25 April 2021: Articles 
Discontinuation of Hemodialysis After 8 Years in Favor of Toprak’s Kidney Care in a Patient with End-Stage Kidney Disease
Unusual clinical course, Unusual setting of medical care
Omer Toprak1ABCDEF*, Emel A. Bozyel2BDE, Burak Alp2BEF, Ali Kirik2ACDEDOI: 10.12659/AJCR.930857
Am J Case Rep 2021; 22:e930857






Abstract
BACKGROUND: End-stage kidney disease patients who need hemodialysis for more than 3 months are less likely to be able to discontinue dialysis. Patient care, however, can play a role in improving kidney function. In this study, we showed that even a patient on hemodialysis for 8 years can discontinue or reduce the number of weekly dialysis sessions through kidney care. Here, we report the effect of patient care on the ability to cease dialysis or reduce dialysis sessions, discuss such cessation or reduction in chronic hemodialysis patients, and describe proper follow-up procedure for a patient whose dialysis has been discontinued or reduced.
CASE REPORT: Here, we present a 77-year-old man who had undergone hemodialysis 3 times weekly for 75 months, after which dialysis sessions were gradually decreased and terminated within 21 months while undergoing Toprak’s Kidney Care, a kidney care program. The patient went without dialysis for 10 months. Then, hemodialysis was started once weekly for 46 months, as the glomerular filtration rate values decreased significantly. Following this period, he underwent hemodialysis 3 times weekly for 19 months. During these follow-up periods, 2 hospitalizations were required due to pneumonia and atrial fibrillation. There were no major adverse cardiac events. The patient is still in our follow-up care.
CONCLUSIONS: Gradual termination of an 8-year period of hemodialysis through a kidney care program without kidney transplantation is very rare. In end-stage kidney disease patients with adequate urination, kidney care should be considered to terminate hemodialysis or reduce the weekly dialysis sessions.
Keywords: Dialysis, Kidney Failure, Chronic, Nutrition Assessment, Patient Care, Atrial Fibrillation, Kidney, Kidney Transplantation, Renal Dialysis
Background
End-stage kidney disease (ESKD) patients who have been on dialysis for more than 3 months are unlikely to ever be able to completely cease dialysis [1]. Termination of dialysis is highly risky for ESKD patients, and can be fatal, especially due to pulmonary edema and hyperkalemia [2]. However, 1–8% of ESKD patients receiving long-term dialysis can recover kidney function and stop hemodialysis [3–6]. Renal function recovery (RFR) is defined as the termination of dialysis treatment after more than 3 months of dialysis and the recovery of adequate renal function [5,6]. Patient care may be considered in terms of preventing unnecessary dialysis, preserving residual kidney function, and RFR [7,8].
A limited number of publications have shown that RFR can occur and hemodialysis can be stopped by making dietary adjustments in hemodialysis patients [8]. The main components of Toprak’s Kidney Care are patient and caregiver training, lifestyle changes, nutrition and regular exercise, using the right drugs at the right doses, supporting morale and motivation, adjusting fluid balance, preserving residual kidney function, and alternative treatments [7].
Here, we present a case of discontinuation of hemodialysis after 8 years, without kidney transplantation, in a patient with ESKD. We also report follow-up of the patient without dialysis for 10 months, followed by dialysis only once a week for about 4 years, with Toprak’s Kidney Care. To the best of our knowledge, this is the first case in the literature in which the patient was able to discontinue hemodialysis after 8 years due to a renal care program.
Case Report
In October 2012, a 77-year-old man applied to our nephrology outpatient clinic. He had heard from other dialysis patients that some patients who have sufficient urination may be removed from chronic dialysis, or that the frequency of dialysis can be decreased. His medical history showed that he had bilateral nephrolithiasis for 20 years; hypertension for 9 years; an operation for benign prostate hypertrophy 20 years previously; double j catheter insertion in both kidneys 2 times, because of nephrolithiasis, 10 years ago; chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) because of recurrent renal colic; and intermittent antibiotic use for 20 years for recurrent pyelonephritis. He had been smoking half a pack of cigarettes per day for 30 years. He was diagnosed with ESKD secondary to chronic pyelonephritis in February 2005, and was followed up for 17 months in a pre-dialysis outpatient clinic. Renal biopsy could not be performed due to atrophic kidneys. An arteriovenous fistula was created in January 2006. Hemodialysis started in July 2006 due to hypervolemia and a glomerular filtration rate (GFR) of 5.8 ml/min/1.73 m2. He was treated with hemodialysis in an outpatient dialysis center for 75 months, 3 days per week, 4 hours per session. Preinitiation creatinine values were stabilized at 4–5 mg/dL during the 6 years of hemodialysis.
