17 July 2021: Articles 
Probiotic Supplementation Improved Acute Anterior Uveitis of 3-Year Duration: A Case Report
Unusual setting of medical care
Pasquale Napolitano1ABCDEF*, Mariaelena Filippelli1CDEF, Luca D'andrea1F, Marianna Carosielli1F, Roberto dell'Omo1DF, Ciro Costagliola1ACDEDOI: 10.12659/AJCR.931321
Am J Case Rep 2021; 22:e931321






Abstract
BACKGROUND: Uveitis is a clinical condition characterized by acute blurry vision related to an inflammation of the uvea. Gut microbiome dysbiosis can influence the prognosis of uveitis by inducing a loss of intestinal immune homeostasis leading to a lower activation threshold of the immune cells. This promotes a pro-inflammatory response resulting in reactivation of the disease. This is the case report of a 21-year-old woman with a 3-year history of acute anterior uveitis (AAU) of the right eye, who responded favorably to probiotic dietary supplementation.
CASE REPORT: A 21-year-old woman, previously unknown to our Ophthalmology Unit, presented with ocular pain and redness. Three years ago, she had been diagnosed with monolateral AAU in the right eye. Her medical and family histories were unremarkable. After a complete clinical evaluation, we decided to start a combination treatment protocol with continuous use of probiotics and the use of ocular steroids only during an exacerbation of the condition. To monitor the trend of the disease, she underwent a monthly clinical examination for the following year. During this period, we observed a decrease in ocular inflammation with a gain in the primary outcome (best-corrected visual acuity), and the steroids and atropine were discontinued for the following months.
CONCLUSIONS: This case report describes a patient with a 3-year history of AAU, who responded well to a combination treatment of dietary probiotic supplementation and steroids, demonstrating that probiotics can reduce recurrences of AAU.
Keywords: Probiotics, Uveitis, Anterior, Recurrence, uveitis, young adult
Background
Uveitis is a clinical condition characterized by acute blurry vision related to an inflammation of the uvea. The classification of uveitis is based on its anatomical location, etiology, and prognosis [1,2]. The prevalence of uveitis is approximately 5/1000 patients in the United States, with a direct correlation with smoking and age [3]. Idiopathic uveitis and auto-immune uveitis are more common, whereas infectious uveitis represents a small percentage of cases (approximately 17%). Acute anterior uveitis (AAU) is seen in approximately 85% of cases. This is related to a specific leukocyte cell-surface antigen called HLA-B27 [4].
Gut dysbiosis can influence the prognosis of uveitis by inducing a loss of the gut’s immune homeostasis, resulting in an easier activation of immunity, thus promoting inflammation and reactivating the disease. Several hypotheses link the gut micro-biome and ocular disease, including the loss of immune homeostasis, which allows the presentation of bacterial products and the activation of immune cells in remote sites, the loss of local intestinal immune balance, molecular mimicry, and the relative loss of tolerance toward ocular antigens. Usually, ocular antigens are not presented to the immune cells, as they are protected behind the blood-ocular barrier [5]. At the molecular level, epigenetic modifications coordinate gene transcription regulation. Therefore, it is crucial to identify the factors that trigger epigenetic changes leading to altered cellular function [6]. In a rat model of uveitis, the upregulation of micro-ribonucleic acid 223 (miRNA-223) was found to promote Th1/Th17 cytokines, including interferon (IFN)-g and interleukin (IL)-17 [7]. These authors linked the increased serum levels of miRNA-223 to microbiome dysbiosis. A case-control serum comparison of miRNA profiles highlighted the presence of uveitis-associated miRNA clusters. This evidence suggested a strong association between gut microbiota and ocular uveitis. This is the case report of a woman with a 3-year history of anterior uveitis who responded favorably to treatment with dietary probiotic supplementation and steroids.
Case Report
A 21-year-old woman previously unknown to our Ophthalmology Unit presented in our Outpatient Clinic with ocular redness and pain. When she was 18 years old, she had ocular pain, redness, and reduced visual acuity and was diagnosed with monolateral AAU in her right eye. During the 3 years before our clinical assessment, she had >3 annual uveitis recurrences treated with steroids (oral prednisone 25 mg, 2% topical betamethasone eye drops, and a peribulbar injection of 20 mg triamcinolone acetonide). She had no remarkable family or medical history. At our clinical examination, her best-corrected visual acuity (BCVA) (evaluated using the Monoyer chart) [8] was 3/10 in her right eye (sphere −1.25=cylinder −1 axis 180°) with normal ocular motility and color vision. The slit lamp examination showed 3+ cellular proteins in the Tyndall effect, defined as proteins present inside the anterior chamber. In these cases, the slit lamp light can reflect in multiple directions, leading to the scattering of light [9]. Mutton-fat keratic precipitates and iris Koeppe and Busacca nodules were observed. The iris had persistent posterior synechia. Her intraocular pressure (IOP) was 25 mmHg and a posterior subcapsular cataract was recorded. The fundus examination revealed the presence of a pink optic disc, normal fovea, and normal retinal vessels. Vitreal flow, which is a sign of spillover cells from the anterior chamber determining vitreal inflammation, was detected. Optical coherence tomography (OCT) performed with spectral domain OCT (SD-OCT) (Heidelberg Engineering, Heidelberg, Germany) [10] showed normal macular thickness (mean macular thickness [MMT] 230 μm, normal range 212±20 μm) with no retinal pigment epithelium (RPE) dystrophy, and an inflammatory cell flow in the vitreous.
