14 December 2020: Articles 
Three Cases of COVID-19 Pneumonia That Responded to Icosapent Ethyl Supportive Treatment
Unusual or unexpected effect of treatment
Winston Suh1DEF*, Ivan Urits2DEF, Omar Viswanath1345DEF, Alan D. Kaye1DEF, Haresh Patel6DEF, Wade Hall7DEF, Jonathan P. Eskander8DEFDOI: 10.12659/AJCR.928422
Am J Case Rep 2020; 21:e928422






Abstract
BACKGROUND: Icosapent ethyl, a form of eicosapentaenoic acid with anti-inflammatory activity, has been approved as an adjunctive treatment with statins in patients with hypertriglyceridemia. Icosapent ethyl is currently undergoing clinical trials to determine its anti-inflammatory effects in patients with coronavirus disease 2019 (COVID-19). This report describes 3 intensive care unit (ICU) patients with moderate to severe COVID-19 pneumonia treated with icosapent ethyl as part of their supportive care who had favorable outcomes.
CASE REPORT: Case 1 was a 75-year-old man with a past medical history of hyperlipidemia, hypertension, type 2 diabetes mellitus, obesity, and benign prostatic hyperplasia. Case 2 was a 23-year old man with a past medical history of type 2 diabetes mellitus and obesity. Case 3 was a 24-year old man with a history of autism. All cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection were confirmed from a nasopharyngeal swab using the Becton Dickinson nasopharyngeal reverse-transcription polymerase chain reaction. All patients in these cases were treated with a course of 2 g of icosapent ethyl twice a day by nasogastric tube.
CONCLUSIONS: This report of 3 cases describes the use of icosapent ethyl as a component of supportive treatments in ICU patients with moderate to severe COVID-19 pneumonia. However, as of yet there are no evidence-based treatments for SARS-CoV-2 infection from controlled clinical trials. The outcomes of ongoing clinical trials are awaited to determine whether icosapent ethyl has anti-inflammatory effects in patients with SARS-CoV-2 infection and which patients might benefit from the use of this adjunctive treatment.
Keywords: COVID-19, eicosapentaenoic acid, COVID-19, young adult
Background
The new strain of coronavirus, labeled severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is at the heart of an ever-growing coronavirus disease 2019 (COVID-19) pandemic. In addition to the fact that more than 14 million confirmed cases have been reported, the actual burden of the virus has been shown to be underestimated; of the numerous confirmed cases, there is a substantially greater amount of people that have actually been exposed or infected by the virus [1]. In recent studies, the actual immunopathogenesis and development of severe lung and occasional systemic disease after infection have been shown to closely follow the immune response. Specifically, research shows that corona-virus expresses surface proteins that activate the NLRP3 inflammasome, subsequently activating caspases, interleukins (ILs), and causing the release of proinflammatory cytokines, thus inducing pyroptosis, a highly inflammatory mechanism of cell death when compared with the usual neat and orderly process of apoptosis [2,3]. Thus, the respiratory sequelae morbidity commonly associated with SARS-CoV-2 infection are not solely caused by the viral infection itself, but also by an over-activated inflammatory host immune response, marked by an overall increase in inflammatory markers [4,5]. By that logic, anti-inflammatory therapy may be a driving point in combating SARS-CoV2-related disease.
Indeed, such therapy involving corticosteroids and other immunosuppressants has been proposed, and clinical trials are well underway [4,5]. One such ongoing clinical trial (NCT04412018) (with an estimated completion date of December 2020) addresses the effects of icosapent ethyl on inflammatory biomarkers in individuals with COVID-19 by looking at outcome measures such as changes to high-sensitivity C-reactive protein (hs-CRP) and the neutrophil-lymphocyte ratio [6]. Currently, icosapent ethyl, a form of eicosapentaenoic acid, is indicated for the treatment of hypertriglyceridemia in patients at risk for ischemic heart disease and as an adjunctive treatment with maximally tolerated doses of statin therapy [7,8]. Regulatory approval for adjunctive treatment of hypertriglyceridemia has been supported by the findings from the ANCHOR (NCT01047501) and the MARINE (NCT01047683) trials, showing a reduction in inflammatory markers in treated patients [9–11]. Apart from treatment for hypertriglyceridemia, it has been shown to have continued anti-inflammatory activity, as determined by the measurement of certain biomarkers of inflammation [12].
