10 July 2020: Articles 
Total Pancreatectomy with Splenectomy for Multifocal Intraductal Tubulopapillary Neoplasm (ITPN) of the Pancreas Associated with Invasive Component: Report of a Rare Case
Challenging differential diagnosis, Rare disease
Christoforos Kosmidis1ACDF, Nikolaos Varsamis1ABCDEFG*, Stefanos Atmatzidis2BCDF, Georgios Koimtzis2ACF, Stylianos Mantalovas2ACF, Georgios Anthimidis1ADF, Eleni Georgakoudi3AC, Christina D. Sevva4FG, Katerina Zarampouka5BCD, Danai Chourmouzi6BCD, Ariadni Leptopoulou7AD, Sofia Baka3ACD, Maria Kosmidou8DFDOI: 10.12659/AJCR.924760
Am J Case Rep 2020; 21:e924760






Abstract
BACKGROUND: Pancreatic intraductal tubulopapillary neoplasm (ITPN) was first described by Yamaguchi in 2009 and was recognized by World Health Organization as a distinct entity in 2010. Since then few case reports and case series have been published. Little is known about its clinicopathologic features and treatment outcomes. We present the seventh case of total pancreatectomy for ITPN reported in the English literature.
CASE REPORT: Our patient was an 82-year-old male with a previous history of acute evolving-to-chronic pancreatitis. After 2 years of medical consultation, an abdominal magnetic resonance imaging was suspicious for multifocal pancreatic neoplasia. A computed tomography-guided biopsy of the lesion was performed which indicated pancreatic intraductal neoplasia with intermediate dysplasia. After oncology consultation, the patient underwent pylorus-preserving total pancreatectomy with splenectomy. The pathology report showed pancreatic ITPN with intermediate to severe dysplasia and associated invasive carcinoma. All 21 resected lymph nodes were non-metastatic (pT3N0). The postoperative course of the patient was uncomplicated. He received adjuvant gemcitabine (single agent) for 6 months. At 18 months after surgery he was diagnosed with hepatic metastases; he was still alive at the time of this reporting.
CONCLUSIONS: ITPN has been associated with previous history of acute pancreatitis in some patients. Early diagnosis, radical surgical resection, and adjuvant chemotherapy may lead to long-term survival rates even in cases with associated invasive component. Total pancreatectomy may be a preferable procedure for ITPN in selected patients.
Keywords: Carcinoma, Intraductal, Noninfiltrating, Pancreatectomy, Pancreatic Neoplasms, Adenocarcinoma, Mucinous, Adenocarcinoma, Papillary, Aged, 80 and over, Pancreatic Intraductal Neoplasms, Splenectomy
Background
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas is a relatively new and rare clinical entity. It is defined as an intraductal, grossly visible, tubule-forming epithelial neoplasm with high-grade dysplasia and ductal differentiation without overt production of mucin [1,2]. Suda et al. published 4 cases of “intraductal papillotubular pancreatic carcinoma with scant mucin production” in 1996 [3]. However, the term ITPN was introduced by Yamaguchi et al. in 2009; they described the first 10 acknowledged cases of pancreatic ITPN [1]. In 2010 the World Health Organization (WHO) recognized ITPN as a distinct subgroup of intraductal tumors of the pancreas [4]. Since then, less than 40 cases of ITPN have been published. As a result, there is insufficient information regarding its clinicopathologic features, treatment options, and outcomes [5,6]. We herein present the seventh case of total pancreatectomy for ITPN reported in the English literature.
Case Report
Our patient was an 82-year-old male with a history of hyper-tension who had suffered from acute pancreatitis 16 years ago due to gallstone disease. He underwent laparoscopic cholecystectomy after conservative treatment of acute pancreatitis at that time and had a normal recovery. As a consequence, acute pancreatitis evolved to what seemed to be chronic pancreatitis. The patient suffered from sporadic episodes of abdominal pain along with elevated amylase levels and ended up with diabetes and exocrine pancreatic insufficiency with normal amylase levels. His medical treatment included amlodipine 5 mg/valsartan 160 mg, nebivolol 5 mg, metformin 850 mg, and pancreatin 25 000 IU.
