05 February 2021: Articles 
Intermittent High-Frequency Percussive Ventilation Therapy in 3 Patients with Severe COVID-19 Pneumonia
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment
Sergey P. Marchenko1BEF*, Ecaterina Scarlatescu2ABEF, Paul Robert Vogt3AEFG, Alexey Naumov1ABDEF, Sergey Bognenko1ABCDEFDOI: 10.12659/AJCR.928421
Am J Case Rep 2021; 22:e928421






Abstract
BACKGROUND: High-frequency percussive ventilation (HFPV) is a method that combines mechanical ventilation with high-frequency oscillatory ventilation. This report describes 3 cases of patients with severe COVID-19 pneumonia who received intermittent adjunctive treatment with HFPV at a single center without requiring admission to the Intensive Care Unit (ICU).
CASE REPORT: Case 1 was a 60-year-old woman admitted to the hospital 14 days after the onset of SARS-CoV-2 infection symptoms, and cases 2 and 3 were men aged 65 and 72 years who were admitted to the hospital 10 days after the onset of SARS-CoV-2 infection symptoms. All 3 patients presented with clinical deterioration accompanied by worsening lung lesions on computed tomography (CT) scans after 21 days from the onset of symptoms. SARS-CoV-2 infection was confirmed in all patients by real-time reverse transcription-polymerase chain reaction (RT-PCR) assay from nasal swabs. All 3 patients had impending respiratory failure when non-invasive intermittent HFPV therapy was initiated. After therapy, the patients had significant clinical improvement and visibly decreased lung lesions on followup CT scans performed 4–6 days later.
CONCLUSIONS: The 3 cases described in this report showed that the use of intermittent adjunctive treatment with HFPV in patients with severe pneumonia due to infection with SARS-CoV-2 improved lung function and may have prevented clinical deterioration. However, recommendations on the use of intermittent HFPV as an adjunctive treatment in COVID-19 pneumonia requires large-scale controlled clinical studies. In the pandemic context, with a shortage of ICU beds, avoiding ICU admission by using adjunctive therapies on the ward is a useful option.
Keywords: COVID-19, High-Frequency Ventilation, Pneumonia, Viral, COVID-19, Clinical Deterioration, Cough, Dyspnea, Hospitalization, Oxygen Inhalation Therapy, Respiratory Insufficiency, Tomography, X-Ray Computed
Background
Pneumonia caused by COVID-19 with severe acute respiratory syndrome has been reported since December 2019. In addition to real-time reverse transcription-polymerase chain reaction (RT-PCR), lung computed tomography (CT) scan is useful for the diagnosis and monitoring of pneumonia, as the extent of lung impairment on CT correlates with disease severity [1,2]. The most frequent patterns described on lung CT scan in patients with COVID-19 pneumonia are ground-glass opacities (GGO), intralobular and/or interlobular septal thickening, reticular pattern, consolidation, and linear opacities [3–5]. These variable patterns are observed isolated or in combination at different times throughout the disease course. According to recent publications, the extent of lung involvement rapidly increases during the early stages (first 8–9 days from symptom onset), reaching the advanced stage with maximal lung lesions in about 14–21 days after onset of symptoms. Then, after 21–28 days from disease onset (DOD), the extent and intensity of lung lesions decrease (the absorption phase) [6–5]. This is seen in most of the cases with favorable outcomes; however, some patients present worsening lung lesions associated with clinical deterioration 4 weeks from disease onset, and these patients are at risk for respiratory failure and ICU admittance.
In this article, we present 3 cases of hospitalized patients with pneumonia caused by COVID-19 associated with severe acute respiratory syndrome who received intermittent high-frequency percussive ventilation (HFPV) non-invasively using the IPV-2C Percussionnaire Intrapulmonary Percussive Ventilation device (Percussionaire, Sandpoint, ID, USA). HFPV is a method that combines mechanical ventilation with high-frequency oscillatory ventilation. The HFPV technique uses small high-frequency gas pulses, allowing improved oxygen diffusion combined with conventional tidal volume ventilation and convective washout of carbon dioxide [8]. HFPV improves gas exchange and facilitates the recruitment of atelectatic lung areas and the mobilization and drainage of secretions [8]. This technique has been used in neonates and pediatric patients and for burn, lung transplant, and trauma, as well as in acute respiratory distress syndrome (ARDS) as salvage therapy. It has also been used in patients with chronic obstructive pulmonary disease or cystic fibrosis [9–15].
This adjunctive therapy was started in patients receiving regular treatment on the ward, who presented with clinical deterioration accompanied by worsening of their lung lesions on CT scans after 21 days from symptoms onset. After HFPV therapy, all the patients had significant clinical improvement and visibly decreased lung lesions on followup CT scans performed 4–6 days later.
