31 October 2020: Articles 
A 44-Year-Old Hispanic Man with Loss of Taste and Bilateral Facial Weakness Diagnosed with Guillain-Barré Syndrome and Bell’s Palsy Associated with SARS-CoV-2 Infection Treated with Intravenous Immunoglobulin
Rare disease
Misbahuddin Khaja1BDEF*, Gabriella P. Roa Gomez1ABDEF, Yaneidy Santana1ADEF, Nolberto Hernandez2ABDEF, Asim Haider2ADEF, Jose Luis Perez Lara1ABDEF, Rene Elkin3ABDFDOI: 10.12659/AJCR.927956
Am J Case Rep 2020; 21:e927956






Abstract
BACKGROUND: This case report is of a patient who presented with loss of taste and facial weakness and was diagnosed with Guillain-Barré syndrome (GBS) and Bell’s palsy, associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. GBS is a neurological emergency defined as acute inflammatory demyelinating polyneuropathy. The patient responded to intravenous immunoglobulin (IVIG) treatment.
CASE REPORT: We present the case of a 44-year-old Hispanic man who came for evaluation of bilateral facial weakness and lack of taste sensation. He had lower motor neuron facial weakness. His head computed tomography and brain magnetic resonance imaging scans did not show any pathological abnormalities. He tested positive for SARS-CoV-2 by a nasopharyngeal swab reverse transcription polymerase chain reaction (RT-PCR) test. Cerebrospinal fluid (CSF) analysis via lumbar puncture revealed elevated protein levels, no leukocytes, and a negative Gram stain. The CSF RT-PCR test for SARS-CoV-2 was negative. PCR tests of the CSF for other viral infections were negative. A diagnosis of GBS was made, and he was treated successfully with IVIG. After the fourth dose of IVIG, the patient was able to close his eyes, frown, show his teeth, and smile.
CONCLUSIONS: Our case is rare because the patient did not present with lower extremity weakness, but only with bilateral Bell’s palsy. Physicians should be aware of GBS because it is a neurological emergency for which COVID-19 can be a risk factor. Early diagnosis and treatment of GBS can prevent neurological disability.
Keywords: Bell Palsy, COVID-19, Guillain-Barre Syndrome, Ageusia, COVID-19, Diagnosis, Differential, Hispanic or Latino, Immunoglobulins, Intravenous, Immunologic Factors, Magnetic Resonance Imaging, Pandemics, SARS-CoV-2
Background
Bilateral Bell’s palsy can be a rare presentation of the underlying neurological emergency, Guillain-Barré syndrome (GBS). GBS is an acute immune-mediated demyelinating polyradiculopathy. Although facial weakness is seen in 50% of patients with GBS, unilateral or bilateral Bell’s palsy is rare. Various viral and bacterial infections are considered risk factors for GBS [1].
There have been previous pandemics of coronaviruses, including severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome. The current global pandemic is corona-virus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The neurological symptoms of SARS-CoV-2 infection include headache, myalgia, dizziness, loss of taste, loss of smell, impaired consciousness, encephalomyelitis, acute myelitis, seizures, polyneuropathy, mental status changes, cerebrovascular issues, ischemic stroke, intracerebral hemorrhage, and peripheral nervous system manifestations, such as GBS and Bell’s palsy [2,3].
This case report is of a patient who presented with loss of taste and bilateral facial weakness and was diagnosed with GBS and Bell’s palsy associated with SARS-CoV-2 infection, which responded to IVIG treatment.
Case Report
A 44-year-old Hispanic man with a past medical history of hypertension and asthma presented to the emergency department with bilateral facial weakness. He was on amlodipine 5 mg for arterial hypertension and an albuterol inhaler as needed for asthma. According to the patient, he had tearing in the left eye for 3 days before the left-side facial weakness presented. On the day the left-side facial weakness presented, his symptoms worsened and weakness on the right side of the face developed, leading to bilateral facial weakness. The patient also reported that he was unable to raise his eyebrows, close his eyes, and smile and he lacked taste sensation.
The patient denied any symptoms of cough, difficulty breathing, headache, dizziness, nausea, vomiting, fatigue, confusion, numbness, and weakness of the extremities. He also denied any difficulties with swallowing, vision, or speech. He had no history of smoking, alcohol abuse, recent travel, trauma, or exposure to ticks.