The patient was in a good clinical condition when he referred to our surgical team 4 years ago. Physical examination revealed a soft abdomen without any palpable mass. Laboratory values of complete blood count, biochemical blood tests (liver function tests, amylase, lipase) and serum tumor markers (carcinoembryonic antigen [CEA], cancer antigen [CA] 19-9, CA 125, CA 72-4, and alpha-fetoprotein [AFP]) were within normal limits apart from elevated serum glucose levels (130 mg/dL) due to the known diabetes. Contrast enhanced computed tomography (CT) and magnetic resonance imaging (MRI) of the abdomen showed elements of chronic pancreatic inflammation and presence of cystic lesions which were diagnosed as pseudocysts. Upper gastrointestinal endoscopy revealed normal findings especially in the area of Vater’s papilla. Considering his age and a potentially benign disease we treated him conservatively for 2 years with simple painkillers, dietary restrictions, and pancreatic exocrine enzyme and insulin substitution.
The patient suddenly started to lose weight (6 kg in a year) and presented general symptoms like anorexia, sense of fullness after meal, weakness, and fatigue. Moreover, his Ca 19-9 levels elevated to 265 U/mL (reference range <37 U/mL). The latest abdominal MRI showed new elements that were suspicious for multifocal pancreatic neoplasia. There was a diffuse cystic dilation of the whole pancreas with severe parenchymal heterogeneity (Figure 1A, 1B). A cystic lesion with compact elements was found in the tail of the pancreas which was adherent to the hilum of the spleen and showed high signal intensity in T2-weighed MRI (Figure 1C). MR cholangiopancreatography (MRCP) revealed mild dilation of the common hepatic duct with smooth stenosis of the intrapancreatic portion of the common bile duct. MRCP failed to visualize the major or accessory pancreatic duct (Figure 1D). Moreover, abdominal CT angiography (CTA) showed a hypodense cystic lesion at the head and uncinate process of the pancreas which was in contact and caused distortion of the superior mesenteric vein (Figure 2A, 2B).
A CT-guided biopsy of the cystic lesion at the body and tail of the pancreas was performed which indicated pancreatic intraductal neoplasia with intermediate dysplasia (Figure 2C). Two years after our patient presented to our surgical team, he was referred for oncology consultation which determined that he should be treated surgically with total pancreatectomy and possibly with adjuvant chemotherapy, depending on the pathology report.
We performed a double Kocher incision to access the perito-neal cavity. The liver and all other intraabdominal organs were free of macroscopic disease. The pancreas was diffusely dilated, and its wall was thick and hard in palpation. We performed a Kocher maneuver and we confirmed that the tumor was resectable. The tumor was in contact but did not infiltrate the superior mesenteric vein. The hilum of the spleen was infiltrated by the cystic mass of the pancreatic tail, so we decided to perform a pylorus-preserving total pancreatectomy with splenectomy and regional lymphadenectomy (Figure 3).
Macroscopic examination of the specimen indicated the presence of an off-white lesion occupying both the head and the body of the pancreas with a maximum diameter of 8.5 cm along with a second similar lesion at the edge of the pancreatic tail measuring 4.5 cm in diameter. Histologic examination revealed the presence of multifocal ITPN of the pancreas with intermediate to severe dysplasia and absence of mucin. The neoplasm was observed mainly inside dilated pancreatic ducts and was associated with extensive invasive component which infiltrated both the duodenal wall and the peripancreatic adipose tissue (Figure 4). There was also observed focal peri-neural invasion. All 21 resected lymph nodes were non-meta-static, and the final pathology stage of the tumor was pT3N0.