Although there have been multiple studies performed concerning icosapent ethyl’s anti-inflammatory activity in the treatment of hypertriglyceridemia, the mechanism of icosapent ethyl in dealing with COVID-19-induced inflammation remains speculative. One such hypothesis looks at the potential for icosapent ethyl to suppress tumor necrosis factor (TNF)-alpha and IL-1beta messenger ribonucleic acid expression in alveolar macrophages from asthmatic individuals [13]. Another hypothesis examines how inappropriate neutrophil activation can result in acute lung injury, and how Resolvin E1, a derivative of eicosapentaenoic acid, promotes neutrophil apoptosis and thus reduces lung morbidity [14]. Given that previously mentioned studies have shown lung and systemic disease from SARS-CoV-2 infection to be cytokine and immune mediated, these are several possibilities by which icosapent ethyl can be used to modulate the course of COVID-19. Thus, perhaps immersion pulmonary edema (IPE) shows maximum benefit in patients with severe and persistent lung inflammation.
Although icosapent ethyl is not currently approved as an anti-inflammatory treatment in patients with COVID-19, a recently reported case series did show some beneficial effects in reducing symptom severity [15]. Similarly, our case series describes 3 intensive care unit (ICU) patients with moderate to severe COVID-19 pneumonia treated with icosapent ethyl as part of their supportive care who had favorable outcomes with a reduction in inflammatory markers. None of the patients listed in the following cases has been recruited to any other ongoing clinical trials.
Case Reports
CASE 1:
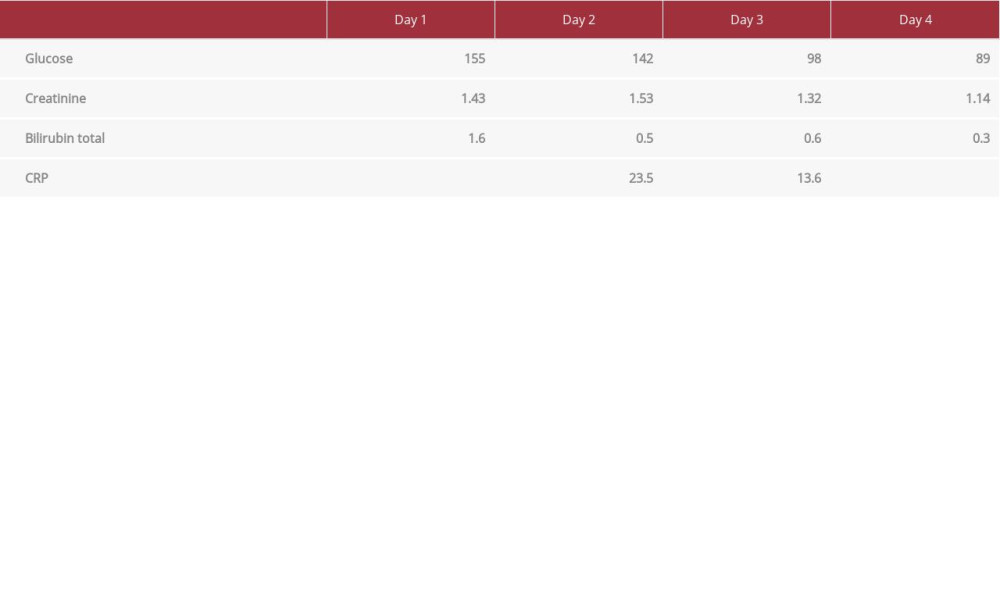
A 75-year-old man with a past medical history of hyperlipidemia, hypertension, diabetes mellitus type 2 requiring insulin, obesity, and benign prostatic hyperplasia was admitted to the hospital for a perirectal abscess. During admission, he was tested and discovered to be positive for COVID-19, and he confirmed subjective fever, altered mental status (memory loss and difficulty thinking), and hypoxia with chest tightness. A chest X-ray demonstrated a focal right basal infiltrate suggestive of COVID-19 pneumonia (Figure 1). He was taken to the operating room for drainage 24 h after admission to the hospital, and that evening he was started on icosapent ethyl 2 g twice a day by NG tube. After the procedure, he was transferred to the ICU for hypoxia and continued systemic inflammatory response syndrome criteria. Two days later, he stated that his symptoms had totally subsided except for pain near the surgical site. Remarkably, his laboratory results reflected this improvement. Before treatment with icosapent ethyl, his creatinine was 1.43 and CRP was 23.5. After 2 days, these numbers improved to 1.14 and 13.6, respectively (Table 1, Figure 2). Additionally, he was no longer febrile, tachycardic, tachypneic, or hypoxic. He left the ICU after 2.5 days of treatment with icosapent ethyl and antibiotics.
