28 July 2021: Articles 
Total Splenectomy for a Giant Isolated Splenic Hydatid Cyst Compressing the Abdominal Viscera: A Case Report
Unusual or unexpected effect of treatment, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Dimitrios Chatzifotiou1ABDEF*, Christian Wolf1BEF, Arturs Baibakovs1BEF, Harald Werthebach2CD, Bogdan Lupascu1BEF, Martin Schnell1BEFDOI: 10.12659/AJCR.931195
Am J Case Rep 2021; 22:e931195






Abstract
BACKGROUND: Extrahepatic and extrapulmonary localizations of cystic echinococcosis (CE) are rare and the incidence of splenic involvement is seen in 1.0% to 3.3% of all cases in the endemic areas of the Middle East and Asia. The diagnostic pathway consists of a detailed travel history, physical examination, abdominal ultrasonography, computed tomography, and serological tests. The efficacy of perioperative administration of albendazole (400 mg twice a day) has been proven; however, the appropriate surgical procedure for the treatment of giant, centrally located splenic hydatid cysts remains controversial.
CASE REPORT: We present the case of a 49-year-old woman referred to our hospital for a suspected isolated splenic hydatid cyst causing a compression of the right kidney, stomach, and the tail of the pancreas. She reported chronic pain in the left upper quadrant and a history of contact with animals. She underwent open splenectomy via a medial to lateral approach to minimize manipulation of the spleen. In addition, she received perioperative parasitostatic drug therapy with albendazole. The postoperative period was uneventful and the histologic analysis confirmed the diagnosis.
CONCLUSIONS: The spleen is a rare location for isolated CE, especially in non-endemic areas and must be considered in the differential diagnosis of splenic cystic masses. Surgical resection remains the most effective treatment that completely resolves this condition. A comparison of randomized trials is needed to compare the recurrence rates between splenectomy and spleen-preserving procedures in the treatment of giant splenic hydatid cysts.
Keywords: Echinococcosis, Splenectomy, Splenomegaly, Spleen, Splenic Diseases, Viscera
Background
A hydatid cyst is the most common form of echinococcosis in humans. Although it presents as an endemic transmission in some areas of South America, Asia, and Africa, it is rare in European countries. The disease is mostly localized in the liver and lungs, although other organs can be affected due to systemic dissemination. An isolated spleen involvement is rare and presents only in 0.7% of the infected patients [1]. Large cysts can be symptomatic causing a compression of the adjacent abdominal organs. Cystic echinococcosis (CE) has a good prognosis in the majority of cases. The perioperative mortality rate is 0.8% and anaphylactic shock is the main cause of death [2]. This case report presents the rare case of an isolated splenic hydatid cyst, which should be considered in the differential diagnosis of cystic lesions of the left upper abdomen, especially in non-endemic regions.
Case Report
A 49-year-old Balkan woman living in a rural area presented to her general practitioner reporting 6 months of left upper quadrant pain without tenderness. Her past medical, pharmacological, and surgical history was unremarkable. On physical examination, a mass occupying the left upper abdomen was palpated. Ultrasonography revealed an uncertain cystic mass with solid components. Computed tomography (CT) of the abdomen and pelvis with an intravenous contrast showed a 22×18×13 cm septated splenic cyst with scattered calcifications and transient enhancement of the wall after contrast administration (Figure 1). The voluminous cyst had displaced the right kidney, stomach, and pancreas (Figure 2). No liver cysts were identified and the inflammatory markers were normal. On suspicion of CE, the patient was referred to our clinic. She mentioned contact with animals in her hometown. A CT scan of the lungs and a magnetic resonance imaging of the brain did not detect any additional lesions. The
Two weeks before the hospital admission, she was vaccinated against P
Discussion
CE due to
Hydatid disease can affect any organ, although the most common localization sites are the liver and the lungs. According to a systematic review, a splenic echinococcal involvement develops in 1% to 3.3% of the patients [4]. Other studies report this percentage to be between 2% and 5% [5,6]. However, most reported cases had concomitant hepatic hydatidosis, showing a systematic dissemination. According to a study from China, only 0.7% of 3003 patients with CE had an isolated splenic involvement [3]. There is no universally accepted size to define a hydatid cyst as ‘giant.’ A large hydatid cyst causing a significant enlargement of the affected organ or with exophytic growth through the natural routes provided by the organ capsule is defined as a giant hydatid cyst [7].
Diagnosis is based on clinical examination, imaging techniques, and serological tests. Hydatid cysts are mostly asymptomatic or can present with mild, dull, and non-specific abdominal pain, justifying the diagnostic delay [8]. The differential diagnosis incorporates other cystic formations of the spleen, including an epidermoid cyst, a pseudocyst, an abscess, a hematoma, and a cystic neoplasm of the spleen [9].