Immunohistochemical studies of the specimen showed that the tumor cells were positive for cytokeratin 7, CA 19-9, and MUC1, whereas they were negative for cytokeratin 20, MUC2, and CDX2 (Figure 5).
The patient had an uncomplicated postoperative course and was discharged on the ninth postoperative day in a good clinical condition. He received adjuvant chemotherapy with gemcitabine (single agent) for 6 months which he tolerated well. Follow-up at 6 and 12 months after surgery with abdominal and chest CT did not show any recurrence or metastatic disease. The patient was diagnosed with hepatic metastases 18 months after surgery. He refused to receive any other adjuvant therapy. At the time of this report, 28 months after surgery, he was still alive and active.
Discussion
Intraductal tubulopapillary neoplasms (ITPNs) of the pancreas account for less than 1% of all pancreatic exocrine tumors and approximately 3% of all pancreatic intraductal neoplasms [1,6,7]. Intraductal tumors of the pancreas are classified as intraductal pancreatic mucinous neoplasms (IPMNs) and ITPNs according to the 4th World Health Organization (WHO) tumor classification in 2010 [4–9].
Immunohistochemical workup is useful to confirm the diagnosis of ITPN. Typically, ITPNs show pancreatic duct differentiation by strong expression of CK7 (100%) and CK19 (95%), as well as expression of MUC1 (88%) and MUC6 (74%). Additionally, they lack gastroenteric differentiation and they do not express MUC2 and MUC5AC, unlike some types of IPMNs. Most IPMNs are positive for MUC5AC and negative for MUC6, apart from the oncocytic-type [1,5,7,8,10]. Molecular findings in patients with ITPN include somatic PIK3CA mutations in 18% of cases, KRAS in 10%, TP53 in 23% and BRAF in 15% [2,10,11].
Macroscopically, ITPN is a solid nodular tumor that arises mostly in the main pancreatic duct and causes upstream dilation of the ducts surrounding the neoplasm [1,5,10]. Branch-duct ITPNs have been detected in 5% to 10% of cases without dilation of the main pancreatic duct [10,12]. Inomata et al. reported the case of a patient with concurrent presence of branch-duct ITPN and IPMN in the head of the pancreas in 2018 [12]. ITPNs have also been found to arise from the bile ducts [5,13,14]. ITPN is most frequently located in the head of the pancreas in almost half of the patients. It can also be found in the body of the pancreas (17%), in the tail (7%), in both the head and body (3%), in both the body and tail (7%), and diffusely in the whole pancreas (14%) [2,5,8,10], like our patient
Preoperative diagnosis of ITPN is challenging since there is not a “gold-standard” method in literature. Duodenoscopy and endoscopic retrograde cholangiopancreatography (ERCP) may provide preoperative diagnosis in some patients with abnormal tissue sticking out of the papilla of Vater that can be taken for biopsy [5,6]. Endoscopic ultrasonography fine needle aspiration cytology (EUS-FNAC) may also be helpful in confirming the diagnosis of ITPN [15,16]. Kölby et al. suggested that imaging-guided core needle biopsy (CNB) could be more useful since it enables histologic examination [2]. The “cork-of-wine-bottle” sign and the “2-tone duct” sign are characteristic in MRCP and ERCP and are associated with the intraductal growth of ITPN [17]. Zhang et al. suggested in 2019 that MRI is an important imaging examination for the preoperative diagnosis of ITPN since it provides more detailed information about the tumor [18]. In our patient, imaging studies and CT-guided biopsy pointed to the diagnosis of multifocal intraductal pancreatic tumor.