This report describes 3 cases of patients with severe COVID-19 pneumonia who received intermittent adjunctive treatment with HFPV at a single center without requiring admission to the intensive care unit (ICU). SARS-Cov-2 infection was confirmed in all patients by RT-PCR of nasal swabs using the D-5580 RealBest SARS-CoV-2 RT-PCR Assay (Vector Corporation, Moscow, Russia).
Case Reports
CASE 1:
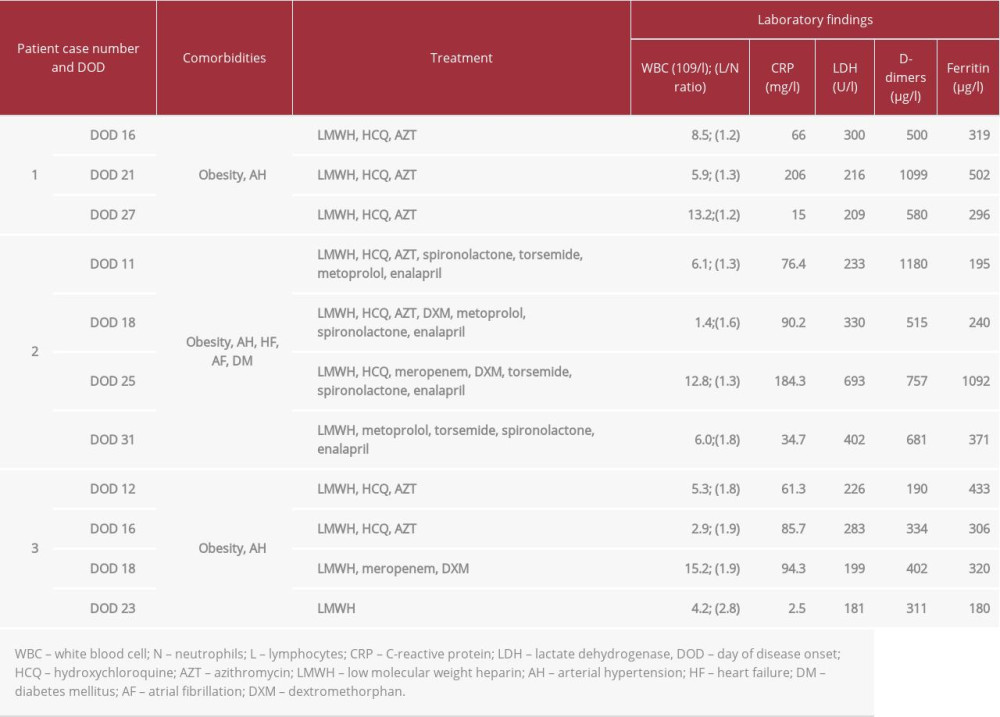
A 60-year-old woman was admitted to hospital on the 14th day from the onset of SARS-CoV-2 infection symptoms with persistent dry cough, weakness, and intermittent fevers. On physical examination, the only distinctive features were signs of dehydration (dry mucous membranes, sinus tachycardia, prolonged capillary refill time, oliguria) and increased blood pressure (158/90 mm Hg). After admission, the patient received standard treatment for COVID-19 as recommended by our hospital protocols in use at that time (Table 1). However, her symptoms worsened (frequent dry coughing, dyspnea, abdominal discomfort, loose stool) and peripheral oxygen saturation dropped to 92% on room air. The worsening of lung lesions with evidence of bilateral lung consolidations was revealed by consecutive lung CT scans performed at 5-day intervals, mirroring the worsening of clinical status (Figures 1A, 2A, 2B). As the patient was clinically deteriorating, with a permanent need for high-flow supplemental oxygen via facial mask and impending respiratory failure, HFPV therapy was started. Noninvasive HFPV was performed at 8-hour intervals for 1 week. After 3 days, her clinical status improved, her supplemental oxygen requirement decreased, and the CT scan performed on DOD 27 revealed an important resolution of her previously severe lung lesions (Figure 2C). Supplemental oxygen was completely discontinued after DOD 29, when her oxygen saturation on room air was 97–99%. She was discharged from the ward, completely asymptomatic, on DOD 33.