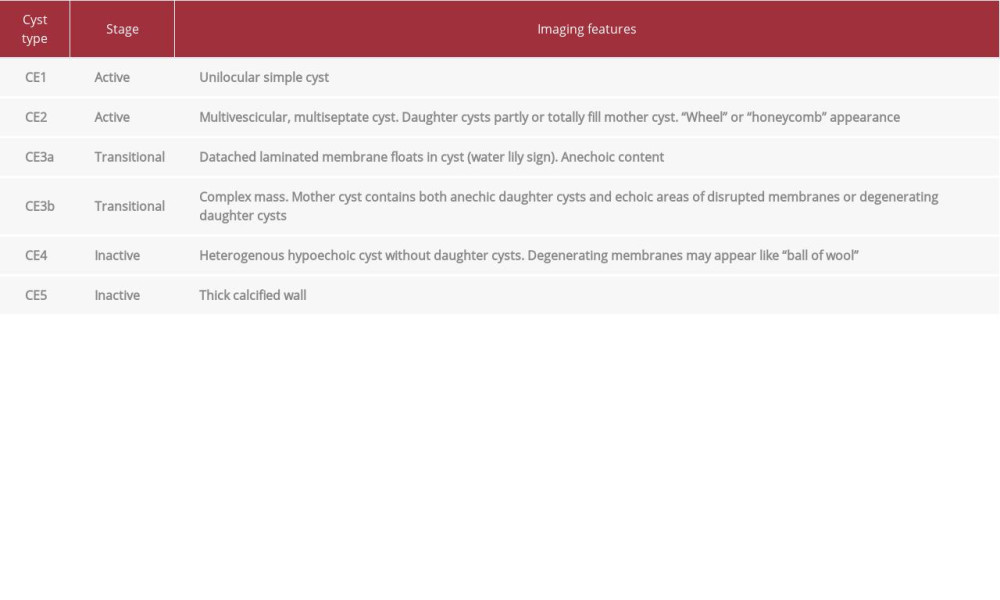
Ultrasonography is the diagnostic tool of choice for the detection of cystic lesions. Based on ultrasound imaging, the World Health Organization’s Informal Working Group for Echinococcosis (WHO-IWGE) has classified CE into 5 types. A CT is indicated for the subdiaphragmatic localizations of disseminated disease and presurgical evaluations [10]. The main radiological characteristics for hepatic and splenic hydatid cysts can vary from simple cysts to a solid appearance. However, solitary components are mainly found in splenic cysts [8,11]. Calcifications, a daughter cyst sign, hydatid membranes, and hydatid sand are other typical findings of the disease. In the present case, the CT revealed a type 4/5 CE hydatid cyst according to the WHO-IWGE classification (Table 1).
Serology has a complementary role in the primary diagnosis of the disease, although it is also useful for the follow-up. The ELISA tests have progressively replaced the tests with low sensitivity and specificity, including the Cassoni intradermal test, latex agglutination test, and indirect hemagglutination test. The enzyme-immunoassay system for the determination of IgG antibodies against
Surgical treatment is the main therapeutic option for patients with splenic hydatid cysts. The aim of the surgical procedure is cyst resection without intraoperative contamination of the abdominal cavity [10]. A percutaneous treatment with puncture, aspiration, injection of the protoscolicidal agent and reaspiration (PAIR), a watch and wait approach, or a long-term parasitostatic chemotherapy cannot be considered as alternative treatments for patients without any significant contraindications for surgery [10]. For patients with splenic hydatid cysts, a splenectomy is considered the treatment of choice providing a complete removal of the cyst with a low recurrence rate. On the other hand, it is associated with an overwhelming sepsis syndrome after the splenectomy. Thus, many authors suggested a spleen-preserving procedure for younger patients or in cases of peripherally located cysts, which occupy <50% to 75% of the parenchyma [3,16]. Spleen-preserving procedures can be a partial splenectomy, a partial cystectomy, or a cystotomy using flushing with 20% saline solution, and an omentoplasty [14]. Further studies with longer follow-ups are needed to estimate the recurrence rates in patients who undergo a partial cystectomy or cystotomy. In the present case, we performed an open splenectomy to avert a cyst perforation by manipulation of the specimen. A laparoscopic approach could be an optional procedure in patients with small cysts due to the low perforation risk. If a laparoscopic operation is performed, it is essential to adhere to the same technical standards that apply to corresponding open procedures. To the best of our knowledge, there are several case reports and case series in the bibliography, using various surgical procedures [17–21].
The surgical treatment must be combined with the perioperative administration of benzimidazole-carbamate compounds (BMZ). Among the BMZ compounds, ABZ and mebendazole are currently the only licensed drugs for the systemic treatment of echinococcosis [10]. ABZ has better bioavailability and is the preferred first-choice parasitostatic drug with a daily dose of 15 mg/kg divided in 2 doses [22]. The suggested duration of ABZ administration for patients after a radical and uncomplicated resection of the hydatid cyst is 4 weeks to 8 weeks [23]. The histological and cytological examinations are mandatory to confirm the presence of a parasitic cyst.