In published case series, patients with ITPN presented with a variety of symptoms: abdominal pain or discomfort, nausea and vomiting, jaundice, anemia, severe diarrhea or steator-rhea, appetite or weight loss, fever, excessive thirst, exacerbation of diabetes mellitus and acute abdomen due to rupture of ITPN. About one-third of patients were asymptomatic and ITPN was an incidental finding [2,5–8,10,19]. ITPN has also been associated with episodes of recurrent acute pancreatitis and should be considered in the differential diagnosis of idiopathic acute pancreatitis [20]. The intraluminal growth of the neoplasm inside the pancreatic duct may cause slow obstruction and obstructive chronic pancreatitis [11]. This is a patho-physiological mechanism that can explain the symptoms of chronic pancreatitis to our patient.
ITPN is considered a precursor lesion to invasive pancreatic ductal adenocarcinoma [4,11,21–23]. Approximately 40% to 50% of ITPN cases harbor an invasive component and they should be referred to as cases of “ITPN with an associated invasive carcinoma” [2,7,10,22]. Male sex, large tumor size, dilated pancreatic duct with pancreatoliths and high Ki-67 labelling index could be considered as predictive factors for invasiveness [2,23]. Rare cases of patients with lymphovascular and perineural invasion, lymph node and liver metastases are reported in literature [8]. Fujimoto et al. consider all 31 cases of ITPN reviewed by them as intraductal tubulopapillary cancer despite the presence or absence of an invasive component [6].
Prognosis of ITPN after curative resection seems to be more favorable than conventional pancreatic ductal adenocarcinoma according to literature data [5,8,10]. Basturk et al. [8] published a case series of 33 patients with ITPN in 2017. Twenty-two patients had available follow-up clinical information for a median time of 45 months; 15 patients had associated invasive component, 6 patients did not have invasive cancer, and 1 patient had only biopsy specimen. The estimated overall 1-year, 3-year, and 5-year survival rate of these 22 patients was 100% (22 out of 22), 93% (20 out of 22), and 77% (17 out of 22), respectively. The overall 5-year survival rate was 100% (6 out of 6) in cases without invasive carcinoma and 1-year, 3-year, and 5-year survival rates were 100% (15 out of 15), 91% (14 out of 15), and 71% (11 out of 15), respectively in cases with invasive carcinoma [8]. Fujimoto et al. presented an overall 1-year survival rate of 88% (23 out of 26) in their case series of 31 patients with ITPN published also in 2017. Twenty-six patients had available follow-up clinical information [6].
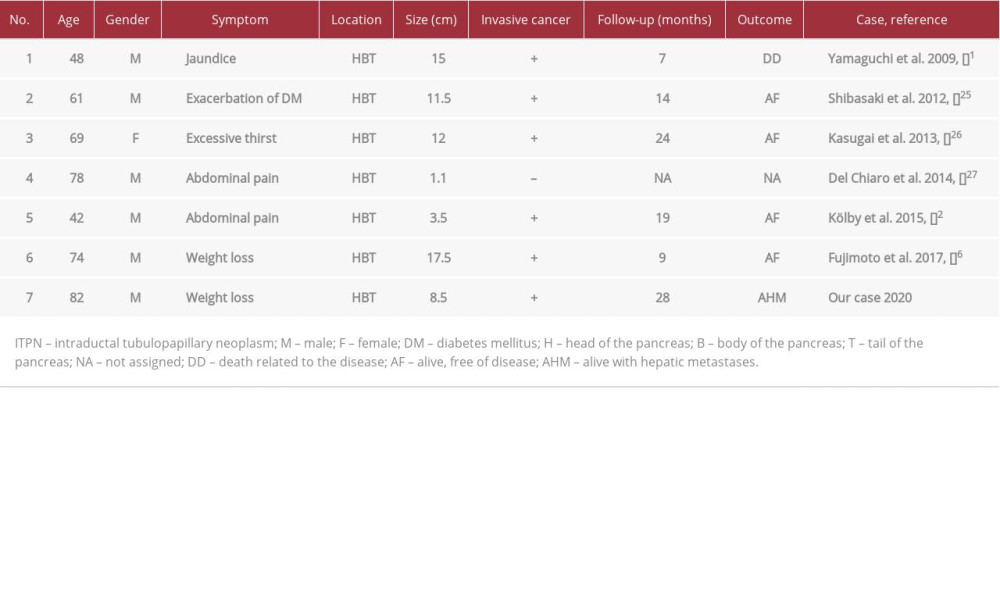
Radical surgical treatment performed before ITPN evolves into an invasive carcinoma is recommended by some authors and has been associated with a better prognosis [2,23]. The most common surgical procedure for ITPN is pancreatoduodenectomy according to the literature [5,6,10]. In cases with multifocal ITPN, like our patient, total pancreatectomy is the preferred surgery following oncological criteria [5 6]. Fujimoto et al. [6] and Basturk et al. [8] published 5 cases of total pancreatectomy for ITPN in 2017. Date et al. [7] included in their review a new case of a Japanese patient treated with total pancreatectomy by Shibasaki et al. [25] in 2012. Thus, our patient is the seventh case (Table 1) of total pancreatectomy for ITPN reported in the English literature since the original article of Yamaguchi et al. in 2009.