Physical examination showed that the patient was normally built and afebrile with a temperature of 36.7°C. He had a heart rate of 94 beats per min, blood pressure of 136/94 mmHg, respiratory rate of 18 breaths per min, and oxygen saturation of 98% on room air. Bilateral bronchial breathing sounds were noted, and the cardiovascular and gastrointestinal examinations were within normal limits. During the neurological examination, the patient was alert and oriented to people, place, and time and had no dysarthria or dysphagia. His sensations were intact, and he had a normal score of 5/5 for upper and lower extremity muscle strength and normal reflexes. The patient’s oculomotor movements and gait were also normal.
Further examination showed complete lower motor neuron facial weakness, which included the inability to raise his eyebrows, frown, close his eyes, smile, or pucker his lips. There was bilateral flattening of the nasolabial folds, and involvement of the bilateral orbicularis oris, orbicularis oculi, buccinators, and frontalis was consistent with lower motor neuron facial weakness. According to the House-Brackmann grading system, our patient had grade V severe dysfunction, with only barely perceptible motion, asymmetry with no motion of the forehead, incomplete eye closure, and slight deviation of the mouth. There was no hyperacusis and the corneal reflex was intact. The patient’s Brudzinski’s and Kernig’s signs were negative. All other cranial nerves were intact. The external ear exam did not show any vesicles, and the parotid gland was not enlarged. Pedal edema was present on the bilateral extremities.
Laboratory test results, which included a comprehensive metabolic panel and a complete blood count, were within normal limits. His D-dimer, serum ferritin, lactate dehydrogenase, and C-reactive protein levels were within normal range. The chest X-ray was clear, and the computed tomography scan of the head did not show any acute findings. Because the patient lacked taste sensation, a nasopharyngeal reverse transcription polymerase chain reaction (RT-PCR) test for SARS-CoV-2 was performed, and the results were positive for COVID-19. Our hospital uses the Roche cobas SARS-CoV-2 assay on the cobas 6800 system, a real-time RT-PCR test which qualitatively detects nucleic acid from SARS-CoV-2 in patient nasopharyngeal swab samples. It is used only under the Food and Drug Administration’s Emergency Use Authorization (EUA).
We performed a bedside lumbar puncture on the patient, and the cerebrospinal fluid (CSF) analysis showed elevated protein levels (92 mg/dL), no leukocytes, normal glucose levels (77 mg/dL), and a negative Gram stain. The CSF RT-PCR test for SARS-CoV-2 was negative, and the CSF PCR tests for other viruses, including cytomegalovirus, Epstein-Barr, herpes simplex, and varicella-zoster, were negative. CSF analysis showed albuminocytologic dissociation, favoring GBS as the diagnosis.
Brain magnetic resonance imaging (MRI) was performed with and without contrast, and there was no evidence of an acute infarction. There was no intracranial bleeding, intracranial mass effect, or abnormal enhancement found after injection of the contrast material. The parenchyma, ventricles, and cortical sulci were within normal limits. MRI of the cervical spine did not show any abnormal enhancements.
The patient’s serum test for IgG antibodies to GQ1B was negative. We did not perform electrodiagnostic studies because the patient’s clinical presentation and CSF analysis were consistent with GBS.
Once the patient was diagnosed with GBS after the lumbar puncture, he was started on intravenous immunoglobulin (IVIG). After the fourth dose of IVIG, he was able to partially close his right eye but was still unable to close his left eye. He was also able to frown his forehead, show his teeth, and smile. He received a total of 5 doses of IVIG. On hospitalization day 10, he was able to close both eyes. The patient was discharged on day 12 and had follow-up in the neurology clinic as an outpatient. There were no other complications associated with SARS-CoV-2 infection in our patient.
This is a case of GBS, a neurological emergency presented as bilateral facial palsy triggered by SARS-CoV-2 infection. The patient did not have any weakness in the lower extremities and his reflexes were normal.
