16 May 2021: Articles 
Hydralazine-Induced Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: Asymptomatic and Renal-Restricted Presentation
Challenging differential diagnosis, Unusual setting of medical care, Rare disease, Adverse events of drug therapy
Wan Tu1ABCDEFG*, Barry Fayman1ADE, Stephen C. Ward2BDE, Yusufal Mamoon1ABD, Sabiha S. Bandagi3CDDOI: 10.12659/AJCR.931263
Am J Case Rep 2021; 22:e931263






Abstract
BACKGROUND: Hydralazine, a potent vasodilator widely used to treat hypertension, has been implicated in an increasing number of cases of drug-induced autoimmune diseases in recent years. However, antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis secondary to hydralazine use has rarely been described and most reported cases involved multi-organ-related vasculitis, including skin and lung-kidney manifestations. ANCA-associated vasculitis is an immune-inflammatory condition characterized by necrotizing vasculitis with few or no immune deposits, predominantly affecting small vessels. The fact that the vasculitis is associated with hydralazine use and improves with discontinuation of hydralazine supports the diagnosis of hydralazine-induced disease. The case we report is a hydralazine-induced, ANCA-associated, pauci-immune crescentic glomerulonephritis with a presentation limited to the kidneys.
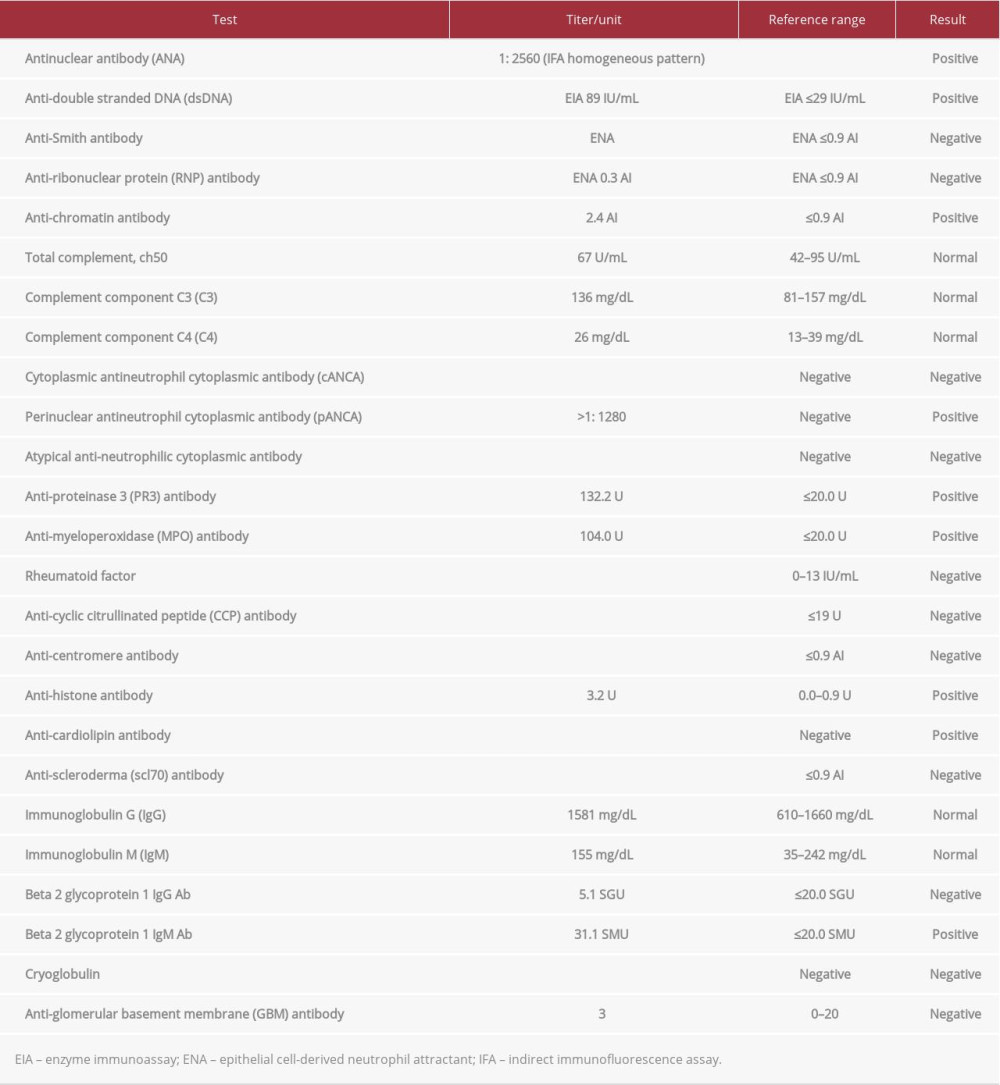
CASE REPORT: A 66-year-old woman was admitted to the hospital for worsening renal function over a month with no symptoms. Serology work-up was significantly positive for antinuclear, perinuclear ANCA, anti-histone, anti-double-stranded DNA, anti-cardiolipin, and anti-myeloperoxidase antibodies. The patient ultimately underwent a kidney biopsy, which revealed pauci-immune crescentic glomerulonephritis. Her kidney function improved with cessation of hydralazine as well as therapy with pulse steroids.
