28 November 2020: Articles 
Pulmonary Embolism Presenting as ST-Elevation Myocardial Infarction: A Diagnostic Trap
Challenging differential diagnosis
Ayesha Siddiqa1ABCDEF*, Asim Haider1ABCDEF, Abhishrut Jog1ABCDEF, Bing Yue2ABCDEF, Nassim R. Krim2ABCDEFDOI: 10.12659/AJCR.927923
Am J Case Rep 2020; 21:e927923






Abstract
BACKGROUND: The clinical presentation of pulmonary embolism (PE) is highly variable, ranging from no symptoms to shock or sudden death, often making the diagnosis a challenge. An electrocardiogram (EKG) is not a definitive diagnostic tool; however, it can alter the clinical suspicion of acute PE. PE has nonspecific electrocardiographic patterns ranging from a normal EKG in almost 33% of patients to sinus tachycardia, S1Q3T3 pattern (McGinn-White Sign), right axis deviation, and incomplete right bundle branch block (RBBB). ST-segment elevation associated with PE is exceedingly rare, and to date, only a few cases have been reported.
CASE REPORT: We present a case of a middle-aged male patient with no medical comorbidities other than obesity, who presented with initial symptoms and EKG findings concerning an ST-elevation myocardial infarction (STEMI). He was later found to have rather patent coronary arteries on cardiac catheterization but bilateral sub-massive pulmonary embolism on computed tomography angiogram (CTA) of the chest.
CONCLUSIONS: The differential diagnosis of STEMI is broad, including, but not limited to, Prinzmetal’s angina, takotsubo cardiomyopathy, Brugada syndrome, left ventricular aneurysm, hypothermia, hyperkalemia, and acute pericarditis. Pulmonary embolism may present with abnormal EKG and biomarkers that appear to be an acute coronary syndrome, even STEMI. Physicians must maintain a high index of clinical suspicion through risk stratification to identify PE in these settings, as the frequency of such an occurrence is extremely low. A bedside echocardiogram can be an invaluable diagnostic tool in such cases.
Keywords: acute coronary syndrome, Electrocardiography, Pulmonary Embolism, Arrhythmias, Cardiac, Bundle-Branch Block, ST elevation myocardial infarction
Background
The precise incidence of pulmonary embolism (PE) is unknown; estimates suggest PE and deep venous thrombosis (DVT) account for 60,000 to 100,000 deaths per year in the United State. Between 10% and 30% die within 1 month of diagnosis, and around 33% percent are at risk of having a recurrence within 10 years. The overall incidence and case-fatality rate increase with increasing age [1,2]. The prognosis of PE is determined both by the degree of vascular obstruction and hemodynamic stability. The estimated mortality rate associated with low-risk PE is <1%, whereas sub-massive and massive PE have mortality rates of 3–15% and 25–65%, respectively [1,3]. Therefore, a high level of suspicion must be maintained for identifying patients in whom diagnostic testing may be necessary. The evaluation approach should be efficient while simultaneously avoiding the risks of unnecessary testing so that therapy can be promptly initiated and potential morbidity and mortality avoided [4].
The electrocardiogram (EKG) is the most crucial test in the evaluation of any patient with chest pain. ST-elevation is the most life-threatening acute EKG change and directs the clinician toward urgent thrombolysis or percutaneous coronary intervention (PCI). A few conditions other than ST-elevation myocardial infarction (STEMI) can have ST-elevation in the EKG, such as Prinzmetal’s angina, takotsubo cardiomyopathy, Brugada syndrome, left ventricular aneurysm, hypothermia, hyperkalemia, and acute pericarditis [5]. However, it is exceedingly rare to find ST-elevation in a patient with PE, with only a few cases being reported in the past.
