23 February 2022: Articles 
Penile Necrosis Associated with Local Intravenous Injection of Cocaine
Challenging differential diagnosis, Rare disease
Haider Ghazanfar1ABCDEF*, Paola Valeria Espinosa1ABCDEF, Cosmina Zeana2ABCDEF, Sridhar Chilimuri1ABCDEF, Donald Rudikoff3ABCDEFDOI: 10.12659/AJCR.935250
Am J Case Rep 2022; 23:e935250






Abstract
BACKGROUND: Cocaine is a highly addictive drug and its use has increased in recent years. It is the second most popular illicit drug in the United States and is the second most trafficked illicit drug in the world. Intravenous (i.v.) drug use leads to severe injury to the veins, including erythema, thrombophlebitis, vasoconstriction, necrosis, development of venous ulceration, and vein occlusion.
CASE REPORT: A 35-year-old man presented to our Emergency Department with a 3-day history of excruciating and progressive penile and scrotal pain after having injected cocaine in the dorsal vein of the penis. A genital examination revealed ulcerations and swelling on the ventral proximal penis and scrotum junction, with foul-smelling serous discharge. There was no crepitus. He also had stellate purpura with necrosis of the dorsum of the penis and tender bilateral inguinal lymphadenopathy. Computed tomography of the pelvis, with contrast, showed subcutaneous edema of the penis with ulceration of the penile tip on the right. It also revealed left inguinal adenopathy. Vasculitis and concomitant sexually transmitted disease were ruled out as well as Fournier gangrene, and he was started on i.v. broad-spectrum antibiotics. The patient’s clinical condition improved with antibiotics and local wound care.
CONCLUSIONS: Our case highlights the importance of taking a thorough history from i.v. drug users, as they are at risk of injecting drugs into unusual sites, such as the dorsal penile vein. It is important for the physician to counsel active i.v. drug users regarding possible complications of injecting drug into unusual sites.
Keywords: Cocaine, Levamisole, Necrosis, Substance Abuse Detection, adult, Genital Diseases, Male, Humans, Injections, Intravenous, Male, Penile Diseases
Background
Cocaine is a highly addictive drug, and its use has progressively increased in recent years [1]. It is the second most popular illicit drug used in the United States and is the second most trafficked illicit drug in the world. According to the Centers for Disease Control and Prevention, cocaine accounted for 1 in 5 fatal drug overdoses and resulted in 14 665 drug overdose deaths in 2018 [1]. About 5.1% of European adults have tried cocaine during their lifetime [2]. Cocaine use has increased by 30% per year in adults between the ages of 25 and 64 years [1]. According to a study using 2 national United States data sources, 63.78% of cocaine users are male [3]. Studies have indicated that cocaine use is most prevalent in ages 15 to 35 years. Its use has been reported to be more common in Hispanic individuals, but drug overdose deaths are highest in the non-Hispanic Black population [3].
Intravenous (i.v.) drug use leads to severe injury to the veins, including erythema, thrombophlebitis, vasoconstriction, necrosis, development of venous ulceration, and vein occlusion [4]. Intravenous drug users are 35 times more likely to develop chronic venous disorders than are individuals who never injected i.v. drugs [5].
Cocaine is a sympathomimetic agent that causes central and peripheral adrenergic stimulation by blocking norepinephrine and dopamine presynaptic reuptake. This leads to increased norepinephrine levels, which in turn cause vasoconstriction of the cardiac and peripheral vasculature. Cocaine also causes severe vasoconstriction by direct alpha-adrenergic stimulation [6]. We present a case of a 35-year-old Hispanic man who presented with progressive penile and scrotal pain after injecting cocaine into the dorsal vein of the penis.