We hospitalized the patient for nephrological evaluation, and found an arteriovenous fistula with aneurysms in the left arm (Figure 1). This took place on a routine dialysis day. The patient was stable and had 800 cc/day of urine. Laboratory analysis revealed an estimated GFR of 11.1 ml/min/1.73 m2. On renal ultrasound, we found kidneys with bilateral small size and increased parenchymal echogenicity (Figure 2). We continued dialysis 3 times per week and started to change the patient’s medications, lifestyle, and nutritional habits according to Toprak’s Kidney Care (Tables 1, 2). We added calcium acetate, acetylsalicylic acid, carvedilol, and multivitamins, and stopped the intake of polystyrene sulfonate, unnecessary antibiotics, herbals, and NSAIDs. Salt intake and smoking were stopped. He was drinking 750 cc of water and 500 cc of other liquids during the periods when he was on dialysis. There was no fluid load. We allowed him to drink 1.5 liters of water and 500 cc of other liquids each day and stopped the diuretic. We also increased the dry weight from 76 kg to 77 kg. The patient and his wife attended our education seminars and training sessions. After 7 months, based on the patient’s laboratory and clinical findings, we reduced the dialysis sessions to twice per week, then to once per week. Finally, after 21 months of kidney care, the patient was removed from dialysis. When we decided to stop dialysis, the patient did not have uremic symptoms, acidosis, uncontrolled hypertension, hyponatremia, hyperphosphatemia, hyperkalemia, uremic encephalopathy, or fluid overload. Urine output increased. GFR levels stabilized at an average of 13 ml/min/1.73 m2 (Table 1). At the end of the 10-month dialysis-free period, we restarted dialysis once a week due to deterioration in renal function after pneumonia. He continued on dialysis once a week for 4 years. After a newly emerged atrial fibrillation, warfarin was started and dialysis sessions were increased to 3 times per week due to the accompanying hypervolemia. During our follow-up, 2 hospitalizations were required due to pneumonia and atrial fibrillation. There were no major adverse cardiac events. He is now 85 years old and continues dialysis 3 times a week, 4 hours per session.
Discussion
The novel findings of this case are that after a kidney care program, the hemodialysis sessions of an ESKD patient who had been on dialysis for many years were able to be reduced and even stopped. Residual renal function may be protected, even after 13 years of hemodialysis. Dialysis sessions can be reduced or terminated even if complete RFR is not detected. Even patients who have been on dialysis for many years and have received pre-dialysis training may have major dysfunctional lifestyle and dietary habits, and patients should be retrained in these areas.
Like the patient in our case, the expected remaining life of a patient over 75 years old in hemodialysis is approximately 3 years [9]. If this patient had not applied to us, and if he did not attend to his kidney care program, he would most likely still be on hemodialysis or perhaps he would have died. Under normal conditions, no one will attempt to reduce the number of hemodialysis sessions or terminate dialysis of a patient who has been on dialysis 3 times a week for 8 years, and who has had an arteriovenous fistula with aneurysmal dilatations and atrophic kidneys, as shown in Figures 1 and 2. In addition, no nephrologist would take such a risk and, moreover, most do not even think that such a possibility exists, because the patient’s diagnosis was not acute kidney injury (AKI). The diagnosis of the patient was ESKD requiring 8 years of hemodialysis. Of course, we cannot conclude with a single case report that all hemodialysis patients can discontinue dialysis with Toprak’s Kidney Care. We do not claim this. Although this is an important and rare presentation, prospective controlled studies with more patients are needed to generalize our observations. However, this case report is important as it shows that even after a very long dialysis period it is possible to discontinue dialysis or reduce dialysis sessions for years.
Renal replacement therapies create a huge burden on the economies of countries, and many patients can die because they cannot have kidney transplantation [2]. It is very important to be able to follow chronic kidney disease (CKD) patients with care programs [10,11]. Toprak’s Kidney Care is a care program available for CKD patients and their caregivers [7]. Most patients starting dialysis do not receive adequate kidney care before starting dialysis [10]. The present patient had been smoking, ingesting a high level of salt, not taking care to eat potassium-rich foods, and engaging in other suboptimal lifestyle practices, despite receiving pre-dialysis care for 17 months.
