence is possible, and a high index of suspicion is required to make the diagnosis.
References:
1.. Kraut J, Madias N, Metabolic acidosis: Pathophysiology, diagnosis, and management: Nat Rev Nephrol, 2010; 6(5); 274-85
2.. Kraut J, Madias N, Serum anion gap: Its uses and limitations in clinical medicine: Clin J Am Soc Nephrol, 2007; 2; 162-74
3.. Vichot A, Rastegar A, Use of anion gap in the evaluation of a patient with metabolic acidosis: Am J Kidney Dis, 2014; 64(4); 653-57
4.. Emmett M, Acetaminophen toxicity and 5-oxoproline (pyroglutamic acid): A tale of two cycles, one an ATP-depleting futile cycle and the other a useful cycle: Clin J Am Soc Nephrol, 2014; 9; 191-200
5.. Trevor-Jones E, Hughes L, Lessons of the month: Pyroglutamic acidosis: Long-term paracetamol and a high anion gap: Clin Med, 2020; 20(5); 522-23
6.. Hunter R, Lawson C, Pyroglutamic acidosis in association with therapeutic paracetamol use: Clin Med, 2016; 16(6); 524-29
7.. Hodgman M, Horn J, Profound metabolic acidosis and oxoprolinuria in an adult: J Med Toxicol, 2007; 3(3); 119-24
8.. Raibman Spector S, Mayan H, Pyroglutamic acidosis as a cause for high anion gap metabolic acidosis: A prospective study: Sci Rep, 2019; 9; 3554
9.. Bersselaar LR, Brule JMD, Acetaminophen use concomitant with long-lasting flucloxacillin therapy: A dangerous combination: Eur J Case Rep Intern Med, 2020; 7(7); 001569
10.. Zand Irani A, Borchert G, Flucloxacillin and paracetamol induced pyroglutamic acidosis: BMJ Case Rep, 2021; 14(1); e237536
11.. Nordstrom O’Brien LM, Hooper M, Chronic acetaminophen ingestion resulting in severe anion gap metabolic acidosis secondary to 5-oxoproline accumulation: An under-diagnosed phenomenon: BMJ Case Rep, 2012; 2012; bcrbcr032012602
12.. Duewall J, Fenves A, 5-Oxoproline (pyroglutamic) acidosis associated with chronic acetaminophen use: Proc (Bayl Univ Med Cent), 2010; 23(1); 19-20
13.. Hundemer G, Fenves A, Acquired 5-oxoproline acidemia successfully treated with N-acetylcysteine: Proc (Bayl Univ Med Cent), 2017; 30(2); 169-70
14.. Zand Irani A, Almuwais A, Acquired pyroglutamic acidosis due to long-term dicloxacillin and paracetamol use: BMJ Case Rep, 2020; 13; e233306
15.. Kortmann W, Agtmael MA, 5-Oxoproline as a cause of high anion gap metabolic acidosis: An uncommon cause with common risk factors: Neth J Med, 2008; 66(8); 354-57
16.. Howie S, Tarn A, A not so simple analgesic: NDT Plus, 2010; 3; 573-75
17.. Fenves A, Kirkpatrick H, Increased anion gap metabolic acidosis as a result of 5-oxoproline (pyroglutamic acid): A role for acetaminophen: Clin J Am Soc Nephrol, 2006; 1; 441-47
18.. Palmer BF, Clegg DJ, Starvation ketosis and the kidney: Am J Nephrol, 2021; 52(6); 467-78
In Press
06 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.942937
12 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943244
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943275
13 Mar 2024 : Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.943411
Most Viewed Current Articles
07 Mar 2024 : Case report
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
10 Jan 2022 : Case report 
DOI :10.12659/AJCR.935263
Am J Case Rep 2022; 23:e935263
19 Jul 2022 : Case report
DOI :10.12659/AJCR.936128
Am J Case Rep 2022; 23:e936128
23 Feb 2022 : Case report
DOI :10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250