Case Report
A 50-year-old man with obesity (BMI 37) was brought in by emergency medical services (EMS) as a STEMI notification for an acute-onset chest pain for 3 hours. The pain was intermittent, retrosternal, squeezing in character, non-radiating, and exertional. There was associated exertional dyspnea. He also reported a syncopal episode 2 weeks before the chest pain, for which a computerized tomography (CT) scan of the head had been done and was negative. Initial vital signs were a respiratory rate of 33 breaths per minute, a heart rate of 133 bpm, a temperature of 36.3°C, and blood pressure of 127/68 mmHg. Otherwise, the patient was found to have an unremarkable systemic physical examination. An initial EKG showed sinus tachycardia with ST-elevation from V1 to V3 with deep T-wave inversions in the precordial leads V1–V4 (Figure 1). Unfortunately, there was no previous EKG available for comparison. Due to active chest pain and EKG concerning for acute coronary syndrome, the patient was started on heparin, aspirin, and clopidogrel and was taken for cardiac catherization within 20 min of arrival. Surprisingly, the coronaries were found to be patent. Later on, blood tests were remarkable for high-sensitivity troponin T elevation of 43 ng/L, pro-BNP of 27,658 pg/ml, and a D-dimer of 2466 ng/ml. An urgent echocardiogram (ECHO) was done, which showed severe right-ventricle strain with a right ventricular systolic pressure of 65 mmHg and McConnel’s sign suggesting pulmonary embolism (Figures 2–4, Video 1). Computed tomography angiography (CTA) was consistent with bilateral significant filling defects within the main pulmonary arteries extending into the subsegmental branches (Figure 5). Ultrasound imaging of the lower extremities was consistent with a thrombus throughout the right popliteal, superficial femoral, and common femoral veins. Heparin drip was continued and later switched to enoxaparin. In the setting of refractory hypoxia and high clot burden, the patient was offered alteplase and thrombectomy, but he refused. He was discharged on apixaban and home oxygen.
Discussion
A timely diagnosis of PE remains challenging as there is a wide variety of presenting features suggestive of PE, ranging from no symptoms to shock or sudden death. The most common symptoms identified by the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) group are exertional or resting dyspnea (73%), pleuritic chest pain (66%), thigh swelling (44%), cough (37%), orthopnea (28%), wheezing (21%), hemoptysis (13%), and, less commonly, syncope, presyncope, arrhythmias, and hemodynamic collapse (<10% each) [6]. Delayed presentation (over weeks or days) is common in many patients. Even patients with large PE can have mild or nonspecific symptoms or are asymptomatic [7,8]. Although the true incidence of asymptomatic PE remains unknown, a systematic review of 28 studies found that, among the 5233 patients who had a DVT, 32% had silent PE [9].
A meta-analysis of 19 studies found that clinical impression alone had a sensitivity of 85% and specificity of 51% for PE diagnosis [10]. Thus, a high level of suspicion must be maintained so that clinically relevant cases are not missed. X-ray chest and lab tests, including ABG, BNP, troponin, and D-dimer, are non-diagnostic but play an essential role in reliable risk stratification of patients with PE. Chest CTA is the imaging modality with >90% specificity and sensitivity. V/Q scan is an alternative for patients in whom the CTA is inconclusive or relatively contraindicated (e.g., history of moderate or severe contrast allergy, renal insufficiency [estimated glomerular filtration rate <30 mL/min/1.73 m2] or hypotension). However, ECHO has limited value diagnostically; approximately 30–39% of patients with PE present echocardiographic abnormalities indicating right ventricular strain or pressure overload [8,11]. McConnell’s sign (regional wall motion abnormalities that spare the right ventricular apex) has 77% sensitivity and 94% sensitivity for the diagnosis of PE and can discern patients with pulmonary hypertension, who tend to have global right ventricular (RV) dysfunction as opposed to those with RV strain from acute PE [12].
Treatment guidelines recommend that clinicians employ a clinical strategy that includes risk stratification of patients with pulmonary embolism (PE) to estimate the probability of circulatory shock and 30-day all-cause mortality. Well-recognized methods for risk stratification include scoring systems, blood biomarkers (troponins I and T, brain natriuretic peptides), findings of a dilated RV on CT chest, and echocardiographic findings of RV strain [8,13]. Although it remains challenging to define the physiological basis for the EKG findings associated with PE, EKG may be useful to alter the clinical suspicion of acute PE. PE has nonspecific electrocardiographic patterns, ranging from a normal EKG in almost 33% of patients to findings suggestive of right ventricle strain, including sinus tachycardia, S1Q3T3 pattern, right axis deviation, right bundle branch block, T-wave inversions in V2 and V3, atrial fibrillation, and ST-elevation in the VR lead [13].