Discussion
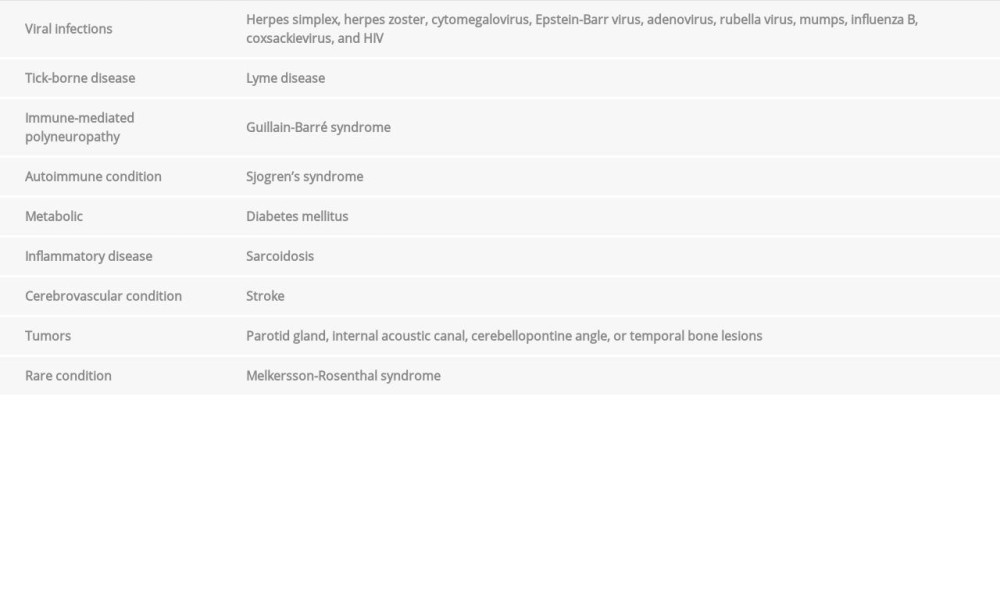
Bell’s palsy can be the only presenting feature of the life-threatening neurological emergency known as GBS. The most common causes of bilateral Bell’s palsy are herpes zoster, otitis media, sarcoidosis, Lyme disease, GBS, infectious mononucleosis, and Sjogren’s syndrome [4]. The list of causes is presented in the Table 1.
The pathogenesis of Bell’s palsy remains unclear, but it is postulated that neurotropic viruses induce immune responses and inflammation of the nerves, leading to demyelination. The other mechanisms of Bell’s palsy include ischemia of the facial nerves and a genetic predisposition [5].
GBS is an acute inflammatory demyelinating polyneuropathy with an unclear etiology. However, it is thought to be caused by an immune response directed to the myelin sheath or axons of the peripheral nerves from a prior infection. In GBS, weakness starts in the legs, but it can also begin in the facial muscles and the arms. It can also present as dysautonomia, oculomotor weakness, oropharyngeal weakness, paresthesia of the hands and feet, or respiratory muscle weakness requiring ventilator support. Furthermore, approximately 50% of GBS cases present as facial nerve palsy. GBS can cause symmetric muscle weakness with depressed or absent deep tendon reflexes, and it can take from a few days to a week for symptoms to present [6].
The most common infection that can trigger GBS is
SARS-CoV-2 infection usually presents as a cough, fatigue, fever, headache, dizziness, nausea, vomiting, and diarrhea. In severe cases, it presents as acute respiratory distress syndrome, acute cardiovascular problems, myopathy, rhabdomyolysis, multi-organ failure, and even death. The neurological symptoms can include encephalitis, seizures, polyneuropathy, mental status change, and cerebrovascular issues [8]. Patients who present with sudden onset of loss of taste or smell should have a high clinical suspicion of SARS-CoV-2 infection [9].
The neurologic complications of COVID-19 include cerebrovascular disease and a hypercoagulable state, which are rarely seen with other viral infections. Neurologic disorders secondary to SARS-CoV-2 infection could lead to long-term disability [10].
Our hospital uses the Roche cobas SARS-CoV-2 assay on the cobas 6800 system, a real-time RT-PCR test which qualitatively detects nucleic acid from SARS-CoV-2 in nasopharyngeal swab samples taken from patients. It is used only under the Food and Drug Administration’s EUA [11].