Case Report
A 35-year-old Hispanic man presented to our Emergency Department with a 3-day history of excruciating and progressive penile and scrotal pain after having injected cocaine into the dorsal vein of the penis. He had immediate severe pain radiating to the inguinal region and right foot, accompanied by swelling and blanching of the dorsal aspect of the penis and necrosis and ulceration of the lateral aspect. His past medical history was significant for previous i.v. drug use. He stated that he had previously injected cocaine in the dorsal vein at least 2 times in the past 2 weeks without any complications.
On initial assessment, the patient was stable (temperature 37°C, heart rate 86 beats/per/min, blood pressure 117/63 mmHg). He was oriented to time, place, and person. He had bilateral vesicular breathing on lung auscultation. The cardiac examination revealed normal S1 and S2 heart sounds. Abdominal examination showed no hepatosplenomegaly. The neurological examination was unremarkable. The genital examination revealed ulceration and swelling on the ventral proximal penis and scrotum junction with foul-smelling serous discharge. There was no crepitus. He also had stellate purpura with necrosis of the dorsum of the penis and tender bilateral inguinal lymphadenopathy (Figures 1–3).
He had a white blood cell count of 11.9 g/dL, erythrocyte sedimentation rate of 43.0 mm/h, and C-reactive protein level of 52.71 mg/L. The liver function tests and electrolytes were normal. Computed tomography (CT) of the pelvis performed with contrast showed subcutaneous edema of the penis, with ulceration of the penile tip on the right. It also revealed left inguinal adenopathy, with nodes measuring up to 1.7 cm, which was presumably reactive (Figure 4).
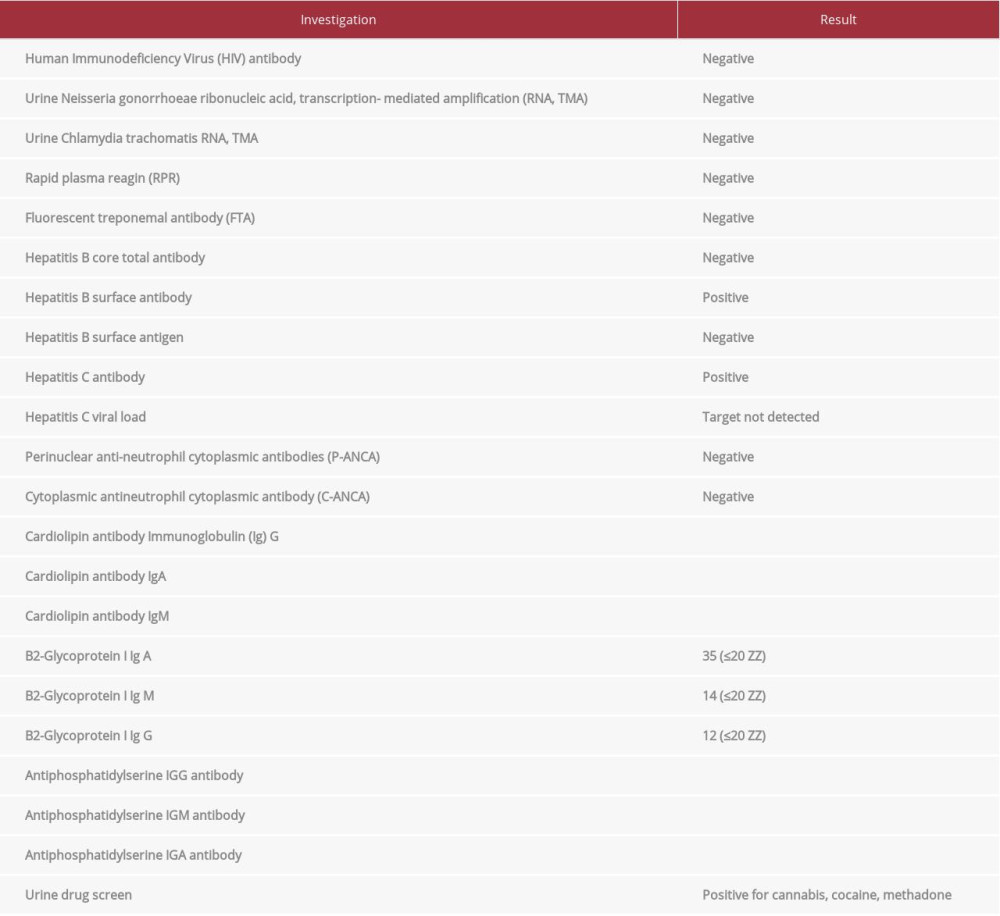
Fournier gangrene was ruled out, and he was started on i.v. piperacillin-tazobactam 3.375 g every 6 h, vancomycin 1.5 g every 12 h, clindamycin 300 mg every 8 h, and topical bacitracin/polymyxin 1 application every 6 h. He refused any surgical debridement. His clinical condition improved slowly with antibiotics and local wound care. A blood culture showed no growth. Vasculitis and concomitant sexually transmitted diseases were ruled out (Table 1).