Our patient was diagnosed with dialysis-dependent ESKD. He had atrophic kidneys, permanent vascular access before dialysis, and was on pre-dialysis care for over 1 year. The possible causes of ESKD in this patient were multifactorial, including analgesic nephropathy or chronic interstitial nephritis due to NSAIDs or antibiotics, hypertensive nephropathy, chronic pyelonephritis due to recurrent urinary tract infections, or obstructive uropathies. Many patients with a diagnosis of CKD may develop acute renal failure, and this may lead patients to be misdiagnosed as ESKD, possibly resulting in patients becoming dialysis dependent [1,4]. Maybe our patient had AKI in addition to CKD and began dialysis at an early stage. When a patient is referred to a dialysis center, such a situation may be overlooked and the patient may be perceived as having ESKD. In our case, the estimated GFR value at the time of the start of the dialysis was 5.8 ml/min/1.73 m2 and this may be considered as ESKD. In addition, inaccurate measurement of ideal dry weight, unnecessary ultrafiltrations, unnecessary diuretic use, and fluid restrictions can further disrupt existing renal perfusion. In addition, unfortunately, progressive decreases in serum urea and creatinine values are perceived as inadequate nutritional status and, when accompanied by decreased muscle mass, patients may be subjected to more aggressive dialysis [6,7]. Probably, all of the situations mentioned above might be relevant for our patients.
Stopping long-term hemodialysis in end-stage renal disease would be lethal [6,7]. However, publications have reported that 0.3% to 8% of ESKD patients who receive long-term dialysis treatment may develop RFR, and dialysis may be terminated [3–6]. RFR rates are low in patients with permanent vascular access and who have received more than 1 year of care before starting dialysis [3,6]. The occurrence of RFR was unexpected for our patient because he had a fistula and had received more than 1 year of pre-dialysis care. Most patients with RFR have less than a year of dialysis-free time, and only 45% survive for 1 year after dialysis is discontinued [5,7]. Despite this, our patient did not undergo dialysis for more than 10 months, although complete RFR was not detected. After this, dialysis was performed only once a week for 4 years, and the patient is still alive today, with dialysis. If any undesirable effects or complications had developed in the patient after removing him from dialysis or reducing the dialysis sessions, we would be in a very difficult situation. Unfortunately, when we reduce the number of dialysis sessions of the patients or remove the patients from dialysis, sometimes we encounter objections and criticism from some foci. Just as there are conditions and medical guidelines for the initiation of hemodialysis, there should also be guidelines for termination and reduction of the dialysis sessions.
The topics of RFR and incremental dialysis have been described in the literature [3–8]. However, we could not find any case in which dialysis was discontinued after patient education or lifestyle changes. Only 1 study showed that continuing a low-protein diet can lead to cessation of dialysis in 3 CKD patients [8]. Hemodialysis duration before withdrawal from dialysis is less than 1 year in most RFR cases [3–5]. Data from 12 observational studies reveal that the median time to RFR and dialysis discontinuation is 8.3 months [6]. In a Swedish data registry, it was reported that 39 patients had RFR after 1 year of dialysis, and the longest duration before dialysis discontinuation was 5.7 years [5]. In the literature, there are very limited cases about discontinuation of hemodialysis secondary to RFR in ESKD patients after 8 years of dialysis. We found only 1 report: Letachowicz et al reported that the longest duration of hemodialysis before RFR and dialysis discontinuation was 97 months [4]. Our case is the second longest period of continuous dialysis reported in the literature before withdrawal from hemodialysis.
In our case we did not discontinue dialysis secondary to RFR, progressive decrease in urea and creatinine, or inability to tolerate dialysis. Most of the cases emerging from chronic hemo-dialysis have progressively decreasing urea and creatinine values and an inability to tolerate dialysis [3–6]. Despite the high creatinine levels, we enrolled the patient in our care program and decreased and then discontinued the dialysis sessions and observed an increase in kidney function. While the GFR value was initially 5.8 mL/min, it increased to 14.2 mL/min over the years, although the patient did not undergo dialysis, and the amount of daily urine increased from 700 mL to 1800 mL. Many factors, such as the patient’s condition, comorbid diseases, residual renal function, and intellectual capacity of both the patient and caregiver are some of the factors that determine the effect of Toprak’s Kidney Care on a patient.
