02 August 2021: Articles 
Scurvy as an Alarm Bell of Autistic Spectrum Disorder in the First World: A Case Report of a 3-Year-Old Girl
Challenging differential diagnosis, Unusual setting of medical care, Patient complains / malpractice, Rare disease
Maria Liuzzo Scorpo1ABEF, Giovanni Corsello1CD, Maria Cristina Maggio1ABCDEF*DOI: 10.12659/AJCR.930583
Am J Case Rep 2021; 22:e930583






Abstract
BACKGROUND: Scurvy secondary to deficiency of vitamin C is a rare condition in children. The polymorphism of clinical signs and symptoms makes scurvy diagnosis a challenge for the pediatrician.
CASE REPORT: A 3-year-old girl came to our observation because she refused to walk and to stand, she showed petechiae, follicular hyperkeratosis on the limbs, and bleeding gums. After a physical exam, laboratory tests, and X-ray examinations, we suspected scurvy disease and started treatment with vitamin C. During the hospitalization, some relationship difficulties of the little girl emerged such as absence of eye contact, smiling and laughter without reason, solitary play activities, poor interaction with strangers, non-communicative language, and gestural stereotypes. Therefore, we suspected an autism spectrum disorder, which is often associated with vitamins intake deficiency secondary to food selectivity. After the administration of vitamins, there was a clinical improvement. Due to the suspicion of autism spectrum disorder, the neuropsychiatric team started neuro-psychomotor and speech therapy.
CONCLUSIONS: This case shows that although the incidence of scurvy has been greatly reduced in Western Europe, this pathology can still manifest itself, especially in vulnerable children, and its prompt diagnosis and therapy are important considering the excellent response to treatment.
Keywords: Ascorbic Acid Deficiency, Autistic Disorder, Scurvy, Ascorbic Acid, Autism Spectrum Disorder, Child, Preschool, Vitamins, Walking
Background
Scurvy secondary to vitamin C deficiency is a rare condition in pediatric patients. The polymorphism of clinical signs and symptoms makes scurvy difficult to detect. The role of vitamins in humans is essential. Above all, vitamin C is necessary for collagen synthesis, promoting the hydroxylation of excess proline and lysine in the procollagen, stabilizing the triple helix of collagen. Unlike most mammals, primates do not have enzyme systems to convert glucose into ascorbic acid or vitamin C, which must therefore be obtained by diet (especially fresh fruits and vegetables). In addition, its intake promotes the intestinal absorption of iron. It is also involved in tetrahydrofolic acid formation, neurotransmitters synthesis, and pros-taglandins metabolism [1]. Several case reports describe children affected by scurvy in association with iron overload with medical conditions such as drepanocytic anemia and thalassemia or bone marrow transplantation (excess iron deposits, in fact, accelerate ascorbic acid catabolism) [2]. Vitamin C in-take depends on food preparation, as oxidation can destroy active vitamin C [3]. Although scurvy is currently considered rare in Western countries, it can still be diagnosed in the elderly, patients with mental retardation and psychiatric disorders, or in patients who follow a selective diet [4]. Furthermore, scurvy continues to be diagnosed in children with medical or developmental diseases with restricted diets. Diagnosis can be challenging given the supposed rarity of the disease and nonspecific symptoms, including gingival disease, arthralgia, and petechiae.
In infancy, vitamin C deficiency is diagnosed exclusively in children fed plant-based formula, in children with oral aversion, autism, restricted diets, and cerebral palsy.
Scurvy can present with purpuric rash, nonspecific limp, or bone pain in children with a restricted diet secondary to developmental delay. These children, in fact, choose to consume only a few foods and reject all others, with a ritual and a stereotyped approach to taste, consistency, colors, and smell of selected foods.
In patients with these conditions and in children with a restricted diet secondary to a refusal to eat solid food and/or fresh fruits and vegetables, accurate nutritional counseling and diet prescriptions are mandatory to avoid scurvy. In fact, the diagnosis of scurvy is often complex and requires an accurate differential diagnosis, excluding rheumatologic, neurologic, hematologic, and neoplastic diseases. The differential diagnosis approach requires several hematological evaluations and imaging by echography, traditional radiography, magnetic resonance, and computed tomography, with a significant increase in costs and in discomfort for the patients and their families. These conditions, in fact, require a nutritional approach after diagnosis of the disease, obtaining an improvement in the global assessment of the patients’ care [3–5].