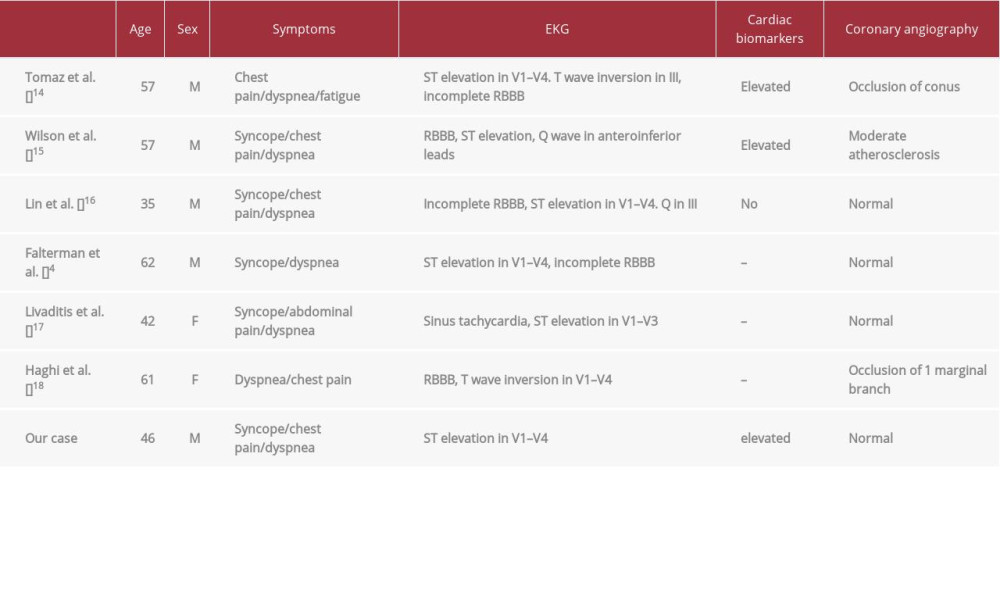
ST-segment elevation associated with PE is rare. The overall incidence rate of ST-elevation in patients presenting with acute PE is unknown, and, to date, only a few cases have been reported (Table 1) [4,14–18]. In 2001 Falterman and colleagues reported the first case of PE with ST-segment elevation in leads V1–V4 in a 62-year-old man who died despite resuscitative efforts. An autopsy revealed no evidence of myocardial infarction; instead, the patient died of a pulmonary embolism [4].
The direct relationship between acute PE and ST-elevation remains unclear [15]. However, a few suggested theories are: (a) severe hypoxemia induces a catecholamine surge, which increases myocardial workload and results in ischemia; (b) a sudden pressure load on a non-compensatory right ventricle, which may cause global or focal myocardial ischemia due to additional strain; and (c) a possible mechanism of ST-segment elevation in patients with DVT and PE is paradoxical embolization of a venous clot across an atrial septal defect or a patent foramen ovale into a coronary vessel [15].
An arterial plaque rupture leads to the acute coronary syndrome (ACS), whereas deep vein thrombosis accounts for PE pathophysiology. Despite having different pathological backgrounds, the concomitant existence of both entities has been reported. A few proposed mechanisms of co-existence of ACS and PE are: (a) massive PE leading to RV infarction due to increased RV afterload; (b) presence of severe coronary artery obstruction; and (c) patent foramen ovale leading to paradoxical coronary embolism, allowing the thrombus to pass from RA to the left atrium. However, the co-existence is quite rare. A retrospective analysis of 467 patients revealed a low prevalence of 5.5% of ACS among PE patients, suggesting that patients presenting with initial high pre-test PE probability should be triaged for CTA chest and ECHO [19–21].
In our case, the STEMI notification was initiated by EMS due to EKG findings and active chest pain. To ensure timely management of suspected acute coronary syndrome, the patient was taken for cardiac catherization prior to any further diagnostic test or laboratory test. The ECHO proved an invaluable resource in this case. The presence of McConnell’s sign pointed toward PE as a cause of the chest pain and prompted us to get a chest CTA.
Conclusions
Pulmonary embolism may present with abnormal EKG and bio-markers that may appear to be an acute coronary syndrome, even STEMI. A high index of suspicion should be maintained to identify PE in this setting, as the frequency of such an occurrence is extremely low. A bedside transthoracic ECHO is invaluable in this situation and will provide a definitive diagnosis, thereby avoiding unnecessary diagnostic and therapeutic decisions.