CASE 2:
A 65-year-old man was admitted to hospital on the 10th day from the onset of SARS-CoV-2 infection symptoms, with fever, dry cough, dyspnea, tachypnea, peripheral edema, and oxygen saturation of 90% on room air. He had multiple comorbidities (Table 1). Diminished breath sounds and late inspiratory crackles were noted in both lungs on auscultation, reflecting pleural effusions and interstitial lung edema that was confirmed by the lung CT scan (Figure 3A). After admission, besides the standard treatment as recommended by local protocol, the patient received a combination of diuretics and his clinical condition improved, with O2 saturation of 94–95% on room air and visible improvement of the lung CT scan (Figure 3B). However, after 1 week of therapy, he started to deteriorate again with oxygen saturation of 90–91% on room air, dyspnea, and the appearance of a productive cough, while the CT scan on DOD 25 showed bilateral lung consolidation (Figures 1B, 3C). Taking into consideration his clinical status and paraclinical data, extended-spectrum antibiotic and non-invasive intermittent HFPV therapy was started. After 6 days, his clinical status improved, and his C-reactive protein values decreased significantly (Table 1). Moreover, the lung CT scan performed on DOD 31 revealed an important resolution of his severe lung lesions (Figure 3D). Supplemental oxygen was completely discontinued after DOD 32. He was discharged from the ward on DOD 35 with oxygen saturation of 98% on room air and without any respiratory symptoms.
CASE 3:
A 72-year-old man was admitted to hospital on the 10th day from the onset of SARS-CoV-2 infection symptoms, with fever, oxygen saturation of 96% on room air without any cough or dyspnea, and normal lung auscultation. His lung CT scan performed on day 2 after hospital admission revealed lesions (mainly GGO) occupying roughly about 30% of the lung parenchyma (Figure 4A, 4E). He received standard treatment for COVID-19 as recommended by local protocol and he seemed to be undergoing a favorable evolution. However, 1 week after hospital admission, he presented with dyspnea and tachypnea, and his peripheral saturation decreased to 86–88% on room air (Figure 1C). The clinical worsening was mirrored by the extent of lung lesions on the CT scans repeated on DOD 16 and 18 (Figure 4B, 4F – DOD 16 and Figure 4C, 4G – DOD 18). As the patient continued to deteriorate, extended-spectrum antibiotics and corticosteroids were added and non-invasive intermittent HFPV therapy in the prone position was initiated. After 5 days, his clinical status improved and his lung CT scan revealed an important resolution of the severe heterogeneous lung lesions seen on previous CT scans (Figure 4D, 4H). Supplemental oxygen was completely discontinued after DOD 29. He was discharged from the ward on DOD 32 with oxygen saturation of 96% on room air and without any respiratory symptoms.
Discussion
Currently, our understanding of the clinical spectrum of COVID-19 is based on data published by previous authors. The main focus has been to prevent potentially fatal complications from respiratory failure and ARDS due to severe COVID-19 pneumonia, and also from cardiac injury and coagulopathies [16]. Patients with coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and presenting with worsening lung lesions associated with clinical deterioration after 3-4 weeks following disease onset are at high risk for respiratory failure and ICU admittance [16]. For adults with COVID-19 and acute hypoxemic respiratory failure despite conventional oxygen therapy, guidelines suggest using high-flow nasal cannula over conventional oxygen therapy [17]. In patients presenting with clinical deterioration, impending respiratory failure, high inflammatory markers, and extending areas of lung damage, it is very important to undertake timely therapeutic measures for the reduction of interstitial and intra-alveolar edema and recruitment of collapsed alveoli to decrease intra-pulmonary right to left shunting and to improve oxygenation without causing lung over-distention. For this purpose, a therapy using low volumes of air (oxygen) with high frequency (to prevent sharp increases in pressure), high flow (to reach peripheral lung areas), and low pressure (to prevent barotrauma) can be delivered to the heterogeneously damaged lung areas. During the course of viral pneumonia, the lungs present heterogeneous lesions and areas with different compliance. Standard non-invasive ventilator strategies using positive end expiratory pressure recruit non-aerated alveoli, and reduce the inhomogeneity of lung volume distribution, but might cause over-distention of normal alveolar spaces, resulting in barotrauma [18]. HFPV using the Phasitron® device allows the recruitment of collapsed alveoli by delivering the optimal volume and pressure of air required by the alveolar space without over-distention of compartments with normal compliance, a very important issue to consider in mechanically heterogeneous lungs [19].
At the time when HFPV therapy was started, patients were on the ward, but they were oxygen dependent and were clinically deteriorating, with signs of impending respiratory failure. It is important to note that these cases were identified on the basis of clinical picture and repeated lung CT scan to set the indication for more aggressive treatment including HFPV therapy. After HFPV sessions were started, a reduction in the effort needed for breathing and improved gas exchange were clearly observed, while the CT scans also revealed decreased lung lesions. Patients also reported less breathing effort. In this way, further respiratory deterioration and ICU admission were avoided and the management of these severe patients was possible on the ward. In our view, the use of HFPV was beneficial in our patients because it allowed the recruitment of collapsed alveoli using high flow and frequency and accommodating the optimal volume and pressure of air required by the alveolar space. Due to the associated risk of aerosol spreading, non-invasive HFPV was performed in a single room with the minimum number of required healthcare workers wearing adequate personal protection equipment (PPE) to minimize staff exposure.
