13 May 2021: Articles 
A 27-Year-Old Lebanese Man with Stomach Perforation and Regurgitation of a Beef Tapeworm (): A Case Report and Review of the Literature
Unusual clinical course, Challenging differential diagnosis, Unusual setting of medical care
Samer Dbouk1ABCDEFG*, Nagham Bazzi2ABCDEFG, Hussein Mcheimeche1ABCDEFG, Mohammad Rida Farhat2DEF, Ali Alameh3BCD, Mohamad Rakka2ABCDEFGDOI: 10.12659/AJCR.928355
Am J Case Rep 2021; 22:e928355






Abstract
BACKGROUND: The global burden of Taenia saginata (T. saginata), the beef tapeworm, includes economic loss, and its pathogenicity is considered mild. T. saginata can infect the human definitive host when people ingest larval cysts from raw or undercooked beef, as cattle are the intermediate host. This report is of a case of gastric perforation and pneumoperitoneum with regurgitation of T. saginata in a 27-year-old Lebanese man, and includes a review of previous cases of gastrointestinal perforation due to T. saginata.
CASE REPORT: We report a rare case of stomach perforation caused by T. saginata, in which the tapeworm was subsequently expelled orally. A computerized tomography (CT) scan was done, revealing pneumoperitoneum and abdominal fluid, which was consistent with evidence of a perforated hollow viscus. Three days after exploratory laparoscopy, the patient vomited a 3-meter tapeworm and the diagnosis was subsequently made. On the fourth day, a CT scan of the abdomen with oral contrast was performed and showed no leakage. A clear fluid diet was started on the fifth day. The patient was discharged home on the seventh postoperative day in good condition. One week after the discharge, the patient was examined; he was in a good condition and symptoms were completely relieved 1 week after worm expulsion.
CONCLUSIONS: This report shows that in countries or societies where eating raw beef is common, a diagnosis of infestation with T. saginata should be considered in patients who present with gastrointestinal symptoms.
Keywords: Parasitic Diseases, peritonitis, Taenia saginata, Cattle, Stomach Diseases, Taeniasis, Vomiting
Background
We report a rare case of stomach perforation caused by
Case Report
A 27-year-old male patient presented to the Emergency Department reporting severe abdominal pain, nausea, and vomiting for 5 days. The patient was afebrile, his blood pressure was 125/75 mmHg, and his heart rate was 105 beats/min. A physical examination revealed high-pitched bowel sounds and diffuse abdominal tenderness with involuntary guarding and rebound tenderness. His pain started 2 months ago with gradual postprandial onset. The pain was prominently in the epigastric area, and then it became diffuse, persistent, aggravated by lying flat, and associated with multiple episodes of nausea and postprandial vomiting. He denied fever, chills, or change in bowel habits. His past medical history included an episode of left-side spontaneous pneumothorax 2 years ago with a subsequent left chest tube placement. The patient did not have a history of stomach ulcer or alcohol intake. He reported taking nonsteroidal anti-inflammatory drugs (NSAIDs) for a short period of time due to dental pain, and smoking 20 packs of cigarettes per year. Notably, the patient stated he had a diet heavy in raw meat consumption (kebbeh nayye, a traditional Lebanese dish) for several years.
A complete blood count showed the following: leukocyte count 12 600/mm, segmented neutrophils 90%, hemoglobin level 14 mg/dl, and hematocrit 30%. Other laboratory test results included sodium 128 mEq/L, potassium 5.1mEq/L, Lipase 250, amylase 240, and serum creatinine 0.9. Liver function test results were within normal limits. A computed tomography (CT) scan of the abdomen and pelvis with intravenous contrast was obtained and was notable for mild pneumoperitoneum and a moderate amount of free fluids in the abdomen and pelvis, which are consistent with evidence of a perforated hollow viscus (Figure 1).
After fluid resuscitation and correction of the electrolyte imbalance, a broad-spectrum antibiotic was started and the patient was then taken to the operating room for urgent exploratory laparoscopy. The abdomen was insufflated using a Veress needle and 3 trocars were then inserted. Exploration revealed a diffuse and moderate amount of purulent fluids in the abdomen and pelvis, with fibrin and pseudomembranes. Thus, after minimal lavage and suction, a 2-cm perforation in the anterior surface of the stomach near the pylorus was identified (Figure 2). The perforation was closed primarily with 3 simple stitches using 2/0 polyglactin, and reinforced with an omental patch. It was then followed by copious peritoneal lavage of the abdominal quadrants in a sequential manner moving from quadrant to quadrant until the effluent was clear. Corrugated drains were then inserted in all 4 abdominal quadrants. The trocars were removed under direct vision, the abdomen was deflated, and the skin incision was closed.
The patient tolerated the operation well and there were no complications. He was transferred to the recovery room in stable condition. Three days after the operation, he vomited a 3-meter-long tapeworm (
The remaining postoperative course was uneventful. A CT scan of the abdomen with oral contrast was performed on the fourth day and showed no leakage.
A clear fluid diet was then started on the fifth day and advanced. The patient was discharged home on the seventh postoperative day in good condition. One week after the discharge, the patient was examined and he was in good condition.
Discussion
This case report suggests that
Among many risk factors for peptic ulcer, NSAIDs and smoking play a pivotal role in developing peptic ulcer disease; they both lead to increased stomach acidity [10]. Knowing that our patient was a smoker and had been taking NSAIDs, peptic ulcer disease was a potential differential diagnosis. It was reported that the possible obstruction mechanism of the tapeworm in the abdomen is caused by a physical obstruction due to long strobila (a chain of segments) of
Similar to our case, symptoms of peptic ulcer disease include abdominal pain that worsens after stomach perforation, bloating, and abdominal discomfort [9]. The most common presenting manifestation of stomach perforation is severe consistent pain; less common symptoms include increased heart rate and respiration rate, fever, sepsis, and confusion [7]. Severe pain and tachycardia were present in our patient.