There are many beneficial factors that may have led our patients to successfully discontinue dialysis. Diet, lifestyle changes, fluid regulation, regulation of medicines, and alternative treatments may all have contributed to cessation of dialysis. We added acetylsalicylic acid, carvedilol, and multivitamins, and stopped diuretics. Patients’ residual renal function usually decreases quickly under dialysis. However, there are certainly patients who maintain urine output for years while on dialysis, like our patient. In patients with residual renal function, there may be benefits associated with continuing diuretic use rather than automatically discontinuing diuretic therapy at dialysis initiation. However, many patients that may have had potential for RFR have been missed because of incorrect measurements of ideal dry weight, unnecessary fluid restriction, and excessive use of diuretics [12,13]. In our patient, we did not detect hypervolemia. Therefore, we increased fluid intake and stopped the diuretic he was taking. Using unnecessary diuretics can lead to pre-renal azotemia and a further decrease in renal perfusion. After increasing the patient’s oral fluid intake and ending ultrafiltration and hemodialysis, a significant increase was observed in our patient’s urine amount. In the 13th year of follow-up, we started the diuretic again when the patient developed hypervolemia (Table 1). CKD patients have a high risk of cardiovascular events. Low-dose aspirin is commonly used by elderly people for the prevention of thrombosis. The benefits and risks of antiplatelet therapy for patients with CKD remain controversial. In addition to providing cardiovascular protection, antiplatelet therapy is presumed to prevent dialysis vascular access thrombosis and improve fistula. Antiplatelet therapy might reduce the occurrence of major cardiovascular events and hemodialysis vascular access failure in CKD patients compared with placebo or usual-care groups [14]. For these reasons, we added acetylsalicylic acid to the patient’s treatment regimen. Carvedilol exerts an important reno-protective effect in CKD. Carvedilol may retard progression of albuminuria, provide cardiorenal protection in CKD patients with hypertension, and allow patients to retain residual kidney function [15]. Carvedilol has a pronounced vasodilating effect, which significantly reduces central arterial pressure; this is also an important renoprotective mechanism in the treatment of patients with renal dysfunction [16]. Therefore, after cardiology consultation, we started carvedilol in our patient. In adults with CKD, the prescription of folate, vitamin B12, and/ or B complex supplement is suggested, to correct for folate or vitamin B12 deficiencies [11]. In dialysis patients, additional intake of vitamin B6 reduces plasma cholesterol and triglyceride levels, and additional intake of folate can reduce high levels of homocysteine, which has been determined to be a risk factor for cardiovascular disease [17]. Therefore, we prescribed a multivitamin that contained vitamins B1, B6, B12, and folate.
We educated the patient and his wife through meetings and educational videos. We also used the educational television we prepared in the polyclinic: TV channels, social media, and educational videos to answer patients’ questions about diet and lifestyle. We curtailed salt intake and replaced it with kidney-friendly spices and herbs. Smoking was stopped and exercise duration was increased. We banned harmful drinks, processed meats, margarine, and white bakery products, and replaced them with kidney-friendly products. We reduced the amount of daily protein intake. We recommended taking sun baths. We gave spiritual support and treated depression and anxiety, both in the patient and his wife. We regulated the patient’s impaired sleep pattern by instituting the practice of siesta. All follow-up was done by the same nephrologist. Our patients can contact their nephrologist directly when they have any questions, 24 hours per day, 7 days per week.