In this report, we describe a case of scurvy in a 3-year-old girl, associated with autism spectrum disorder that was diagnosed only during hospitalization. In fact, it is widely reported in the literature that 46%–89% of children with autism spectrum disorder manifest food selectivity, preferring carbohydrates, snacks, and processed foods, and rejecting fruits and vegetables. Subsequently, a micro- and macro-nutrients deficit results months later and becomes apparent only when symptoms arise [4]. In addition, the objective of this case report is to show that an early diagnosis is very important because scurvy can be treated with an integration of vitamin C and a varied diet, avoiding the development of complications such as bleeding, arthralgia, and delayed growth. Scurvy and other vitamin or micronutrient deficiencies are a possible manifestation of malnutrition in the First World, and the risk of malnutrition is high in children with autism spectrum disorder, involving several metabolic and enzymatic pathways.
Autism spectrum disorder, when it is present, needs neuropsychiatric care to promote social interaction and interests and the development of communicative language improving the quality of life beginning in childhood.
Signs of autism spectrum disorder are a lack in social-communication abilities, low interest in play and inadequate interaction with caregivers, unsatisfactory age-related activities and sensory behaviors, and communication deficits.
However, medical complications allow a diagnosis in some children with a mild phenotype, and guide the diagnosis starting from an organic feature, with an unexpected link with autistic spectrum disorder.
Case Report
We describe the clinical case of a 3-year-old girl born at 37.5 weeks. Her weight at birth was 2340 g (8th percentile) and length was 47 cm (28th percentile).
She was taken to the Emergency Department because, in the previous 2 weeks, she had difficulties walking (caused by lower-limb pain), mild bleeding gums, petechiae, and follicular hyperkeratosis on the upper and lower limbs. Therefore, the admission to the pediatric emergency area was required for diagnosis and adequate treatment. A careful anamnesis showed that she did not have a varied diet, but cow’s milk and biscuits were her favorite foods. However, the little girl did not manifest gastrointestinal symptoms such as abdominal pain, gastro-esophageal reflux, stypsis, vomiting, and/or diarrhea. Furthermore, she had a good appetite, even if associated with selective feeding, limited to liquids or semi-liquid nutriments. In addition, the mother had not administered vitamin supplements to her in the previous year.
For the lower-limb pain, she was treated with ibuprofen at home, without benefit. At the physical examination, she had a forced position with lower limbs flexed to 90 degrees with abduction of the lower right limb, and any attempt to relax the joints made her cry. The presence of muscular hypotrophy in the lower limbs was associated with important functional impotence. Her general condition was very compromised.
Overall, she appeared pale and suffering. At the admission to the pediatric ward, her weight was 12 kg (9th percentile), her length was 95 cm (35th percentile), and her body mass index was 13.3 kg/m2 (0.2 percentile, indicating a condition of underweight). The presence of rachitic rosary at the level of costochondral junctions and a severe psychomotor delay were evident. Therefore, during the hospitalization, laboratory tests, X-rays, abdominal echography, and extensive neuropsychiatric and psychological consultations were performed. In particular, laboratory tests showed mild microcytic anemia (hemoglobin: 11.6 g/dl, mean corpuscular volume 74.2 fl, red blood cells: 4 620 000/mmc), an increase of white blood cells (white blood cells: 8500/mmc (neutrophil percentage: 56%; lymphocyte percentage: 33.9%), and slightly high inflammatory indices (C-reactive protein 1.41 mg/dl). Liver function, kidney function, urine test, osteocalcin, electrolytes, and uric acid levels were within normal ranges.
The X-ray of the chest, performed to show rachitic rosary at the level of costochondral junctions, demonstrated the presence of bilateral pulmonary opacification; in fact, for this reason and due to the mild increase of white blood cells and C-reactive protein, she was started on antibiotic therapy.