Six out of these 7 patients with total pancreatectomy were male (86%) and 1 was female. Their mean age was 65 years old (range, 42 to 82 years old). All 7 cases were multifocal pancreatic ITPNs and 6 out of 7 patients (86%) harbored an associated invasive carcinoma. The mean tumor size was 9.87 cm (range, 1.1 to 17.5 cm). One out of 7 patients died 7 months after surgery due to the primary disease. One patient with a familial history of pancreatic cancer did not have postoperative follow-up details available. Four patients (57%) were alive without recurrence on clinical follow-up for a mean period of 16.5 months (range, 9 to 24 months). Finally, our patient was alive with hepatic metastases 28 months after surgery [1,2,6,25–27].
The extent of surgical resection should be taken into serious consideration for the treatment of ITPN, since 7 cases of local recurrence have been published in the English literature. The soonest was 12 months after surgery and the latest was 16 years after surgery. Recurrence of ITPN may require total pancreatectomy. Additionally, recurrence has occurred even in cases where the initial ITPN was not associated with invasive carcinoma [1,9,28]. Three possible mechanisms have been proposed to elucidate this phenomenon: a) residual cancer cells in the remnant pancreas, b) intraductal or intrapancreatic lymphovascular spread, and c) metachronous, multicentric development [9,28].
Due to the rarity of ITPN there are no evidence-based guidelines for the treatment (including chemotherapy or radiation therapy) for this pancreatic tumor. According to the existing literature, neo-adjuvant therapy was not applied to any patient from the reported cases. Adjuvant chemotherapy has also been avoided in many patients, even in some cases with coexisting invasive cancer, since ITPN has a lower malignancy potential than pancreatic ductal adenocarcinoma [5]. In our case, we treated our patient with adjuvant gemcitabine (single agent) for 6 months because the neoplasm extensively infiltrated the duodenal wall and the peripancreatic adipose tissue, and there were also foci of perineural invasion. These elements suggested potential aggressive behavior of the tumor and the patient was considered at high risk for local recurrence or distant metastases [28,29].
Three patients with pancreatic ITPN and associated invasive cancer have been treated with adjuvant gemcitabine and capecitabine (Xeloda) [2,18,23]. Two of them were alive and disease-free 15 and 19 months after surgery [2,23], whereas the third was diagnosed with hepatic metastases in the fourth postoperative month [18]. There were also 4 reported cases of patients from Japan with pancreatic ITPN who received postoperatively S-1 (tegafur-gimeracil-oteracil potassium) [9,20,30,31]. S-1 plays a key role in the treatment of pancreatic cancer in Japan besides gemcitabine [32]. Three of these cases were diagnosed with recurrence of the primary disease at 15 months [30], 34 months [31] and 16 years after pancreatoduodenectomy [9]. The fourth was alive and disease-free in the first postoperative year [20].