Figures
References:
1.. Turetz M, Sideris AT, Friedman OA, Epidemiology, pathophysiology, and natural history of pulmonary embolism: Semin Intervent Radiol, 2018; 35; 92-98
2.. Horlander KT, Mannino DM, Leeper KV, Pulmonary embolism mortality in the United States, 1979–1998: An analysis using multiple-cause mortality data: Arch Intern Med, 2003; 163; 1711-17
3.. Kucher N, Tapson VF, Goldhaber SZ, Risk factors associated with symptomatic pulmonary embolism in a large cohort of deep vein thrombosis patients: Thromb Haemost, 2005; 93(3); 494-98
4.. Falterman TJ, Martinez JA, Daberkow D, Weiss LD, Pulmonary embolism with ST segment elevation in leads V1 to V4: Case report and review of the literature regarding electrocardiographic changes in acute pulmonary embolism. J: Emerg Med, 2001; 21; 255-61
5.. , McGraw-Hill education launches landmark of Harrison’s principles of internal medicine Sep 27, 2018 PR Newswire Europe Including UK Disclose retrieved from http://eresources.library.mssm.edu.eresources.mssm.edu/login
6.. Stein PD, Terrin ML, Hales CA, Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease: Chest, 1991; 100; 598-603
7.. Stein PD, Beemath A, Matta F, Clinical characteristics of patients with acute pulmonary embolism: Data from PIOPED II: Am J Med, 2007; 120; 871-79
8.. Konstantinides SV, Meyer G, Becattini C, 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC): Eur Heart J, 2020; 4; 543-603
9.. Stein PD, Matta F, Musani MH, Diaczok B, Silent pulmonary embolism in patients with deep venous thrombosis: A systematic review: Am J Med, 2010; 123; 426-31
10.. Lucassen W, Geersing GJ, Erkens PM, Clinical decision rules for excluding pulmonary embolism: A meta-analysis: Ann Intern Med, 2011; 155; 448-60
11.. Kucher N, Rossi E, De Rosa M, Goldhaber SZ, Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher: Arch Intern Med, 2005; 165; 1777-81
12.. McConnell MV, Solomon SD, Rayan ME, Regional right ventricular dys-function detected by echocardiography in acute pulmonary embolism: Am J Cardiol, 1996; 78; 469-73
13.. Shopp JD, Stewart LK, Emmett TW, Kline JA, Findings from 12-lead electrocardiography that predict circulatory shock from pulmonary embolism: Systematic review and meta-analysis: Acad Emerg Med, 2015; 22; 1127-37
14.. Goslar T, Podbregar M, Acute ECG ST-segment elevation mimicking myocar-dial infarction in a patient with pulmonary embolism: Cardiovasc Ultrasound, 2010; 8; 50
15.. Wilson GT, Schaller FA, Pulmonary embolism mimicking anteroseptal acute myocardial infarction: J Am Osteopath Assoc, 2008; 108; 344-49
16.. Lin JF, Li YC, Yang PL, A case of massive pulmonary embolism with ST elevation in leads V1–4: Circ J, 2009; 73; 1157-59
17.. Livaditis IG, Paraschos M, Dimopoulos K, Massive pulmonary embolism with ST elevation in leads V1–V3 and successful thrombolysis with tenecteplase: Heart, 2004; 90; 41
18.. Haghi D, Sueselbeck T, Papavassiliu T, Paradoxical coronary embolism causing non-ST segment elevation myocardial infarction in a case of pulmonary embolism: Z Kardiol, 2004; 93; 824-28
19.. Yildiz A, Bostan C, Akin F, Concurrent pulmonary embolism and acute coronary syndrome with dynamic electrocardiographic changes: Am J Emerg Med, 2012; 30(4); 637.e1-4
20.. Qahtani SA, Kandeel AY, Breault S, Prevalence of acute coronary syndrome in patients suspected for pulmonary embolism or acute aortic syndrome: Rationale for the triple rule-out concept: J Clin Med Res, 2015; 7(8); 627-31
21.. Hayıroğlu Mİ, Bozbeyoğlu E, Akyüz Ş, Acute myocardial infarction with concomitant pulmonary embolism as a result of patent foramen ovale: Am J Emerg Med, 2015; 33(7); 984.e5-7
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.949976
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950290
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950607
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950985
Most Viewed Current Articles
07 Dec 2021 : Case report
17,691,734
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  164,491
164,491
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
113,090
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
59,175
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133