The X-ray of the lower limbs was performed because she had pain on movement and a severe functional limitation of the lower limbs. Hence, a modest reduction in the calcium content, more marked in the epiphysis, with the presence of some radi-opaque streak, were documented. A separation of the epiphyses, a transverse metaphyseal band of reduced bone density, and marginal irregularities of the metaphyses with parcel fractures were also present (Figures 1, 2). An ultrasound of the lower limbs was required to perform further diagnostic investigations, which excluded the presence of bilateral joint effusion.
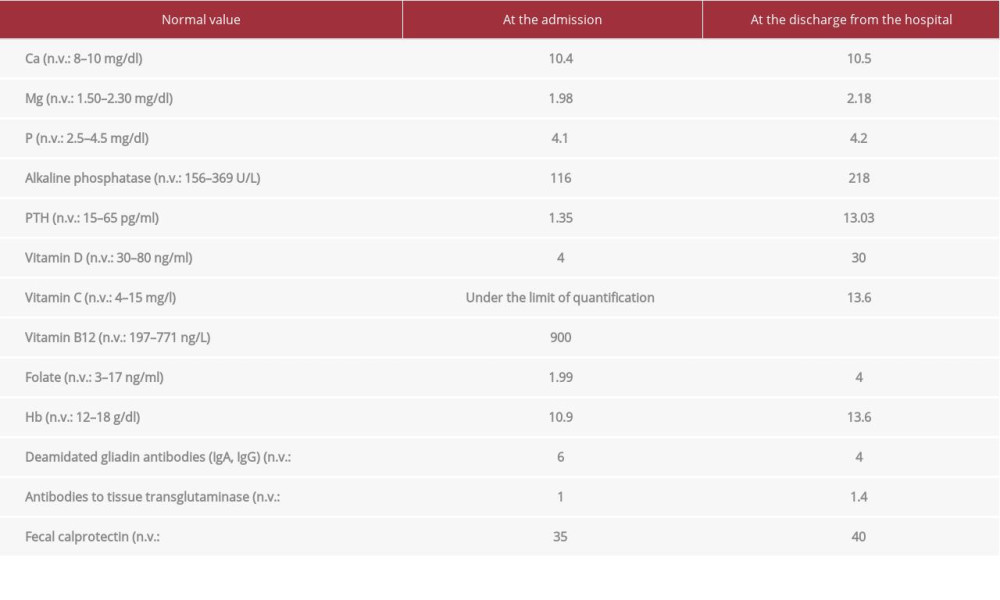
During the hospitalization, she showed absence of eye contact, smiled and laughed without reason, had solitary play activities, poor interaction with strangers, non-communicative language characterized by repetitive and incomprehensible sounds, and stereotyped gestures; these features could be compatible with an autism spectrum disorder, which is often associated with a selective nutrition. Therefore, the severe malnutrition, mild bleeding gums, petechiae and follicular hyperkeratosis on the upper and lower limbs, the exclusive use of milk and biscuits, the presence of radiological findings of scurvy, the suspension of vitamin supplements in the last year, and the features of autism spectrum disorder led to suspicion of vitamin deficiency. Therefore, vitamin C, D, B12, and folates were administered. In fact, vitamin levels were lower than the normal range, in particular vitamin D, folate, and vitamin C, but the level of vitamin B12 was in the normal range (Table 1). We also assessed immunological markers for celiac disease like deamidated antigliadin antibodies (AGA) and anti-transglutaminase antibodies, IgA, IgG, fecal occult blood,
For the vitamin deficiencies, oral administration of ascorbic acid (vitamin C) and vitamin D3 were started at the dosage of 100 mg×3/day and 1.000 UI/day, respectively. After the administration of the first cycle of vitamins and folate, an improvement of the general symptoms was observed, with reduction of bleeding gums, disappearance of musculoskeletal pain, muscle relaxation, and gradual recovery of leg motility. One week after starting treatment, the vitamin levels were in the normal range (Table 1). Gradual food reintroduction was started with the nutritionist counseling. Finally, after a multidisciplinary evaluation by a team composed of a psychologist, a physiotherapist, a neuropsychiatrist, and a speech therapist, neuro-psychomotor and speech therapy were started to promote social integration and language development of the little girl.