After 5 days of treatment, i.v. antibiotics were changed to oral trimethoprim-sulfamethoxazole and amoxicillin-clavulanate to complete a total course of 10 days. His clinical condition improved, but he refused to go for drug rehabilitation treatment and was later lost to follow-up.
Discussion
As the potential for dependence and addiction is high, cocaine is one of the most dangerous drugs available. Drug users often use new injection sites once their primary site becomes damaged and unavailable. Older age at first drug use (odds ratio [OR] 1.039, 95% confidence interval [CI] 1.009–1.069), longer injection duration (OR 1.071, 95% CI 1.041–1.102), and greater injection frequency (OR 1.255, 95% CI 1.072–1.471) are all associated with a higher likelihood of using injection sites other than those on the arms [4]. Our patient had a long history of i.v. drug use which had led to damage to more accessible injection sites; therefore, he had started using alternative injection sites, such as the dorsal penile vein. Cocaine use can also provoke the development of vasculitis, which can result in gangrene. Cocaine use in the groin area has been linked to Fournier’s gangrene [7], superficial penile necrosis [8], and scrotal gangrene [9]. Cocaine can affect the skin of the genital area, regardless of the route of cocaine administration or what type of vascular complication occurs [10]. Our patient presented with penile necrosis after local i.v. injection of cocaine.
Adulteration of cocaine with the anthelmintic levamisole is also common. According to the US Drug Enforcement Agency, approximately 80% of the cocaine seized in the United States is adulterated with levamisole [11]. The addition of levamisole to cocaine increases profitability and enhances cocaine’s effects [12]. Levamisole has been shown to inhibit monoamine oxidase and catechol-0 methyltransferase activity, which leads to an increased level of catecholamine neurotransmitter in nerve synapses, further enhancing the effects of cocaine [13]. Levamisole has also been linked to the development of necrotizing vasculitis. Levamisole-induced vasculitis presents as retiform purpuric lesions that become necrotic, as compared with palpable purpura or Wegener’s granulomatosis-like lesions in pure cocaine-induced vasculitis [14]. Levamisole has a short half-life of 5.6 h; and therefore, testing its level in blood or urine within 48 h of last use has been recommended [15]. Cytoplasmic anti-neutrophilneutrophil cytoplasmic antibody and perinuclear anti-neutrophil cytoplasmic antibodies are usually positive in patients with levamisole-induced vasculitis [15].
Studies have shown that levamisole use is also associated with anticardiolipin antibodies and decreased serum complement component 3 levels [16]. Perinuclear anti-neutrophil cytoplasmic antibodies, cytoplasmic antineutrophilneutrophil cytoplasmic antibodies, and anticardiolipin antibodies were negative in our patient.
Based on the high prevalence of adulteration of cocaine with levamisole, an attempt to rule out levamisole-induced vasculitis was made. Because our patient presented after 48 h and the test was not available in our laboratory, serum or urine levels of levamisole were not sent.