CONCLUSIONS: Hydralazine is commonly prescribed to treat hypertension. Healthcare providers should be aware of potentially severe hydralazine-induced ANCA-associated vasculitis, which can present with various clinical manifestations. Serologic studies have indicated that it has features that overlap with lupus. Biopsy is helpful for making a definitive diagnosis and developing individual treatment plans. Early diagnosis, cessation of the offending drug, and initiation of immunosuppressive therapy are key for favorable prognosis.
Keywords: Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis, Glomerulonephritis, Hydralazine, Antibodies, Antineutrophil Cytoplasmic, Kidney
Background
Hydralazine-induced antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a necrotizing vasculitis with few or no immune deposits that predominantly affects small vessels and it is associated with hydralazine use. The disease typically presents with multisystem involvement of organs such as the kidneys, lung, skin, mucosa, heart, blood, and joints; without prompt treatment, it can rapidly progress to organ failure [1]. The diagnosis mostly relies on serologic studies, with positivity for ANCA (anti-myeloperoxidase [MPO] and/or anti-proteinase 3 [PR3]) and tissue biopsy of involved organs showing pauci-immune vasculitis. Antinuclear (ANA), anti-his-tone, anti-double-stranded DNA (dsDNA), and anti-cardiolipin antibodies also can be positive and present with serologic features that overlap with systemic lupus erythematosus (SLE) [2]. However, only 3 studies have described the kidneys as the only organs involved in hydralazine-induced ANCA vasculitis [3–5]. Thus, the purpose of the present case report is to illustrate an asymptomatic and kidney-limited presentation of hydralazine-induced ANCA-associated vasculitis, which can be easily missed, and to highlight the work-up leading to the diagnosis and discuss a current evidence-based approach to this disease.
Case Report
:
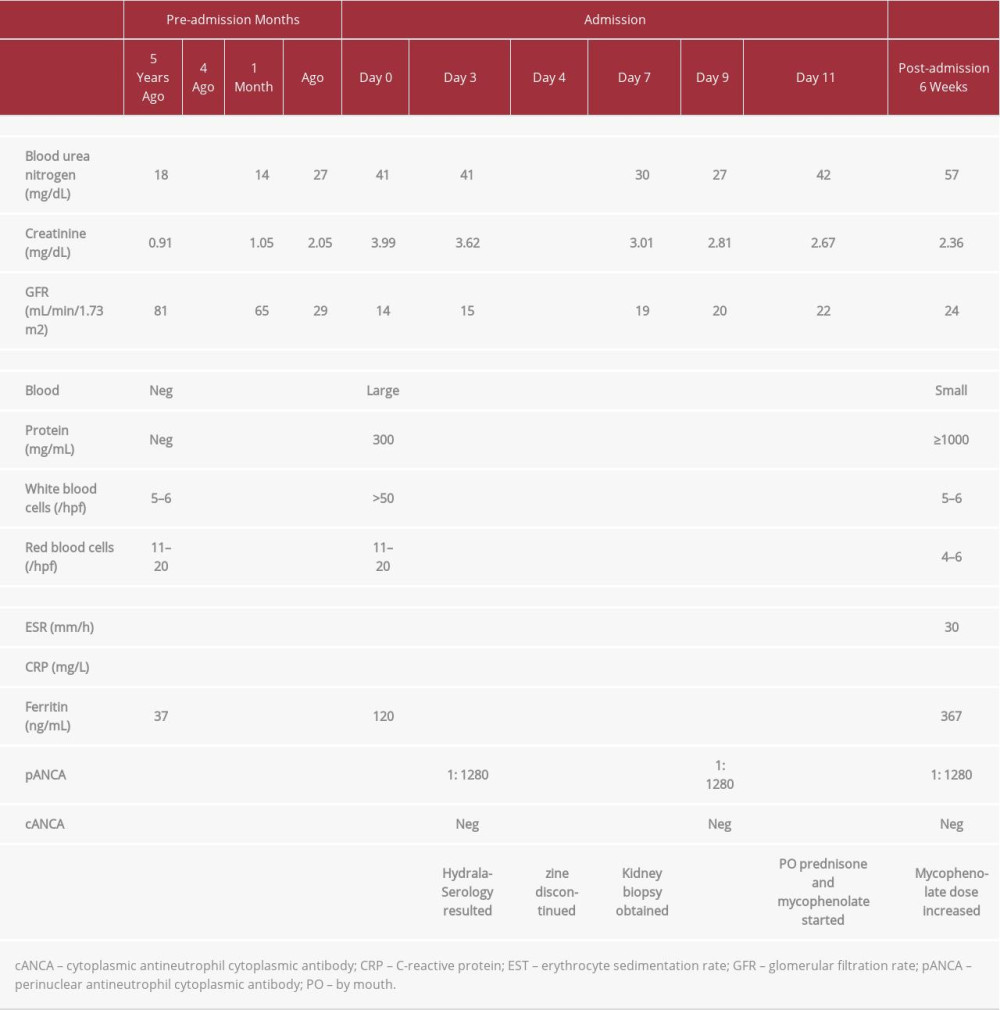
The patient was treated with gentle intravenous hydration, a transfusion of 1 unit of packed RBCs, 5 days of iron sucrose infusion after iron studies suggested that she had iron deficiency anemia, and sevelamer carbonate for hyperphosphatemia. Losartan and hydrochlorothiazide were stopped on the day of her admission and hydralazine was discontinued after the ANA and ANCA results were found to be positive.