CASE 2:
On July 2. 2020, a 23-year old man with a past medical history of obesity and diabetes presented to the ICU with acute kidney injury (AKI), hypoxia, hypercapnia, respiratory failure secondary to COVID-19, and on noninvasive positive-pressure ventilation with bilevel positive airway pressure (BiPAP) with fraction of inspired oxygen of 100% because of acute respiratory distress syndrome (ARDS) along with obesity and hypoventilation that exacerbated COVID-19-induced hypoxia. Upon admission, the patient had a creatinine of 3.06. Aspartate aminotransferases (AST) and alanine aminotransferases (ALT) were also elevated at 949 U/L and 1208 U/L, respectively. On July 3 and 4, the patient was treated with tocilizumab, remdesivir, epoprostenol, and convalescent plasma. Acute-phase reactants began trending down on July 4. The patient was weaned off epoprostenol therapy on July 7, whereas he was transitioned to high-flow nasal cannula during daytime with BiPAP at night because of severe morbid obesity. Icosapent ethyl 2 g twice a day by NG tube was also started on this day. The patient began weaning off the high-flow nasal cannula on July 8. The chest X-ray continued to show severe bilateral effusions and infiltrates consistent with ARDS (Figure 3), but because of suspect fluid overload, the patient was continued on Lasix for diuresis with tracking of fluid intake and urine output. The patient completed broad-spectrum antibiotics on July 9; the nephrologist signed off for the patient’s AKI on July 9, whereas the infectious disease specialist signed off on July 10. At the time of nephrolo-gist sign-off, the patient had a creatinine of 0.78. AST and ALT were also at 18 U/L and 122 U/L, respectively. The patient presented to the hospital with AKI, presumably due to COVID-19. The work-up was minimal so the actual cause of AKI, given its rapid resolution, is not clear. Bilateral lower-extremity duplex scan was negative for deep vein thrombosis (DVT), decreasing suspicion for pulmonary embolism or venous thromboembolism. The patient was continued on high-intensity DVT prophylaxis with supportive care, a steroid course (solumedrol), and probiotics because of frequent bowel movements. By July 10, chest X-rays began improving, acute-phase reactants were near baseline (Table 2, Figure 4), and supportive care was continued. Provided these laboratory results, worsening viral load was not suspected and ARDS was suspected in the setting of COVID-19 pneumonia. The patient continued to do well on BiPAP HS and Vapotherm/high-flow nasal cannula during the day and displayed good diuresis. The patient was also having issues with hyperglycemia and had been meeting with the diabetes team. The patient was removed from the ICU on July 14 and discharged on July 24 after 22 days.