The corresponding author of this study is experienced and trained in nutrition and spiritual care for CKD patients, and he has been working as the only nephrologist in the university hospital for 14 years, due to the lack of academic staff. In addition, the corresponding author has been following approximately 7000 pre-dialysis patients, for more than 14 years. This has provided us with great knowledge from experience in the follow-up of ESKD patients. All of this has led to the emergence of Toprak’s Kidney Care. We think that this experience can play a great role in terminating the dialysis of patients who have been receiving dialysis treatment for many years. We follow current guidelines in the care of CKD patients [11]. In addition, however, we have added alternative therapies gleaned from our 17 years of experience, such as zizyphus jujube, black seed oil, probiotics, pumpkin seeds, walking barefoot, and sweat therapy, all of which are beneficial in CKD. It has been reported that jujube fruits have beneficial effects for the prevention of hypertension, kidney damage, oxidative stress, and inflammation, and they also can help to decrease anxiety and depression [18,19]. We have also shown that jujube can aid in the control of dyslipidemia and diabetes in CKD patients [20]. As a part of Toprak’s Kidney Care, we prescribe tea, fruit, or vinegar of jujube to our CKD patients. Studies on black seed oil have established its nephroprotective role. In addition, black seed oil may improve renal functions in patients with CKD [21,22]. As a part of Toprak’s Kidney Care, we use black seed oil in our CKD patients. In CKD, concentrations of both urea and ammonium increase in the gastrointestinal tract, raising the pH level and promoting aerobic bacteria growth. High concentrations of these toxins have also been associated with progression of CKD. Regular consumption of probiotics has the potential to improve the quality of life in patients with CKD. Studies have indicated that consumption of probiotics may improve gastrointestinal function and slow the progression of CKD [23]. Therefore, as a part of Toprak’s Kidney Care, we prescribe probiotics such as homemade yogurt, apple or jujube vinegar, white sauerkraut, and kefir to our CKD patients. Pumpkin is a good source of vita-min C, B complex vitamins, omega-3 fatty acids, fiber, magnesium, zinc, and iron, which are all substances needed in ESKD patients. Pumpkin seeds help in the prevention and treatment of hypertension; these conditions were also present in our patient. Also, pumpkin seeds help to boost immunity and metabolism, uplift mood, and improve sleep [24]. Therefore, we prescribe pumpkin seeds to our CKD patients. When the connection to the earth is restored through grounding, electrons flood throughout the body and this may reduce inflammation and oxidative stress. Also, studies have shown that walking barefoot decreases pain, improves blood flow, reduces blood viscosity, reduces stress, improves energy, and improves response to trauma [25]. All of these contribute to a better quality of life for the patient. Therefore, we recommend walking barefoot as a part of Toprak’s Kidney Care. The skin is the largest organ in the human body, and has the potential to act like a third kidney [26]. After sweat treatment, especially in CKD patients, potassium, sodium, urea, toxins, and excess fluids that cannot be removed from the body by the kidneys can be excreted through sweating [27]. For this reason, we recommend sweat treatment to our CKD patients as part of Toprak’s Kidney Care. Since there are not enough studies in the literature about these alternative products and applications, we cannot recommend them for all CKD patients. We hope that once our large-scale studies are published, we will be able to talk more clearly about these alternative therapies.
The main limitation of this case report is its nature as only a single case; a larger study population is required to demonstrate the effectiveness of Toprak’s Kidney Care. Changes in lifestyle are very important but also difficult to introduce and to study objectively and quantitatively. The Chronic Kidney Disease Epidemiology Collaboration equation was used to measure the renal function of the patient in our study. We did not determine 24-hour urine creatinine clearance. Although baseline and follow-up creatinine clearance should be measured, in our case we used pretibial edema, urine amount, cardiothoracic ratio in X-ray, pleural effusion, and pericardial effusion for evaluation of the fluid status of the patient. However, it would be better to also use other echocardiogram findings, as well as plasma brain natriuretic peptide, to assess the body fluid status of the patient [28]. Also, there was no histological diagnosis of underlying kidney disease. The fact that the exact etiology of ESKD is unknown does not decrease the value of this case report, because what is important here is the follow-up of a patient diagnosed with ESKD who went without dialysis for nearly 1 year and who then survived with a reduced dialysis rate of once per week for nearly 4 years, even though he had undergone dialysis 3 times per week for 8 years. The strengths of this case report are that we demonstrated that a hemodialysis patient can maintain residual kidney function even after 13 years of dialysis. A dialysis patient may be removed from dialysis or the dialysis frequency may be decreased when combined with a program of kidney care. Such a patient may be able to discontinue dialysis despite decreased kidney function.
Conclusions
We should investigate the possibility of discontinuing dialysis or reducing the number of dialysis sessions, even after 8 years of hemodialysis, in patients with ESKD with sufficient urine. We should not forget that with careful monitoring and care, it is possible to discontinue dialysis in selected patients who have significant residual renal function. There is a risk of underdialysis and development of insidious uremic symptoms or complications in such cases after dialysis discontinuation. A consensus and clinical guidelines are needed regarding the termination or reduction of dialysis sessions in ESKD patients on chronic hemodialysis programs.