Because of the presence of multiple positive autoimmune markers and the unclear etiology and prognosis of the patient’s kidney disease, a kidney biopsy was obtained and multiple cylindrical, pale tan soft tissue samples ranging in size from 0.1 cm to 1.7 cm in length and 0.1 cm in diameter were submitted. Light microscopy (Figure 1) indicated that of 23 glomeruli, 5 were obsolete, 9 contained cellular crescents, and 1 contained a fibrous crescent. There was some mild mesangial expansion and hypercellularity and a few glomeruli showed ischemic-type changes, but no endocapillary proliferation, wire loops, or hyaline thrombi were seen. There was also variable thickening of the tubular basement membranes, moderate arteriosclerosis, and moderate parenchymal scarring with associated lymphoplasmacytic infiltrates. Immunofluorescence studies showed only segmental immune deposits in an area of scarring and weak, nonspecific mesangial staining with immune globulin (Ig) M and lack of significant staining for IgG, IgA, complement component (C) 1q or C3 (Figure 2). Electron microscopy showed glomeruli with ischemic-type changes and variable thickening of the glomerular basement membranes but no immune-type deposits. The diagnosis of pauci-immune crescentic glomerulonephritis was made. The mesangial expansion and thickening of the glomerular and tubular basement membranes were compatible with early diabetic changes.
The patient’s kidney function started to improve 3 days after hydralazine was discontinued, as evidenced by a serum creatinine level of 3.01 mg/dL, BUN of 30 mg/dL, and eGFR of 19 mL/min/1.73 m2. After results of the kidney biopsy were received, the patient was started on methylprednisolone with pulsed dosing, 1000 mg daily for 3 days, and discharged home to take prednisone, 20 mg twice daily, and mycophenolate mofetil, 1000 mg daily. On the day of discharge, the patient’s kidney function had improved further to a creatinine level of 2.67 mg/dL, BUN of 42 mg/d, and an eGFR of 22 mL/min/1.73 m2.
The patient subsequently followed up with our nephrology and rheumatology clinics. She had continued to take prednisone, 20 mg twice daily and mycophenolate mofetil, 1000 mg daily, and remained asymptomatic. Laboratory testing performed 6 weeks after discharge showed an improved serum creatinine level of 2.36 mg/dL, BUN of 57 mg/dL, and eGFR of 24 mL/min/1.73 m2. Urinalysis showed a clear appearance, pH of 5.5, specific gravity of 1.016, 4 to 6 RBCs/hpf, 5 to 6 WBCs/hpf, >1000 mg/mL protein, no bacteria, and no casts.