Discussion
Our patient had hypovitaminosis (particularly vitamin C deficiency) derived from a limited diet, secondary to rejection of foods and disorders of the relational sphere. This condition allowed us to suspect an important neuro-psychomotor disease that had not yet been identified and that had a significant social and economic impact [2]. This led to the suspicion of autism spectrum disorder, thanks to the observation of the attitude of the little girl during hospitalization and the food selectivity that, as previously reported, is often associated with these disorders. Autism spectrum disorder is a neurodevelopmental disease characterized by deficits in social interaction and communication, and repetitive, stereotyped behavioral patterns [5]. It is widely reported in the literature that 46–89% of children with autism spectrum disorders have diet selectivity, avoiding fruits and vegetables that are rich of vitamin C and minerals. Therefore, a restrictive diet for a long time may lead to health risks in growing children due to micro- and macro-nutrients deficiency [4,5].
In the literature, hypovitaminosis C has also been reported in children fed exclusively with pasteurization milk derivatives that denature ascorbic acid. Breast milk, on the other hand, contains an adequate amount of it [3].
The collagen alterations resulting from vitamin C deficiency explain the manifestations of scurvy: the main symptoms are stomatological deformations and tooth loss, vascular fragility that causes bleeding and bruising, and bone alterations and skin alterations related to poor keratin quality. The initial manifestations are nonspecific: irritability, lack of appetite, and fever. However, skin manifestations including petechiae, bruising, perifollicular hemorrhaging, gingivitis, hyperkeratosis and altered healing of wounds start later [4]. The main systemic signs are asthenia, weight loss, inappetence, and anxiety [4,6]; anemia is often mainly due to concomitant iron and folic acid deficiency [6]. In this case, the child showed mild microcytic anemia, but ferritin and transferrin levels were in the normal range. Musculoskeletal manifestations are found in 80% of such patients; symptoms are late and consist of swelling and joint pain, myalgia, muscle hypotrophy, and fractures. In childhood, musculoskeletal manifestations are frequent, including arthritis, myalgia, hemarthrosis, muscle hemorrhaging, and subperiosteal hematomas. The lower limbs and especially the knees are mainly affected [4,6]. The clinical characteristics of vitamin C deficiency may overlap with some systemic diseases that mimic rheumatological, infectious, or hemato-logical disorders such as rheumatic fever, juvenile idiopathic arthritis, osteomyelitis, meningococcal sepsis, vasculitis, and leukemia [3,4,7].
The daily requirement of vitamin C in children varies greatly with age. In adults, it is 40 mg/day. Demand increases in feverish diseases and diarrhea. Prolonged cooking of the food denatures and alters its intake [8].
In our case the suspicion of vitamin deficiency was placed according to the general conditions, the poor growth of the child, and symptoms such as bleeding gums, functional impotence of the lower limbs, and the petechiae on the upper and lower limbs. Other important elements for the diagnosis were the anamnestic data of low intake of vitamin C with the predominantly dairy-based diet and the X-ray of the lower limbs that allowed us to confirm our clinical suspicion by showing the typical radiographic signs of scurvy.
In fact, the literature has reported some specific radiological marks of vitamin C deficiency such as the “Fraenkel sign” (metaphysical calcification zone), the “Wimberger sign” (calcification around the epiphysis), the “Pelkan sign” (enlargement of metaphyses with protruding angles), the scurvy line (a shine adjacent to the metaphysical sclerotic line), and the separation of epiphyses and osteopenia [9,10]. Plasma levels of vitamin C <QL confirmed the diagnosis.
Normal levels of AGA, anti-transglutaminase antibodies, IgA, IgG, fecal occult blood,
Treatment in children consists of oral administration of ascorbic acid (100 mg) 3 times a day for 1 week, followed by 100 mg once a day until symptomatic resolution [4]. Once vitamin C deficiency has been treated, prevention and correction of underlying conditions are required to prevent recurrence [5,6,11].