There are various mechanisms by which SARS-CoV-2 infection can cause nerve damage, including hypoxia, immune injury, direct infection via neuronal or blood circulation pathways, and angiotensin-converting enzyme 2 mechanisms. After nasal infection, SARS-CoV-2 enters the central nervous system via the olfactory bulb and olfactory nerves, leading to demyelination and inflammation. SARS-CoV-2 may also enter the central nervous system by infecting sensory neurons in the taste buds, and by entering the nucleus of the trigeminal nerve (V), the solitary tract (VII, IX, X), or the vagus nerve (X), which inner-vates the respiratory tract. From the respiratory tract, SARSCoV-2 enters the bloodstream via ACE2 receptors present on epithelial cells. ACE2 is a predominant target for coronaviruses and influenza viruses. Binding to this receptor can cause an elevation in blood pressure, leading to intracerebral hemorrhage. Glial cells in spinal neurons and the brain also have ACE2 receptors. The SARS-CoV-2 spike protein may also interact with ACE2 on capillary endothelia and damage the blood-brain barrier [12]. SARS-CoV-2 infection targets the immune pathway and causes lymphopenia and elevated C-reactive protein, ferritin, and D-dimer levels. D-dimer is a marker of hypercoagulation and fibrinolysis; thus, elevated D-dimer levels can explain the acute cerebrovascular disease caused by COVID-19 [13].
The diagnostic criteria for Bell’s palsy are acute onset over 1 or 2 days with progression of symptoms including diffuse facial nerve involvement manifesting as paralysis of the facial muscles and alteration in secretion of the salivary and lacrimal glands, with or without loss of taste on the anterior two-thirds of the tongue. An associated prodrome could include hearing impairment or ear pain. If the facial functions have not returned to baseline, then evaluation to determine another etiology is needed. Electrodiagnostic studies, which help in prognosis, and imaging studies, which look for surgically correctable causes, are not necessary for all patients with Bell’s palsy. If the physical signs are atypical with slow progression beyond 3 weeks or no improvement in 4 months, imaging studies are warranted. Blood is screened to look for infection or systemic diseases that can cause Bell’s palsy. According to the House-Brackmann grading system, our patient had grade V severe dysfunction [14,15].
In Bell’s palsy, House-Brackmann grading of V and VI and an absence of common symptoms of COVID-19, such as headache, myalgia, fever, loss of taste, and loss of smell, a short course of oral corticosteroid therapy is recommended [16]. In their review, Madhok et al. show that the frequency of incomplete recovery from Bell’s palsy decreases with the use of corticosteroids [17].
GBS is a clinical diagnosis made for its characteristic presentation of ascending symmetrical muscle weakness and absent deep tendon reflexes. Our patient presented with GBS variant bulbar symptoms, predominantly bilateral facial paresis and non-affected power in the peripheral extremities. The clinical diagnosis was supported by CSF analysis, electrodiagnostic studies, such as nerve conduction and electromyography, serum IgG antibody to GQ1B, and MRI of the brain and spinal cord, which showed enhancement of the nerves. The diagnostic criteria for GBS have both required and supportive features. The required features include weakness of the extremities, facial weakness, bulbar weakness, trunk weakness, and external ophthalmoplegia. The supportive features include the progress of symptoms, mild sensory signs, autonomic dys-function, electrodiagnostic abnormalities, and elevated CSF proteins with cell counts less than 5 cells/mm3, known as albuminocytologic dissociation [18].
Electrophysiologic studies are not required to diagnose GBS; however, they are used to distinguish subtypes of GBS, such as acute inflammatory demyelinating polyradiculoneuropathy, acute motor sensory axonal neuropathy, and acute motor axonal neuropathy. A normal electrophysiologic result in the early stages of GBS does not rule out the diagnosis, but a repeat test in 2 to 3 weeks may be helpful, particularly in patients with an atypical presentation [19].
Electrodiagnostic studies, including electromyography and nerve conduction, can differentiate between demyelinating and axonal variants of GBS. Axonal forms of GBS produce decreased sensory and motor amplitudes. Demyelinating forms of GBS produce conduction blocks, temporal dispersion, reduced motor nerve conduction velocity, increased F-wave latency, and prolonged distal motor latency. A spinal MRI can show enhancement and thickening of the cauda equine and intrathecal spinal nerve roots, whereas a brain MRI can show enhancement of the facial, abducens, and oculomotor nerves [20,21].