Because the patient’s kidney function was not back to baseline and she had worsening proteinuria, her dosage of mycophenolate mofetil was increased to 1000 mg twice daily. She continues to follow up with our clinics.
Interventions at specific time points and outcomes are shown in Table 2.
Discussion
Drug-induced, ANCA-associated vasculitis is a group of immunoinflammatory conditions characterized by necrotizing vasculitis with few or no immune deposits, which predominantly affect small vessels and are associated with use of certain medications. The pathophysiology of the disease resembles microscopic polyangiitis because granulomatous inflammation is usually absent. The fact that the vasculitis is associated with use of specific drugs and improves with discontinuation of those agents supports the diagnosis of drug-induced disease.
Recently, more cases of drug-induced ANCA-associated vasculitis are being reported. The culprits include anti-thyroid drugs (propylthiouracil, methimazole, carbimazole, and benzylthiouracil), tumor necrosis factor inhibitors (etanercept, infliximab, adalimumab, and golimumab) and hydralazine, rituximab, minocycline, and montelukast. Other drugs that have been shown to have a possible association with ANCA-associated vasculitis include cefotaxime, nitrofurantoin, trimethoprim-sulfamethoxazole, vancomycin, isoniazid, rifampicin, D-penicillamine, sulfasalazine, clozapine, thioridazine, allopurinol, indomethacin, atorvastatin, cocaine/levamisole, denosumab, isotretinoin, and phenytoin [6]. Because of the low incidence of drug-induced ANCA-associated vasculitis and the beneficial use of the previously mentioned drugs, there is no recommendation to preclude the use of these medications. Because drug-induced vasculitis can cause rapidly deleterious disease, increasing awareness of it may lead to earlier diagnosis and prevent severe organ damage and death [7].
Hydralazine is one of the most common causes of drug-induced ANCA-associated vasculitis. A study performed by Kumar et al in 2018 [2] revealed that of 323 patients with ANCA-associated vasculitis, 12 were exposed to hydralazine, with the average duration of hydralazine therapy being 22 months and a mean cumulative dose of 146 g. In these patients, the serologic features overlapped with SLE, as all 12 were found to be positive for ANA (titers 1: 160 to 1: 2560; 10 diffuse pattern and 2 nucleolar), ANCA (titers 1: 320 to 1: 2560; 11 perinuclear ANCA pattern, 1 cytoplasmic ANCA), and anti-histone. Eleven of the 12 patients also were positive for anti-MPO and anti-double stranded DNA (anti-dsDNA), 4 had positive anti-cardiolipin IgG or IgM, and 9 had hypocomplementemia. All 6 patients who underwent kidney biopsy had pauci-immune crescentic glomerulonephritis. A literature review performed by Battisha et al in 2020 [8] showed that of 35 patients with lung-kidney syndrome secondary to hydralazine-induced, ANCA-associated vasculitis, 29 of 33 had positive ANA, 33 of 34 had positive anti-MPO, 6 of 19 had positive anti-PR3, 20 of 21 had positive anti-histone, and 12 of 30 had positive anti-dsDNA antibodies; 9 of 22 had low C3 and C4; none of 13 had anti-GBS antibodies; and 25 of 33 survived.
In our case, because the patient had no symptoms and only her kidneys were involved, it was challenging to reach the final diagnosis. There were 4 possible differentials: hydrazaline-induced lupus (HIL), idiopathic ANCA-associated vasculitis, SLE, and diabetic nephropathy or monoclonal Ig deposition disease.
HIL usually occurs after use of medication for >3 years in patients who are positive for ANA and anti-histone antibodies, and sometimes positive for anti-MPO antibodies [9]. However, HIL usually presents with systemic symptoms and sometimes arthritis (80% to 95%), kidney involvement is uncommon (<5%), and testing for anti-dsDNA antibodies usually is negative [9]. Unlike HIL, hydralazine-induced ANCA vasculitis is frequently associated with kidney involvement with a pauci-immune glomerulonephritis and high titers of anti-MPO [10]. In our case, high-titer anti-MPO (>4 times the normal value) was reassuring about the true-positive ANCA. Even though HIL can present with positive ANCA, the presence of pauci-immune glomerulonephritis instead of immune complex deposits on kidney biopsy helped us to make a definitive diagnosis. While lupus nephritis usually presents with immune complex deposits when kidney function is severely impaired (class III, IV, V, and VI), biopsy would show an immunofluorescence profile with staining for IgG, IgA, C3, and C1q. However, the renal biopsy in our patient only showed weak, nonspecific IgM. Active lupus nephritis would also be expected to show endocapillary proliferation and wire loops and/or hyaline thrombi, which were mentioned as pertinent negatives in our patient’s kidney biopsy.