Figures
References:
1.. Chen Z, Lee BJ, McCulloch CE, The relation between dialysis-requiring acute kidney injury and recovery from end-stage renal disease: A national study: BMC Nephrol, 2019; 20; 342
2.. Bikbov B, Purcell CA, Levey AS, Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017: Lancet, 2020; 395; 709-33
3.. Mohan S, Huff E, Wish J, Fistula First Breakthrough Initiative Data Committee, 2013. Recovery of renal function among ESRD patients in the US medicare program: PLoS One, 2013; 8; e83447
4.. Letachowicz K, Madziarska K, Letachowicz W, The possibility of renal function recovery in chronic hemodialysis patients should not be overlooked: Single center experience: Hemodial Int, 2016; 20; 12-14
5.. Fehrman-Ekholm I, Bergenhag AC, Heimburger O, Recovery of renal function after one-year of dialysis treatment: case report and registry data: Int J Nephrol, 2010; 2010; 817836
6.. Chu JK, Folkert VW, Renal function recovery in chronic dialysis patients: Semin Dial, 2010; 23; 606-13
7.. Toprak O, Kirik A, Is renal function recovery and discontinuation of long term hemodialysis possible in patients with presumed end stage kidney disease? The role of Toprak’s Kidney Care: J Urol Ren Dis, 2020; 5; 1191
8.. Piccoli GB, Guzzo G, Vigotti FN, Tailoring dialysis and resuming low-protein diets may favor chronic dialysis discontinuation: report on three cases: Hemodial Int, 2014; 18; 590-95
9.. Seckinger J, Dschietzig W, Leimenstoll G, Morbidity, mortality and quality of life in the ageing haemodialysis population: results from the ELDERLY study: Clin Kidney J, 2016; 9; 839-48
10.. Awan AA, Zhao B, Anumudu SJ, Pre-ESKD nephrology care and employment at the start of dialysis: Kidney Int Rep, 2020; 5; 821-30
11.. Ikizler TA, Burrowes JD, Byham-Gray LD, KDOQI clinical practice guideline for nutrition in CKD: 2020 update: Am J Kidney Dis, 2020; 76(Suppl. 1); S1-S107
12.. Bragg-Gresham JL, Fissell RB, Mason NA, Diuretic use, residual renal function, and mortality among hemodialysis patients in the Dialysis Outcomes and Practice Pattern Study (DOPPS): Am J Kidney Dis, 2007; 49; 426-31
13.. Sibbel S, Walker AG, Colson C, Association of continuation of loop diuretics at hemodialysis initiation with clinical outcomes: Clin J Am Soc Nephrol, 2019; 14; 95-102