The first reported case of GBS due to COVID-19 was from Wuhan City, China, where the patient presented with acute leg weakness, which responded to IVIG treatment [22]. Sedaghat et al. reported the case of a patient presenting with bilateral facial palsy and ascending paralysis leading to quadriplegia, which was also managed with IVIG [23]. Virani et al. reported a case of GBS in which the patient presented with diarrhea, tested positive for COVID-19, and responded to IVIG [24]. Toscano et al. reported cases of GBS in which patients who presented with limb weakness and paresthesia followed by facial weakness were also treated with IVIG [25]. Plasma exchange and IVIG are the primary treatments for GBS. Patient recovery is faster, muscle strength improves, and the need for mechanical ventilation decreases when treatment is started early [26].
For COVID-19 cases presenting with neurologic conditions, treatment with immunosuppressant medications leads to worse outcomes. For example, corticosteroids as first-line treatment may prolong viral shedding. Plasma exchange and IVIG are used as second-line treatments for neuroinflammatory crises and have been shown to be beneficial; however, patients should be given prophylaxis therapy for thromboembolism and should be monitored. The use of third-line therapies, such as rituximab or cyclophosphamide, is appropriate when the second-line treatment fails [27].
IVIG has been used as an immunomodulatory and anti-inflammatory treatment for conditions like GBS, chronic inflammatory demyelinating polyneuropathy, multifocal motor neuropathy, and myasthenia gravis. There is no standard mode of action of IVIG because the mechanism of action is dependent on different pathology responses to IVIG. The dose of IVIG is 0.4 g/kg per day, given for 5 days. The common adverse effects of IVIG include headache, back pain, chest pain, fever myalgia, and post-infusion fatigue. The rare adverse effects include aseptic meningitis, rash, acute renal failure, and hyperviscosity, causing a pulmonary embolism, myocardial infarction, or stroke as a thromboembolic event [28].
The proven effective treatments for GBS are IVIG and plasma exchange. It is unclear whether IVIG and plasma exchange are effective in children, cases of mild GBS, or patients with Miller Fisher Variant syndrome. Still, most effectiveness has been seen in adult patients who were unable to walk. One-third of patients received a second treatment with no clinical improvement. Comparing a 5-day and 2-day regimen in children, the children who received a 2-day regimen had more frequent treatment-related fluctuation. In GBS, plasma exchange was as effective as IVIG [29].
Our case is interesting because the patient had bilateral Bell’s palsy as the presenting feature of GBS. Most cases have either had unilateral palsy or weakness of the lower extremities. Treating only Bell’s palsy without investigating the etiology of neurologic emergencies like GBS could lead to permanent disability. This case also highlights the importance of early lumbar puncture to facilitate diagnosis. Several other viruses have been risk factors for GBS, but because our patient came to our hospital during the COVID-19 pandemic, SARS-CoV-2 infection was considered a risk factor. Early treatment with IVIG led to the patient’s complete recovery.
Conclusions
This case report has shown that infection with SARS-CoV-2 can result in acute neurological involvement leading to loss of taste, GBS, and facial weakness. Patients should be managed according to the current clinical guidelines for COVID-19, which continue to be developed. This report has also highlights the importance of the rapid and accurate detection of SARSCoV-2 infection using validated and authorized RT-PCR methods, which have high sensitivity and specificity.