Anti-histone, anti-dsDNA, and anti-cardiolipin antibodies usually are absent in idiopathic disease. Cessation of hydralazine significantly improved our patient’s kidney function, which makes drug-induced vasculitis a more probable diagnosis.
SLE typically progresses gradually. Patients with it are usually younger and almost always have other organ involvement, leukopenia and thrombocytopenia with anemia, low levels of C3 and C4, and are negative for anti-histone and ANCA antibodies but positive for anti-dsDNA and anti-Smith antibodies. In addition, in patients with SLE, kidney biopsy should reveal the classic findings of lupus nephritis described previously.
In our patient, the thickening of the glomerular and tubular basement membranes and the mesangial expansion/hyper-cellularity shown in the kidney biopsy were likely secondary to diabetes, but these relatively early diabetic features would not account for the rapid renal dysfunction or crescents. Her relatively well-controlled hemoglobin A1C over the past 5 years and normal serum immunofixation study excluded these diagnoses.
A PubMed search on January 10, 2021 using the search terms “hydralazine” and “ANCA vasculitis” retrieved records for only 50 published cases of hydralazine-induced, ANCA-associated vasculitis. Therefore, hydralazine-induced ANCA vasculitis is a very uncommon condition. The diagnosis mostly relies on serologic studies that are positive for ANCA (anti-MPO and/ or anti-PR3) and tissue biopsy of involved organs that shows pauci-immune vasculitis. Some patients may test positive for anti-histone, anti-dsDNA, and anti-cardiolipin antibodies. It has been observed that patients with hydralazine-induced vasculitis typically have a more severe course than those with hydralazine-induced SLE, predominantly due to more kidney involvement with vasculitis; thus, they require more aggressive treatment [11]. The clinical manifestations of hydralazine-induced, ANCA-associated vasculitis depend on the organ involved and include dyspnea, cough, sinusitis, hemoptysis, paroxysmal nocturnal dyspnea, orthopnea, fatigue, general weakness, edema, fever, dizziness, altered mental status, near syncope, weight loss, decreased appetite, vomiting, hypertension, dysuria, hematuria, skin rash or eruption, hemorrhagic blisters, vesiculobullous lesions, pruritus, arthralgia, myalgia, sore throat, mouth ulcer, otalgia, and hepato-splenomegaly, with the complications of kidney failure, anemia, leukopenia, pancytopenia, alveolar hemorrhage, lung-kidney syndrome, pericarditis, and cutaneous vasculitis.
Kidney involvement is common in hydralazine-induced vasculitis. According to the 50 cases in our literature search, 16 of the patients had kidney biopsies, all of which showed pauci-immune glomerulonephritis. Light microscopy indicated crescent glomerulonephritis in 15 of the patients, combined segmental necrotizing lesions in 8 of them, and acute tubular injury or necrosis in 5 of those patients. Immunofluorescence studies showed mesangial hypercellularity in 5 of the patients.
So far, however, only 3 studies have reported hydralazine-induced vasculitis limited to the kidneys [3–5]. Only 1 study has reported on an asymptomatic patient with hydralazine-induced vasculitis [4]. The case we reported is of an asymptomatic patient with a negative prior urine microalbumin level, who was found to have hydralazine-induced, ANCA-associated, pauci-immune crescentic glomerulonephritis with a presentation limited to the kidneys. The findings in our patient highlight the need for increased awareness on the part of healthcare providers who are using hydralazine to treat hypertension, especially in patients who are asymptomatic and have worsening kidney function.