Conclusions
From our experience, the use of HFPV led to clinical improvement in all our patients. The 3 cases described in this report show that the use of intermittent adjunctive treatment with HFPV in patients with severe COVID-19 pneumonia due to infection with SARS-CoV-2 improved lung function. Further, HFPV may have prevented clinical deterioration. In the pandemic context of ICU bed shortages, avoiding ICU admission by using adjunctive therapies on the ward is extremely important. Therefore, HFPV therapy might be used as adjunctive therapy in deteriorating patients with COVID-19 pneumonia on the ward. Larger studies are needed, however, before making clear and definitive recommendations.
Figures
References:
1.. Yang R, Li X, Liu H, Chest CT severity acore. An imaging tool for assessing severe COVID-19: Radiol Cardiothorac Imaging, 2020; 2(2); e200047
2.. Cheng Z, Qin L, Cao Q, Quantitative computed tomography of the coronavirus disease 2019 (COVID-19) pneumonia: Radiol Infect Dis, 2020; 7(2); 55-61
3.. Shi H, Han X, Jiang N, Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study: Lancet Infect Dis, 2020; 20(4); 425-34
4.. Song F, Shi N, Shan F, Emerging 2019 novel coronavirus (2019-nCoV) pneumonia: Radiology, 2020; 295(1); 210-17
5.. Ding X, Xu J, Zhou J, Long Q, Chest CT findings of COVID-19 pneumonia by duration of symptoms: Eur J Radiol, 2020; 127; 109009
6.. Xiong Y, Sun D, Liu Y, Clinical and high-resolution CT features of the COVID-19 infection: Comparison of the initial and follow-up changes: Invest Radiol, 2020; 55(6); 332-39
7.. Zhou S, Zhu T, Wang Y, Xia L, Imaging features and evolution on CT in 100 COVID-19 pneumonia patients in Wuhan, China: Eur Radiol, 2020; 30(10); 5446-54
8.. Lucangelo U, Fontanesi L, Antonaglia V, High frequency percussive ventilation (HFPV). Principles and technique: Minerva Anestesiol, 2003; 69(11); 841-48 ,848–51
9.. Rizkalla NA, Dominick CL, Fitzgerald JC, High-frequency percussive ventilation improves oxygenation and ventilation in pediatric patients with acute respiratory failure: J Crit Care, 2014; 29(2); 314.e1-7
10.. Chung KK, Wolf SE, Renz EM, High-frequency percussive ventilation and low tidal volume ventilation in burns: A randomized controlled trial: Crit Care Med, 2010; 38(10); 1970-77
11.. Dmello D, Nayak RP, Matuschak GM, High-frequency percussive ventilation for airway clearance in cystic fibrosis: A brief report: Lung, 2010; 188(6); 511-13
12.. Godet T, Jabaudon M, Blondonnet R, High frequency percussive ventilation increases alveolar recruitment in early acute respiratory distress syndrome: An experimental, physiological and CT scan study: Crit Care, 2018; 22(1); 3
13.. Vargas F, Boyer A, Bui HN, Effect of intrapulmonary percussive ventilation on expiratory flow limitation in chronic obstructive pulmonary disease patients: J Crit Care, 2009; 24(2); 212-19
14.. Eastman A, Holland D, Higgins J, High-frequency percussive ventilation improves oxygenation in trauma patients with acute respiratory distress syndrome: A retrospective review: Am J Surg, 2006; 192(2); 191-95
15.. Feltracco P, Serra E, Barbieri S, Noninvasive high-frequency percussive ventilation in the prone position after lung transplantation: Transplant Proc, 2012; 44(7); 2016-21
16.. Bouadma L, Lescure FX, Lucet JC, Severe SARS-CoV-2 infections: Practical considerations and management strategy for intensivists: Intensive Care Med, 2020; 46(4); 579-82
17.. Alhazzani W, Møller MH, Arabi YM, Surviving sepsis campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19): Crit Care Med, 2020; 46(5); 854-87
18.. Navalesi P, Maggiore SM, Positive end-expiratory pressure: Principles and practice of mechanical ventilation, 2006; 273-326, New York, NY, USA, McGraw Hill Medical
19.. Lucangelo U, Accardo A, Bernardi A, Gas distribution in a two-compartment model ventilated in high-frequency percussive and pressure-controlled modes: Intensive Care Med, 2010; 36(12); 2125-31
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133