References:
1.. Verma R, Chaudhari TS, Giri P, Unilateral facial palsy in Guillain-Barre syndrome (GBS): A rare occurrence: BMJ Case Rep, 2012; 2012; bcr2012007077
2.. Asadi-Pooya AA, Simani L, Central nervous system manifestations of COVID-19: A systematic review: J Neurol Sci, 2020; 413; 116832
3.. Nepal G, Rehrig JH, Shrestha GS, Neurological manifestations of COVID-19: A systematic review: Crit Care, 2020; 24(1); 421
4.. May M, Klein SR, Differential diagnosis of facial nerve palsy: Otolaryngol Clin North Am, 1991; 24(3); 613-45
5.. Narayanan RP, James N, Ramachandran K, Jaramillo MJ, Guillain-Barré Syndrome presenting with bilateral facial nerve paralysis: A case report: Cases J, 2008; 1(1); 379
6.. Alshekhlee A, Hussain Z, Sultan B, Katirji B, Guillain-Barré syndrome: Incidence and mortality rates in US hospitals: Neurology, 2008; 70(18); 1608-13
7.. Dimachkie MM, Barohn RJ, Guillain-Barré syndrome and variants: Neurol Clin, 2013; 31(2); 491-510
8.. Wu Y, Xu X, Chen Z, Nervous system involvement after infection with COVID-19 and other coronaviruses: Brain Behav Immun, 2020; 87; 18-22
9.. Xydakis MS, Dehgani-Mobaraki P, Holbrook EH, Smell and taste dysfunction in patients with COVID-19: Lancet Infect Dis, 2020; 20(9); 1015-16
10.. Ellul MA, Benjamin L, Singh B, Neurological associations of COVID-19: Lancet Neurol, 2020; 19(9); 767-83
11.. , WHO lists two COVID-19 tests for emergency use, 2020 https://www.who.int/news-room/detail/07-04-2020-who-lists-two-covid-19-tests-for-emergency-use
12.. Li Z, Liu T, Yang N, Neurological manifestations of patients with COVID-19: Potential routes of SARS-CoV-2 neuroinvasion from the periphery to the brain: Front Med, 2020 [Online ahead of print]
13.. Ng Kee Kwong KC, Mehta PR, COVID-19, SARS and MERS: A neurological perspective: J Clin Neurosci, 2020; 77; 13-16
14.. Hughes GB, Practical management of Bell’s palsy: Otolaryngol Head Neck Surg, 1990; 102(6); 658-63
15.. Brenner MJ, Neely JG, Approaches to grading facial nerve function: Semin Plast Surg, 2004; 18(1); 13-22
16.. Herman P, Vincent C, Parietti Winkler C, Consensus statement. Corticosteroid therapy in ENT in the context of the COVID-19 pandemic: Eur Ann Otorhinolaryngol Head Neck Dis, 2020; 137(4); 315-17
17.. Madhok VB, Gagyor I, Daly F, Corticosteroids for Bell’s palsy (idiopathic facial paralysis): Cochrane Database Syst Rev, 2016; 7(7); CD001942
18.. , Criteria for diagnosis of Guillain-Barré syndrome: Ann Neurol, 1978; 3(6); 565-66
19.. Leonhard SE, Mandarakas MR, Gondim FAA, Diagnosis and management of Guillain-Barré syndrome in ten steps: Nat Rev Neurol, 2019; 15(11); 671-83
20.. Uncini A, Kuwabara S, Electrodiagnostic criteria for Guillain-Barrè syndrome: A critical revision and the need for an update: Clin Neurophysiol, 2012; 123(8); 1487-95
21.. Fontes CA, Dos Santos AA, Marchiori E, Magnetic resonance imaging findings in Guillain-Barré syndrome caused by Zika virus infection: Neuroradiology, 2016; 58(8); 837-38
22.. Zhao H, Shen D, Zhou H, Guillain-Barré syndrome associated with SARS-CoV-2 infection: Causality or coincidence?: Lancet Neurol, 2020; 19(5); 383-84
23.. Sedaghat Z, Karimi N, Guillain Barre syndrome associated with COVID-19 infection: A case report: J Clin Neurosci, 2020; 76; 233-35
24.. Virani A, Rabold E, Hanson T, Guillain-Barré syndrome associated with SARS-CoV-2 infection: ID Cases, 2020; 20; e00771
25.. Toscano G, Palmerini F, Ravaglia S, Guillain-Barré syndrome associated with SARS-CoV-2: N Engl J Med, 2020; 382(26); 2574-76
26.. Patwa HS, Chaudhry V, Katzberg H, Evidence-based guideline: Intravenous immunoglobulin in the treatment of neuromuscular disorders: Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology: Neurology, 2012; 78(13); 1009-15
27.. Needham EJ, Chou SH, Coles AJ, Menon DK, Neurological implications of COVID-19 infections: Neurocrit Care, 2020; 32(3); 667-71
28.. Lünemann JD, Nimmerjahn F, Dalakas MC, Intravenous immunoglobulin in neurology – mode of action and clinical efficacy: Nat Rev Neurol, 2015; 11(2); 80-89
29.. Verboon C, Doets AY, Galassi G, Current treatment practice of Guillain-Barré syndrome: Neurology, 2019; 93(1); e59-76
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952041
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953137
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953095
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953308
Most Viewed Current Articles
07 Dec 2021 : Case report
22,760,974
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,540
176,540
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,802
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,859
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133