CASE 3:
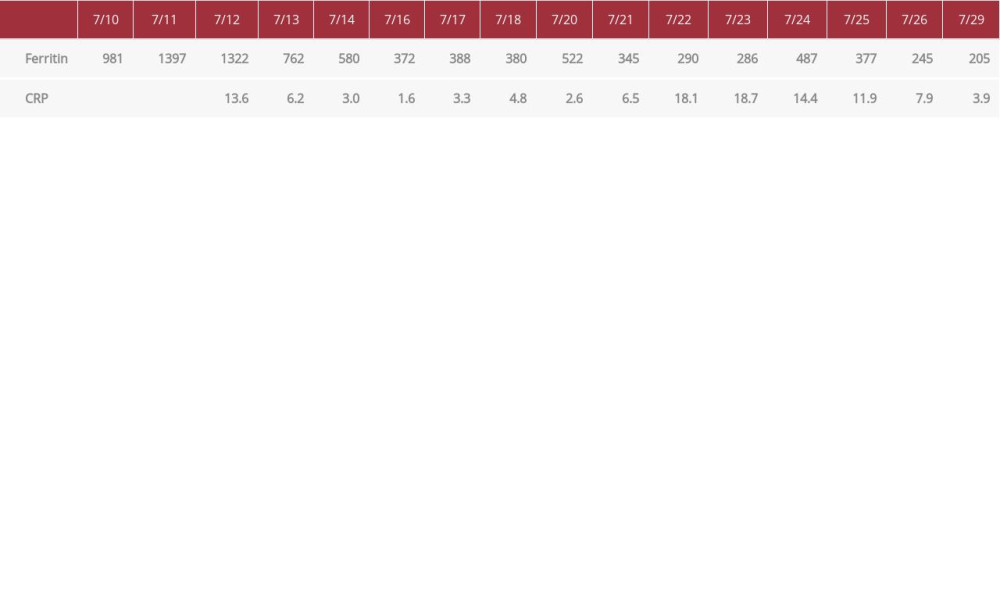
A 24-year old man with a past medical history of autism contracted COVID-19 at his group home, and diagnosis of infection was confirmed by PCR. Subsequently, he was admitted to the ICU and intubated for respiratory distress. He developed ARDS in the setting of COVID-19 pneumonia on July 10. The patient was treated with tocilizumab, remdesivir, epoprostenol, dexamethasone, and convalescent plasma. Icosapent ethyl was given from July 11 to July 14, mistakenly discontinued from July 15 to July 19, and subsequently restarted on July 20 after he developed severe pulmonary inflammation secondary to COVID-19. Of interest, when this patient was taking icosapent ethyl as an adjunct, inflammatory markers and acute-phase reactants trended toward near baseline only after 3 days of administration (Table 3, Figure 5). During the time in which this patient was not taking icosapent ethyl, his inflammatory markers increased in conjunction with his ventilatory requirement and he required significant supportive measures. In addition to broad-spectrum antibiotics, icosapent ethyl appeared to be responsible for his improvement from septic shock, and once again, acute-phase reactants and ventilatory requirements were significantly decreased in just 3.5 days. He was discharged to rehabilitation on August 7.
Discussion
In this clinical presentation, we have described 3 cases; in 1, a 75-year-old patient presented for an abscess but soon developed ARDS secondary to COVID-19. Two days after administration of icosapent ethyl, inflammatory markers improved, and he was moved from the ICU. In the second case, a 23-year-old man presented with ARDS and respiratory failure also due to COVID-19. Inflammatory markers began trending down after administration of antiviral therapy, immunosuppressive therapy, and convalescent plasma but the patient was still being considered for intubation before administration of icosapent ethyl. However, 3 days after the addition of icosapent ethyl as an adjuvant, the patient’s chest X-ray resolved, and acute-phase reactants declined to near baseline levels. In the third case, a 24-year-old man was intubated for ARDS secondary to COVID-19. His case is notable in that he only demonstrated improvement while taking icosapent ethyl.