14.. Su X, Yan B, Wang L, Effect of antiplatelet therapy on cardiovascular and kidney outcomes in patients with chronic kidney disease: A systematic review and meta-analysis: BMC Nephrol, 2019; 20; 309
15.. Hart PD, Bakris GL, Should beta-blockers be used to control hypertension in people with chronic kidney disease?: Semin Nephrol, 2007; 27; 555-64
16.. Murkamilov IT, Sabirov IS, Fomin VV, Beta-blockers and renoprotection: The potential of carvedilol: Rational Pharmacother Cardiol, 2017; 13; 422-26
17.. Jankowska M, Szupryczyńska N, Dębska-Ślizień A, Dietary intake of vitamins in different options of treatment in chronic kidney disease: Is there a deficiency?: Transplant Proc, 2016; 48; 1427-30
18.. Lee D, Kang KB, Kim HW, Unique triterpenoid of jujube root protects cisplatin-induced damage in kidney epithelial LLC-PK1 cells via autophagy regulation: Nutrients, 2020; 12; 677
19.. Sobhani Z, Nikoofal-Sahlabadi S, Amiri MS: Med Chem, 2020; 16; 1069-88
20.. Toprak O, Sari Y, Keceli S; 265
21.. Ansari ZM, Nasiruddin M, Khan RA: Saudi J Kidney Dis Transpl, 2017; 28; 9-14
22.. Alam MA, Nasiruddin M, Haque SF: Saudi J Kidney Dis Transpl, 2020; 31; 21-31
23.. Nelson K, Wysocki J, Benefits of probiotic consumption on chronic kidney disease: J Ren Nutr, 2020; 30; e35-e36
24.. Dotto JM, Chacha JS, The potential of pumpkin seeds as a functional food ingredient: A review: Scientific African, 2020; 10; 575
25.. Menigoz W, Latz TT, Ely RA, Integrative and lifestyle medicine strategies should include Earthing (grounding): Review of research evidence and clinical observations: Explore (NY), 2020; 16; 152-60
26.. Ye T, Tu W, Xu G, Hot bath for the treatment of chronic renal failure: Ren Fail, 2014; 36; 126-30
27.. Keller RW, Bailey JL, Wang Y, Urea transporters and sweat response to uremia: Physiol Rep, 2016; 4; e12825
28.. Stenberg J, Melin J, Lindberg M, Brain natriuretic peptide reflects individual variation in hydration status in hemodialysis patients: Hemodial Int, 2019; 23; 402-13
Figures
Tables
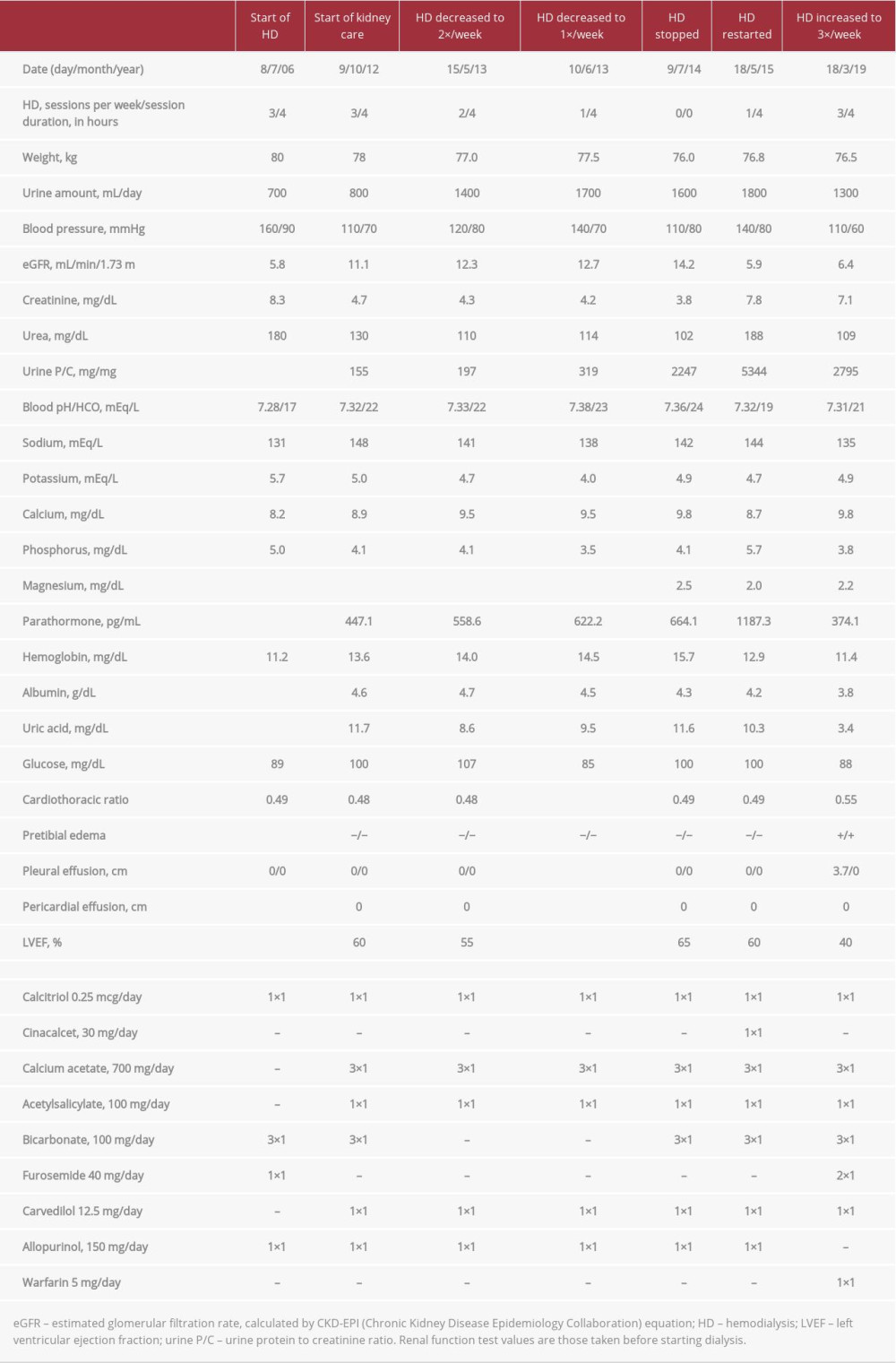 Table 1.. Renal, nutrition, and fluid load parameters and medications of the patient.