Withdrawal of the offending agent is always the primary intervention for hydralazine- or drug-induced ANCA vasculitis and initiation of immunosuppressive therapy is also considered the hallmark of management. Treatment should be individualized to the patient, based on age, disease severity, comorbidities, and kidney function on presentation [12]. Steroids were used in all the cases documented in the literature, as well as other immunosuppressants. Commonly used immunosuppressive therapy includes azathioprine, cyclophosphamide, mycophenolate mofetil, and rituximab [8,12,13]. Plasmapheresis also was used on some patients. Hemodialysis is often applied when there is progression to end-stage kidney disease or if severe hyperkalemia develops [3]. However, progression of kidney disease can still vary, and it sometimes results in poor outcomes despite medical therapy [14]. One study showed remission and relapse of kidney failure despite proper medical management [4]. Nonetheless, it remains crucial to have a high index of suspicion to diagnose and treat hydralazine-induced vasculitis promptly [14].
Conclusions
Hydralazine is widely prescribed during medical encounters. Hydralazine-induced, ANCA-associated vasculitis is still considered a rare disease, and as such, it can be misdiagnosed or neglected during medical practice. The clinical manifestations are varied. Patients can even be asymptomatic with pauci-immune crescentic glomerulonephritis as a kidney-limited presentation, as illustrated by the present case report. The diagnosis is challenging. Biopsy is helpful for making a definitive diagnosis, and especially for differentiating between drug-induced SLE and vasculitis. Early diagnosis, cessation of the offending drug, and initiation of immunosuppressive therapy are key to a favorable prognosis.
References:
1.. Babar F, Posner JN, Obah EA, Hydralazine-induced pauci-immune glomerulonephritis: Intriguing case series with misleading diagnoses: J Community Hosp Intern Med Perspect, 2016; 6(2); 30632
2.. Kumar B, Strouse J, Swee M, Hydralazine-associated vasculitis: Overlapping features of drug-induced lupus and vasculitis: Semin Arthritis Rheum, 2018; 48(2); 283-87
3.. Zuckerman R, Patel M, Costanzo EJ, Hydralazine associated adverse event: A report of two cases of hydralazine induced ANCA vasculitis: J Bras Nefrol, 2018; 40(2); 193-97
4.. Shida H, Hashimoto N, Kusunoki Y, Anti-neutrophil extracellular trap antibody in a patient with relapse of anti-neutrophil cytoplasmic antibody-associated vasculitis: A case report: BMC Nephrol, 2018; 19(1); 145
5.. Baloch NU, Ibeabuchi AN, Hydralazine-induced MPO-ANCA renal-limited vasculitis masquerading as lupus nephritis: J Coll Physicians Surg Pak, 2018; 28(11); 896-97
6.. Weng CH, Liu ZC, Drug-induced anti-neutrophil cytoplasmic antibody-associated vasculitis: Chinese Med J, 2019; 132(23); 2848-55
7.. Grau RG, Drug-induced vasculitis: New insights and a changing lineup of suspects: Curr Rheumatol Rep, 2015; 17(12); 71
8.. Battisha A, Doughem K, Sheikh O, Hydralazine-induced ANCA associated vasculitis (AAV) presenting with pulmonary-renal syndrome (PRS): A case report with literature review: Curr Cardiol Rev, 2020 [Online ahead of print]
9.. Vaglio A, Grayson PC, Fenaroli P, Drug-induced lupus: Traditional and new concepts: Autoimmun Rev, 2018; 17(9); 912-18
10.. Choi HK, Merkel PA, Walker AM, Drug-associated antineutrophil cytoplasmic antibody-positive vasculitis: Prevalence among patients with high titers of antimyeloperoxidase antibodies: Arthritis Rheum, 2000; 43(2); 405-13
11.. Yokogawa N, Vivino FB, Hydralazine-induced autoimmune disease: Comparison to idiopathic lupus and ANCA-positive vasculitis: Mod Rheumatol, 2009; 19(3); 338-47
12.. Aeddula NR, Pathireddy S, Ansari A, Hydralazine-associated antineutrophil cytoplasmic antibody vasculitis with pulmonary-renal syndrome: BMJ Case Rep, 2018; 2018; bcr2018227161
13.. Paley MA, Edrees F, Kudose S, Successful use of rituximab for hydralazine-induced anti-neutrophil cytoplasmic antibodies-associated vasculitis: Saudi J Kidney Dis Transpl, 2019; 30(1); 226-30
14.. Timlin H, Liebowitz JE, Jaggi K, Outcomes of hydralazine induced renal vasculitis: Eur J Rheumatol, 2018; 5(1); 5-8
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133