Imaging techniques for stomach perforation are plain radio-graph, ultrasound, and CT scan; the latter is the most useful and is highly sensitive [8]. Our patient was diagnosed with abdominal perforation using CT scan results. However, the diagnosis of
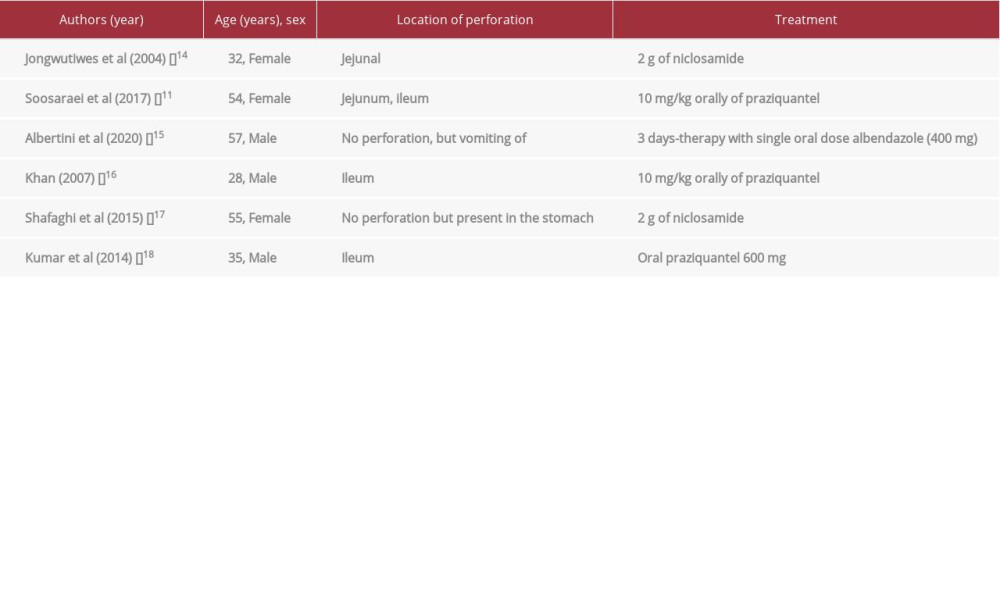
The clinical presentation of
Conclusions
The pathogenicity of
Figures
References:
1.. Eichenberger RM, Thomas LF, Gabriël S: Parasit Vectors, 2020; 13(1); 234
2.. Saratsis A, Sotiraki S, Braae UC: Parasit Vectors, 2019; 12(1); 113-13
3.. Symeonidou I, Arsenopoulos K, Tzilves D, Human taeniasis/cysticercosis: A potentially emerging parasitic disease in Europe: Ann Gastroenterol, 2018; 31(4); 406-12
4.. Braae UC, Thomas LF, Robertson LJ: Parasit Vectors, 2018; 11(1); 518
5.. Jorga E, Van Damme I, Mideksa B, Gabriël S: Parasit Vectors, 2020; 13(1); 375
6.. Bekraki A, Hanna K: J Parasit Dis, 2016; 40(1); 203-4
7.. Langell JT, Mulvihill SJ, Gastrointestinal perforation and the acute abdomen: Med Clin North Am, 2008; 92(3); 599-625
8.. Sigmon DF, Tuma F, Kamel BG, Cassaro S, Gastric perforation: StatPearls, 2020, Treasure Island (FL), StatPearls Publishing
9.. Chung KT, Shelat VG, Perforated peptic ulcer – an update: World J Gastrointest Surg, 2017; 9(1); 1-12
10.. Salih BA, Abasiyanik MF, Bayyurt N, Sander E: World J Gastroenterol, 2007; 13(23); 3245-48
11.. Soosaraei M, Alizadeh S, Fakhar M: Ann Med Surg (Lond), 2017; 24; 74-76
12.. Chiu LW, Soldes OS: Congenital anomalies and surgical disorders of the stomach, 2011, Elsevier
13.. Torgerson PR, Abdybekova AM, Minbaeva G: Parasit Vectors, 2019; 12(1); 175
14.. Jongwutiwes S, Putaporntip C, Chantachum N, Sampatanukul P: J Infect, 2004; 49(4); 324-28
15.. Albertini N, Pecchini F, Esposito S: Int J Surg Case Rep, 2020; 77; S72-74
16.. Khan Z, Small intestinal perforation which is caused by tape worm: Pak J Surg, 2007; 23; 73-5
17.. Shafaghi A, Rezayat KA, Mansour-Ghanaei F, Maafi AA, Taenia: An uninvited guest: Am J Case Rep, 2015; 16; 501-4
18.. Kumar S, Kumar S, Kumar M, Ileal perforation and peritonitis due to taenia a rare case: International Journal of Scientific and Research Publications, 2014; 4(12); 2250-3153
19.. Hakeem SY, Rashid A, Khuroo S, Bali RS: Case Rep Surg, 2012; 2012; 572484
20.. Prasada S, Bhat S, Vidyalakshmi K, Taeniasis: An unusual presentation: J Clin Diagn Res, 2017; 11(6); DD03-04
21.. Sheikh M, Sheikh I, Ali I, Reshi F: The Internet Journal of Surgery, 2007; 16; 77663222
22.. Chang T, Jung BK, Sohn WM: Korean J Parasitol, 2020; 58(2); 201-4
23.. Silva C, Costa-Cruz J: Infect Disord Drug Targets, 2010; 10(5); 313-21
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133