Conclusions
ITPN is a rare entity with a limited number of reported cases in the literature. In some patients it has been associated with previous acute pancreatitis. ITPN should be included in the differential diagnosis in patients with chronic obstructive pancreatitis and unexplained pancreatic insufficiency. Early diagnosis, radical surgical resection following oncologic criteria, and adjuvant chemotherapy may lead to long-term survival rates even in cases with associated invasive cancer. Total pancreatectomy may be a preferable procedure for ITPN in selected patients since many tumors are multifocal and cases with remnant pancreatic recurrence have been described even 16 years after the initial surgery.
Figures
References:
1.. Yamaguchi H, Shimizu M, Ban S, Intraductal tubulopapillary neoplasms of the pancreas distinct from pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms: Am J Surg Pathol, 2009; 33; 1164-72
2.. Kölby D, Thilén J, Andersson R, Multifocal intraductal tubulopapillary neoplasm of the pancreas with total pancreatectomy: Report of a case and review of literature: Int J Clin Exp Pathol, 2015; 8; 9672-80
3.. Suda K, Hirai S, Matsumoto Y, Variant of intraductal carcinoma (with scant mucin production) is of main pancreatic duct origin: A clinicopatho-logical study of four patients: Am J Gastroenterol, 1996; 91(4); 798-800
4.. Bosman FT, Carneiro F, Hruba Rh: WHO classification of tumors of the digestive system, 2010; 304-13, Lyon, IARC Press
5.. Kuscher S, Steinle H, Soleiman A, Intraductal tubulopapillary neoplasm (ITPN) of the pancreas associated with an invasive component: A case report with review of the literature: World J Surg Oncol, 2017; 15; 203
6.. Fujimoto Y, Tomimaru Y, Tamura H, Pancreatic intraductal tubulopapillary neoplasm with associated invasive cancer successfully treated by total pancreatectomy: A case report: Oncol Lett, 2017; 14(1); 153-58
7.. Date K, Okabayashi T, Shima Y, Clinicopathological features and surgical outcomes of intraductal tubulopapillary neoplasm of the pancreas: A systemic review: Langenbecks Arch Surg, 2016; 401(4); 439-47
8.. Basturk O, Adsay V, Askan G, Intraductal tubulopapillary neoplasm of the pancreas: A clinicopathologic and immunohistochemical analysis of 33 cases: Am J Surg Pathol, 2017; 41(3); 313-25
9.. Saeki K, Miyasaka Y, Ohishi Y, Intrapancreatic recurrence of intraductal tubulopapillary neoplasm (ITPN) 16 years after the initial surgery for noninvasive ITPN: A case report: Surg Case Rep, 2018; 4(1); 96
10.. Rooney SL, Shi J, Intraductal tubulopapillary neoplasm of the pancreas: An update from a pathologist’s perspective: Arch Pathol Lab Med, 2016; 140(10); 1068-73
11.. Kim H, Ro JY, Intraductal tubulopapillary neoplasm of the pancreas: An overview: Arch Pathol Lab Med, 2018; 142(3); 420-23
12.. Inomata K, Kitago M, Obara H, Concurrent presentation of an intraductal tubulopapillary neoplasm and intraductal papillary mucinous neoplasm in the branch duct of the pancreas, with a superior mesenteric artery aneurysm: A case report: World J Surg Oncol, 2018; 16(1); 83
13.. Katabi N, Torres J, Klimstra DS, Intraductal tubular neoplasms of the bile ducts: Am J Surg Pathol, 2012; 36; 1647-55
14.. Schlitter AM, Jang KT, Klöppel G, Intraductal tubulopapillary neoplasms of the bile ducts: clinicopathologic, immunohistochemical, and molecular analysis of 20 cases: Mod Pathol, 2015; 28; 1249-64