Table 1.. Renal, nutrition, and fluid load parameters and medications of the patient.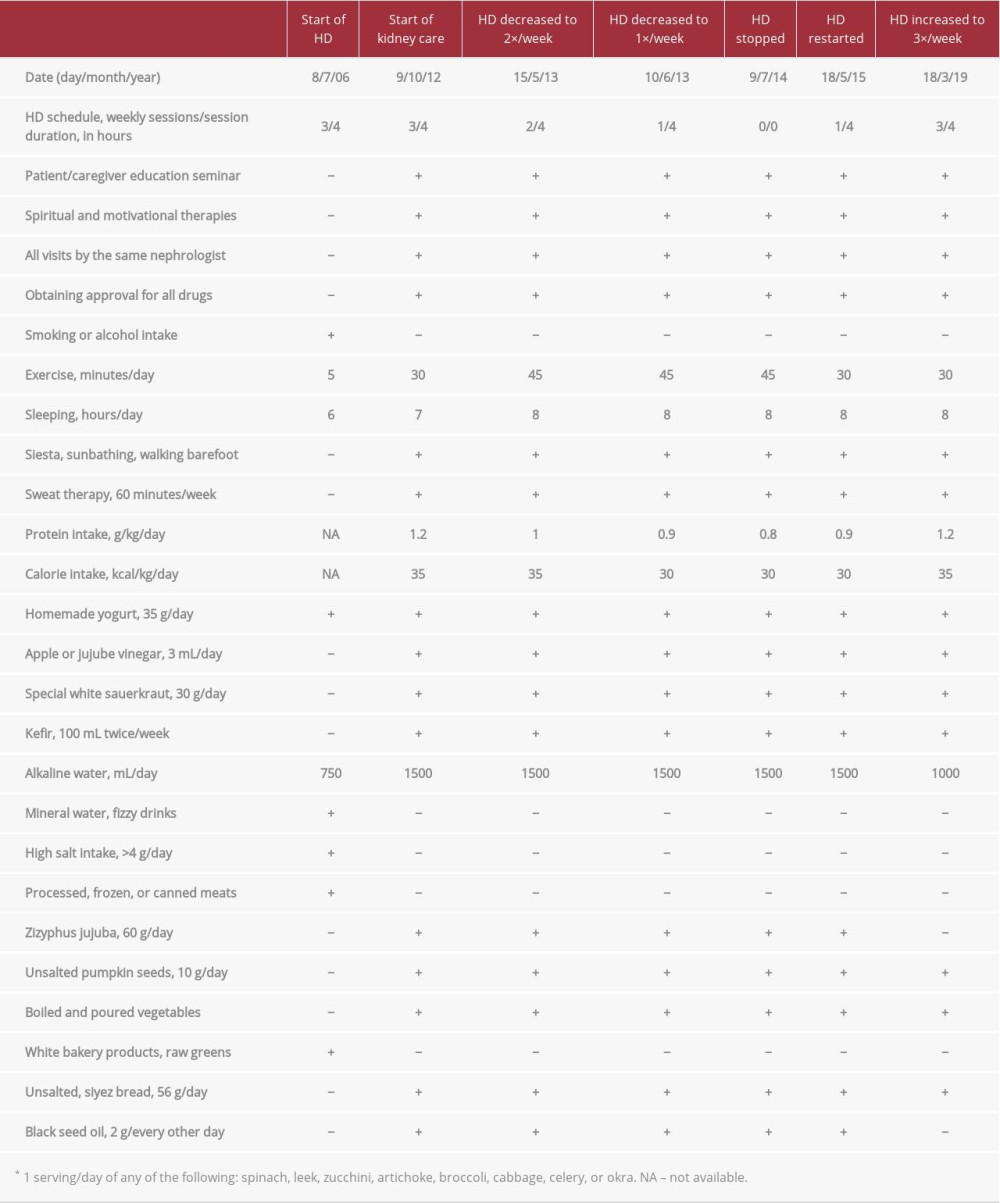 Table 2.. Educational activities, lifestyle changes, and important nutritional habits of the patient.Table 1.. Renal, nutrition, and fluid load parameters and medications of the patient.Table 2.. Educational activities, lifestyle changes, and important nutritional habits of the patient.
Table 2.. Educational activities, lifestyle changes, and important nutritional habits of the patient.Table 1.. Renal, nutrition, and fluid load parameters and medications of the patient.Table 2.. Educational activities, lifestyle changes, and important nutritional habits of the patient. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133