Our patient improved with antibiotics and wound care and was discharged with outpatient appointments, but unfortunately, he was lost to follow-up. Intravenous drug users should be counseled to seek help and should be advised to enroll in drug rehabilitation programs, as cocaine cessation is the only definitive treatment.
Conclusions
Our case highlights the importance of taking a thorough history from i.v. drug users, as they are at risk of injecting drugs into unusual sites, such as the dorsal penile vein. It is important for the physician to counsel active i.v. drug users regarding possible complications of injecting drugs in atypical and dangerous injection sites.
Figures
References:
1.. , Increase in Drug Overdose Deaths Involving Cocaine: United States, 2009–2018 [cited 2021 June 15]; Available from https://wwwcdcgov/nchs/products/databriefs/db384.htm
2.. , European Drug Report 2018: Trend Developments [cited 2021 June 15]. Available from: http://www.emcdda.europa.eu/system/files/publications/8585/20181816_TDAT18001ENN_PDF.pdf
3.. Cano M, Oh S, Salas-Wright CP, Vaughn MG, Cocaine use and overdose mortality in the United States: Evidence from two national data sources, 2002–2018: Drug Alcohol Depend, 2020; 214; 108148
4.. Karimi M, Ghaheri H, Assari S, Drug injection to sites other than arm: A study of Iranian heroin injectors: Front Psychiatry, 2014; 5; 23
5.. Pieper B, Templin TN, Kirsner RS, Birk TJ, Impact of injection drug use on distribution and severity of chronic venous disorders: Wound Repair Regen, 2009; 17(4); 485-91
6.. Gurudevan SV, Nelson MD, Rader F, Cocaine-induced vasoconstriction in the human coronary microcirculation: New evidence from myocar-dial contrast echocardiography: Circulation, 2013; 128(6); 598-604
7.. Mouraviev VB, Pautler SE, Hayman WP, Fournier’s gangrene following pe-nile self-injection with cocaine: Scand J Urol Nephrol, 2002; 36; 317-18
8.. Carey F, Dinsmore WW, Cocaine-induced penile necrosis: Int J STD AIDS, 2004; 15; 424-25
9.. Chen SC, Jang MY, Wang CS, Cocaine-related vasculitis causing scrotal gangrene: Ann Pharmacother, 2009; 43(2); 375-78
10.. Chen SC, Jang MY, Wang CS, Cocaine-related vasculitis causing scrotal gangrene: Ann Pharmacother, 2009; 43; 375-78
11.. Wolford A, McDonald TS, Eng H, Immune-mediated agranulocytosis caused by the cocaine adulterant levamisole: A case for reactive metabolite(s) involvement: Drug Metab Dispos, 2012; 40; 1067-75
12.. Tallarida CS, Egan E, Alejo GD, Levamisole and cocaine synergism: A prevalent adulterant enhances cocaine’s action in vivo: Neuropharmacology, 2014; 79; 590-95
13.. Levandoski MM, Piket B, Chang J, The anthelmintic levamisole is an allosteric modulator of human neuronal nicotinic acetylcholine receptors: Eur J Pharmacol, 2003; 471; 9-20
14.. Friedman DR, Wolfsthal SD, Cocaine-induced pseudovasculitis: Mayo Clin Proc, 2005; 80(5); 671-73
15.. Sánchez-Cruz A, Marrero S, Betancourt J, Cocaine induced vasculitis: Have we found a culprit?: Case Rep Rheumatol, 2012; 2012; 982361
16.. Garg L, Gupta S, Swami A, Zhang P, Levamisole/cocaine induced systemic vasculitis and immune complex glomerulonephritis: Case Rep Nephrol, 2015; 2015; 372413
17.. George TC, Freet DJ, Cross JM, Huzar TF, Levamisole-induced vasculitis: J Am Acad Physician Assist, 2019; 32(1); 23-27
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953007
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953581
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952507
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952041
Most Viewed Current Articles
07 Dec 2021 : Case report
22,760,669
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,388
176,388
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,720
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,753
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133