15.. Furuhata A, Minamiguchi S, Mikami Y, Intraductal tubulopapillary neoplasm with expansile invasive carcinoma of the pancreas diagnosed by endoscopic ultrasonography-guided fine needle aspiration: A case report: Diagn Cytopathol, 2014; 42(4); 314-20
16.. Tajima S, Intraductaltubulopapillary neoplasm of the pancreas suspected by endoscopic ultrasonography – fine-needle aspiration cytology: Report of a case confirmed by surgical specimen histology: Diagn Cytopathol, 2015; 43(12); 1003-6
17.. Motosugi U, Yamaguchi H, Furukawa T, Imaging studies of intraductal tubulopapillary neoplasms of the pancreas: 2-tone duct sign and cork-of-wine-bottle sign as indicators of intraductal tumor growth: J Comput Assist Tomogr, 2012; 36(6); 710-7
18.. Zhang J, Ren S, Wang J, Imaging findings of intraductal tubulopapillary neoplasm (ITPN) of the pancreas. Two case reports and literature review: Medicine (Baltimore), 2019; 98(6); e14426
19.. Umemura A, Ishida K, Nitta H, A rare case of intraductal tubulopapillary neoplasm of the pancreas rupturing and causing acute peritonitis: Case Rep Gastroenterol, 2017; 11(3); 661-66
20.. Sakamoto S, Tsuruga Y, Fujii Y, Intraductal tubulopapillary neoplasm of the pancreas presenting as recurrent acute pancreatitis: A case report: Int J Surg Case Rep, 2018; 48; 122-25
21.. Noë M, Brosens LA, Pathology of pancreatic cancer precursor lesions: Surg Pathol Clin, 2016; 9; 561-80
22.. Riva G, Pea A, Pilati C, Histo-molecular oncogenesis of pancreatic cancer: From precancerous lesions to invasive ductal adenocarcinoma: World J Gastrointest Oncol, 2018; 10(10); 317-27
23.. Fritz s, Küper-Steffen R, Feilhauer K, Intraductal tubular papillary neoplasm (ITPN), a novel entity of pancreatic epithelial neoplasms and precursor of cancer: A case report and review of the literature: Int J Surg Case Rep, 2019; 55; 187-91
24.. Kim HJ, Park MS, Chung T, Multimodality imaging studies of intraductal tubulopapillary neoplasms of the pancreas: Diagn Interv Radiol, 2019; 25(4); 251-56
25.. Shibasaki Y, Sakaguchi T, Inaba K, Intraductal tubulopapillary neoplasm of the pancreas successfully treated with total pancreatectomy: J Jpn Surg Assoc, 2012; 73; 2061-67
26.. Kasugai H, Tajiri T, Takehara Y, Intraductal tubulopapillary neoplasms of the pancreas: Case report and review of the literature: J Nippon Med Sch, 2013; 80; 224-29
27.. Del Chiaro M, Mucelli RP, Blomberg J, Is intraductal tubulopapillary neoplasia a new entity in the spectrum of familial pancreatic cancer syndrome?: Fam Cancer, 2014; 13; 227-29
28.. Neoptolemos JP, Kleeff J, Michl P, Therapeutic developments in pancreatic cancer: Current and future perspectives: Nat Rev Gastroenterol Hepatol, 2018; 15(6); 333-48
29.. Liang D, Shi S, Xu J, New insights into perineural invasion of pancreatic cancer: More than pain: Biochim Biophys Acta, 2016; 1865(2); 111-22
30.. Ko K, Nishida Y, Sasahara K, A resected case of recurrent ITPN in the remnant pancreas after pancreatoduodenectomy: Surg Case Rep, 2019; 5(1); 33
31.. Urata T, Naito Y, Nagamine M, Intraductal tubulopapillary neoplasm of the pancreas with somatic BRAF mutation: Clin J Gastroenterol, 2012; 5(6); 413-20
32.. Sudo K, Nakamura K, Yamaguchi T, S-1 in the treatment of pancreatic cancer: World J Gastroenterol, 2014; 20(41); 15110-18
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953068
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133