Icosapent ethyl, as previously stated, is indicated for the treatment of persistent hypertriglyceridemia and has also been shown to reduce the risk of major coronary events [7]. The reduction in such events has been shown to occur with only a marginal reduction in triglyceride levels, as seen in the Japan EPA Lipid Intervention Study and the icosapent ethyl REDUCE-IT trial, suggesting that the therapeutic effects may be related to its anti-inflammatory mechanisms [17]. Indeed, a significant reduction in inflammatory markers with icosapent ethyl has been shown in the ANCHOR and MARINE trials with applications to a variety of other diseases including metabolic syndrome [11] and chronic kidney disease (CKD) [18]. Specifically, studies have shown that icosapent ethyl significantly lowers levels of, among other markers, hsCRP levels compared with placebo [11,12]. With COVID-19, prominent causes of mortality, including pneumonia and ARDS, have been shown to be associated with elevated inflammatory markers including CRP, ILs, granulocyte colony-stimulating factors, interferons, and TNFs that cause pulmonary inflammation and lung damage [5,19]. As serum levels of cytokines have been shown to directly correlate with severity of the infection in COVID-19 patients, pharmacotherapy such as dexamethasone, corticosteroids, and IL antagonists such as tocilizumab have shown therapeutic effect in COVID-19 treatment [20], supporting the possibility of using icosapent ethyl as another potential form of treatment.
We presented 3 patients infected with SARS-CoV-2 who developed hypoxia with infiltrates on imaging, suggestive of ARDS secondary to COVID-19 pneumonia [21]. With icosapent ethyl and antibiotics alone, the 75-year-old patient improved remarkably, quantitively assessed by a reduction in his creatinine and CRP, with resolution of his tachycardia, tachypnea, and hypoxia. The 23-year-old benefitted initially with an immunosuppressive and antiviral regimen, followed by complete resolution of his chest X-ray and acute-phase reactants near baseline just 3 days after addition of icosapent ethyl. The 24-year-old showed improvement primarily while taking icosapent ethyl as an adjunct during his ICU stay. These findings were reflected in their laboratory results, suggesting the role of inflammation in the immunopathology of COVID-19 pulmonary disease and treatment.
In addition to these findings, a more recently published 2-case series involving a 53-year-old woman and her 21-year-old healthy daughter showed some similar beneficial effects of icosapent ethyl in reducing symptoms in COVID-19 patients [15]. Both the mother and the daughter had similar genetic and medical backgrounds and only differed in age. After exposure to SARS-CoV-2 and the development of similar symptoms, both were treated with similar symptomatic care, but only the mother received icosapent ethyl. Although the mother’s symptoms resolved by symptom day (SD) 7, the daughter’s symptoms resolved only on SD18 [15]. This case series demonstrated the relative reduced duration of symptoms when icosapent ethyl was added to a treatment regimen, speaking to its anti-inflammatory capabilities, specifically with COVID-19 patients. With regard to our own cases, it is important to note that cases 2 and 3 demonstrated more severe COVID-19 pneumonia with more extensive supportive treatments compared with those of case 1. Thus, although the actual effect of IPE is more unclear and difficult to interpret in these contexts, the correlation between time of initiation of icosapent ethyl and rapid clinical improvement can be appreciated in all 3 cases. Similar to what was seen in the recent 2-case series, rapid improvement of symptoms after icosapent ethyl administration demonstrates its likely immunomodulatory effects and the immunopathogenesis of COVID-19.
Conclusions
This report of 3 cases describes the use of icosapent ethyl as a component of supportive treatments in ICU patients with moderate to severe COVID-19 pneumonia. However, as of yet there are no evidence-based treatments for SARS-CoV-2 infection from controlled clinical trials. The outcomes of ongoing clinical trials are awaited to determine whether icosapent ethyl has anti-inflammatory effects in patients with SARS-CoV-2 infection and which patients might benefit from the use of this adjunctive treatment.