Conclusions
In conclusion, our case shows that although the incidence of scurvy is significantly reduced in Western countries, the disease can still manifest and the early diagnosis is crucial, considering the excellent response to treatment.
Children with psychiatric disorders such as autism and anorexia and patients with gastrointestinal diseases with vomiting and/or malabsorption are at high risk of vitamin deficiency. Vitamin C deficiency is a possible consequence of low fresh fruit and vegetable intake and scurvy is a rare and serious complication [5].
In addition, we highlight the importance of a varied diet, especially in childhood, to ensure adequate growth and development. In this case report, vitamin C deficiency due to food selectivity and psychomotor delay were red flags that led to the diagnosis of an autism spectrum disorder. In this context, we want to reiterate the role of the family pediatrician, who must be able to identify the signs and symptoms of scurvy and to direct families to a specialist who can make a diagnosis for an early treatment and careful clinical and instrumental follow-up.
However, the real prevention consists in food education and an adequate nutritional intake for these patients in global health support. In fact, taking care of patients needs to utilize the appropriate resources, especially in complex diseases, who need a multi-specialistic approach [12].
Emergency pediatricians should broaden their differential diagnoses to nutritional deficiencies such as scurvy [13] in the evaluation of pediatric patients with limp, and include appropriate assessments in the differential diagnosis.
The goal of prevention in the field of autism spectrum disorder consists of early diagnosis leading to a timely educational program. This approach permits an improved long-term prognosis and allows the early detection of comorbidities that are sometimes found in children with autism. Significant progress has been made in this field; however, the pediatrician has an important role in starting the correct and timely diagnostic procedures in collaboration with child neuropsychiatrists [14].
References:
1.. Camarena V, Wang G, The epigenetic role of vitamin C in health and disease: Cell Mol LifeSci, 2016; 73(8); 1645-58
2.. Melina J, Saavedra MD, Scurvy due to restrictive diet in a child with autism spectrum disorder. Case report: Arch Argent Pediatr, 2018; 116(5); e684-87
3.. Bendicho S, Espachs A, Arántegui J, Martín O, Effect of high intensity pulsed electric fields and heat treatments on vitamins of milk: J Dairy Res, 2002; 69(1); 113-23
4.. Burhop J, Gibson J, de Boer J, Heydarian C, Do you C what I C: Emergency Department evaluation and diagnosis of pediatric scurvy in an autistic child with a restricted diet: Pediatr Emerg Car, 2020; 36(1); e1-e3
5.. Ma NS, Thompson C, Weston S, Brief report: Scurvy as a manifestation of food selectivity in children with autism: J Autism Dev Disord, 2016; 46(4); 1464-70
6.. Alqanatish JT, Alqahtani F, Alsewairi WM, Al-kenaizan S, Childhood scurvy: An unusual cause of refusal to walk in a child: Pediatr Rheumatol Online J, 2015; 13; 23
7.. Jacobsen A, DeNiro K, Rash and arthralgias in a teenager with autism: JAMA Pediatr, 2017; 171; 89-90
8.. Mayor S, Sixty seconds on scurvy: BMJ, 2016; 355; i65400
9.. Ceglie G, Macchiarulo G, Marchili MR, Scurvy: Still a threat in the well-fed first world?: Arch Dis Child, 2019; 104(4); 381-83
10.. Pan T, Hennrikus EF, Hennrikus WL, Modern day scurvy in pediatric orthopaedics: A forgotten illness: J Pediatr Orthop, 2021; 41(3); e279-84
11.. Luckow C, Thomas AA, Scurvy in a pediatric patient with autism and limp: A case report: J Emerg Med, 2021; 60(3); e53-56
12.. Kothari P, Tate A, Adewumi A, The risk for scurvy in children with neurodevelopmental disorders: Spec Care Dentist, 2020; 40(3); 251-59
13.. Ceglie G, Macchiarulo G, Marchili MR, Scurvy: Still a threat in the well-fed first world?: Arch Dis Child, 2019; 104(4); 381-83
14.. Posar A, Visconti P, Is it autism? Some suggestions for pediatricians: Turk Pediatri Ars, 2020; 55(3); 229-35
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133