Conclusions
Although the spleen is a rare location for an isolated hydatid cyst, it should be included in the differential diagnosis of splenic cysts, especially in non-endemic countries. Despite the fact that surgery is the standard therapeutic option, there is no established consensus regarding the type of surgical procedure. We support the opinion of most surgeons that the main aim of the surgical procedure is complete resection of the hydatid cyst without any intraoperative peritoneal spillage. Therefore, we prefer a total splenectomy performed with a medial to lateral approach for giant hydatid cysts with a central localization in the parenchyma.
Figures
References:
1.. Ran B, Shao Y, Yimiti Y, Spleen-preserving surgery is effective for the treatment of spleen cystic echinococcosis: Int J Infect Dis, 2014; 29; 181-83
2.. El Malki HO, El Mejdoubi Y, Souadka A, Predictive factors of deep abdominal complications after operation for hydatid cyst of the liver: 15 years of experience with 672 patients: J Am Coll Surg, 2008; 206(4); 629-37
3.. , Robert-Koch-Institut Infektionsepidemiologisches Jahrbuch meldepflich-tiger Krankheiten für 2018 [cited 2019 March 1] [in German]https://www.rki.de/DE/Content/Infekt/Jahrbuch/Jahrbuch_2018.pdf?__blob=publicationFile
4.. Eckert J, Deplazes P, Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern: Clin Microbiol Rev, 2004; 17(1); 107-35
5.. Akcam AT, Ulku A, Koltas IS, Clinical characterization of unusual cystic echinococcosis in southern part of Turkey: Ann Saudi Med, 2014; 34(6); 508-16
6.. Mahmoudi S, Mamishi S, Banar M, Epidemiology of echinococcosis in Iran: A systematic review and meta-analysis: BMC Infect Dis, 2019; 19; 929
7.. Ettorre GM, Vennarecci G, Santoro R, Giant hydatid cyst of the liver with a retroperitoneal growth: A case report: J Med Case Rep, 2012; 6; 298
8.. Rasheed K, Zargar SA, Telwani AA, Hydatid cyst of spleen: A diagnostic challenge: N Am J Med Sci, 2013; 5(1); 10-20
9.. Franquet T, Montes M, Lecumberri FJ, Hydatid disease of the spleen: Imaging findings in nine patients: Am J Roentgenol, 1990; 154(3); 525-28
10.. Brunetti E, Kern P, Vuitton DA, Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans: Acta Trop, 2010; 114(1); 1-16
11.. Ilica AT, Kocaoglu M, Zeybek N: Am J Roentgenol, 2007; 189(2); 337-43
12.. Manzano-Román R, Sánchez-Ovejero C, Hernández-González A, Serological diagnosis and follow-up of human cystic echinococcosis: A new hope for the future?: Biomed Res Int, 2015; 2015; 428205
13.. Zhang W, Li J, McManus DP, Concepts in immunology and diagnosis of hydatid disease: Clin Microbiol Rev, 2003; 16(1); 18-36
14.. Wen H, Vuitton L, Tuxun T, Echinococcosis: Advances in the 21st Century: Clin Microbiol Rev, 2019; 32(2); e00075-18
15.. Pagnozzi D, Addis MF, Biosa G, Diagnostic accuracy of antigen 5-Based ELISAs for human cystic echinococcosis: PLoS Negl Trop Dis, 2016; 10(3); e0004585
16.. Ameur HB, Affes N, Abdelhedi C, Hydatid cyst of the spleen: Tunisian series of 21 cases: Indian J Surg, 2015; 77(Suppl.2); 515-19
17.. Ozogul B, Kisaoglu A, Atamanalp SS, Splenic hydatid cysts: 17 cases: Indian J Surg, 2015; 77(Suppl.2); 257-60
18.. Eris C, Akbulut S, Yildiz MK, Surgical approach to splenic hydatid cyst: Single center experience: Int Surg, 2013; 98(4); 346-53
19.. Singal R, Singh SK, Mittal A, A giant splenic hydatid cyst: Proc (Bayl Univ Med Cent), 2016; 29(1); 55-57
20.. Zhuoli Z, Yu Z, Liya X, Literature review: Am J Trop Med Hyg, 2019; 101(4); 821-27
21.. Pukar MM, Pukar SM, Giant solitary hydatid cyst of spleen – a case report: Int J Surg Case Rep, 2013; 4(4); 435-37
22.. Velasco-Tirado V, Alonso-Sardón M, Lopez-Bernus A, Medical treatment of cystic echinococcosis: systematic review and meta-analysis: BMC Infect Dis, 2018; 18(1); 306
23.. Arif SH, Ul-Bari S, Wani NA, Albendazole as an adjuvant to the standard surgical management of hydatid cyst liver: Int J Surg, 2008; 6(6); 448-51
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133