Figures

References:
2.. Yang M, Cell pyroptosis, a potential pathogenic mechanism of 2019-nCoV infection. SSRN: Electron J, 2020
3.. Yap JKY, Moriyama M, Iwasaki A, Inflammasomes and pyroptosis as therapeutic targets for COVID-19: J Immunol, 2020; 205(2); 307-12
4.. Tay MZ, Poh CM, Rénia L, The trinity of COVID-19: Immunity, inflammation and intervention: Nat Rev Immunol, 2020; 20; 363-74
5.. McGonagle D, Sharif K, O’Regan A, Bridgewood C, The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease: Autoimmun Rev, 2020; 19(6); 102537
6.. Verma S, An investigation on the effects of icosapent ethyl (VascepaTM) on inflammatory biomarkers in individuals with COVID-19 https://clinical-trials.gov/ct2/show/NCT04412018
7.. Bhatt DL, Steg PG, Brinton EA, Rationale and design of REDUCE-IT: Reduction of cardiovascular events with icosapent ethyl – intervention trial: Clin Cardiol, 2017; 40(3); 138-48
8.. , Vascepa guidelines | Vascepa® (icosapent ethyl), 2020 https://vascepahcp.com/guidelines/
9.. Miller M, Ballantyne CM, Bays HE, Effects of icosapent ethyl (eicosapentaenoic acid ethyl ester) on atherogenic lipid/lipoprotein, apolipoprotein, and inflammatory parameters in patients with elevated high-sensitivity C-reactive protein (from the ANCHOR Study): Am J Cardiol, 2019; 124(5); 696-701
10.. Brinton EA, Ballantyne CM, Bays HE, Effects of icosapent ethyl on lipid and inflammatory parameters in patients with diabetes mellitus-2, residual elevated triglycerides (200–500 mg/dL), and on statin therapy at LDL-C goal: The ANCHOR study: Cardiovasc Diabetol, 2013; 12; 100
11.. Bays HE, Ballantyne CM, Braeckman RA, Icosapent ethyl (eicosapentaenoic acid ethyl ester): Effects upon high-sensitivity C-reactive protein and lipid parameters in patients with metabolic syndrome: Metab Syndr Relat Disord, 2015; 13(6); 239-47
12.. Bays HE, Ballantyne CM, Braeckman RA, Icosapent ethyl, a pure ethyl ester of eicosapentaenoic acid: Effects on circulating markers of inflammation from the MARINE and ANCHOR studies: Am J Cardiovasc Drugs, 2013; 13; 37-46
13.. Mickleborough TD, Tecklenburg SL, Montgomery GS, Lindley MR, Eicosapentaenoic acid is more effective than docosahexaenoic acid in inhibiting proinflammatory mediator production and transcription from LPS-induced human asthmatic alveolar macrophage cells: Clin Nutr, 2009; 28(1); 71-77
14.. El Kebira D, Gjorstrup P, Filepa JG, Resolvin E1 promotes phagocytosis-induced neutrophil apoptosis and accelerates resolution of pulmonary inflammation: Proc Natl Acad Sci USA, 2012; 109(37); 14983-88
15.. Berger AA, Sherburne R, Urits I, Icosapent ethyl – A successful treatment for symptomatic COVID-19 infection: Cureus, 2020; 12(9); e10211
16.. , Use of laboratory methods for SARS diagnosis https://www.who.int/csr/sars/labmethods/en/
17.. Harris WS, Understanding why REDUCE-IT was positive – mechanistic overview of eicosapentaenoic acid: Prog Cardiovasc Dis, 2019; 62(5); 401-5
18.. Vijayaraghavan K, Szerlip HM, Ballantyne CM, Icosapent ethyl reduces atherogenic markers in high-risk statin-treated patients with stage 3 chronic kidney disease and high triglycerides: Postgrad Med, 2019; 131(6); 390-96
19.. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 8(5); 475-81
20.. Ye Q, Wang B, Mao J, The pathogenesis and treatment of the ‘cytokine storm’ in COVID-19: J Infect, 2020; 80(6); 607-13
21.. Siegel M, Acute respiratory distress syndrome: Clinical features, diagnosis, and complications in adults https://www.uptodate.com/contents/acute-respiratory-distress-syndrome-clinical-features-diagnosis-and-complications-in-adults
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133