The clinical examination of the fellow eye showed a BCVA of 10/10 (sphere −1.75=cylinder −1.25 axis 180°), normal color vision, and ocular motility. The slit lamp examination showed no cellular proteins in the Tyndall effect, an absence of mutton-fat keratic precipitates, and no iris nodules. A clear lens and an IOP of 15 mmHg were noted. The fundus examination showed a pink optic disc, normal fovea, and normal retinal vessels. No signs of vitreal inflammation were observed. The OCT showed normal macular thickness (MMT 242 μm, normal range 212±20 μm) with no RPE dystrophy or inflammatory cell flow in the vitreous. After our clinical evaluation, we made a diagnosis of AAU.
We decided to treat her with a combination treatment of topical steroids (standard treatment) and probiotic supplementation. We added a probiotic cocktail (to be taken every day for 1 year) to the standard topical treatment protocol (1% dexamethasone phosphate 4 times daily and 1% atropine 2 times daily). Therefore, a single dose of ≥1×109 live cells of
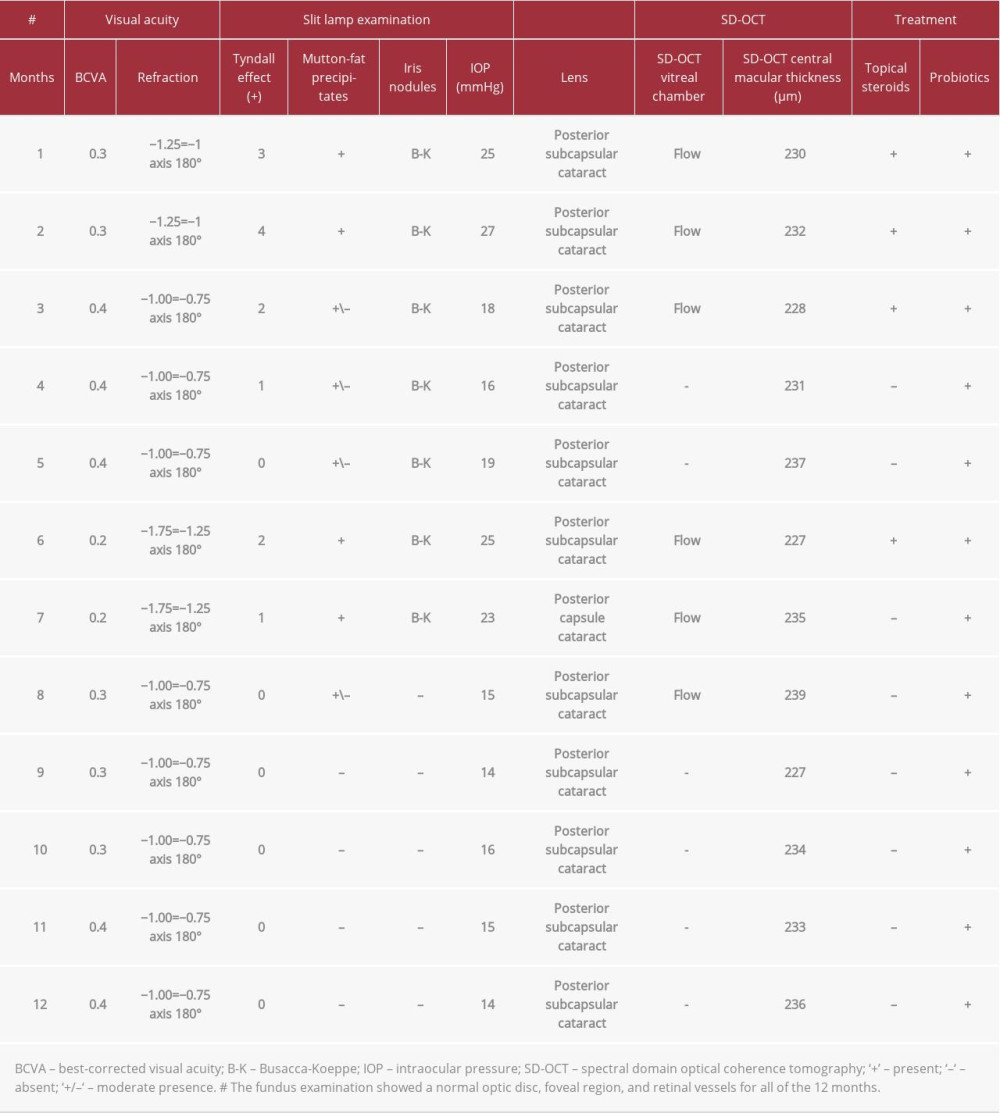
A clinical examination was performed every month for a year (Table 1). After month 1 of the combined treatment (topical 1% dexamethasone phosphate 4 times daily and 1% atropine 2 times daily, and probiotic mixture), the active uveitis was persistent. Nevertheless, the BCVA was stable at 3/10 (sphere −1.25=cylinder −1.0 axis 180°) with evidence of mutton-fat keratic precipitates. The Tyndall effect revealed 4+ cellular proteins with ocular hypertension (27 mmHg) and inflammation. We decided to continue the combined treatment for another month (month 2) and there was an improvement in the BCVA to 4/10 (sphere −1.0=cylinder −0.75 axis 180°) associated with a decrease in the proteins seen in the Tyndall effect, and a decrease in the mutton-fat deposits. The IOP was 18 mmHg and the ocular inflammation had decreased. Therefore, we decided to modify the therapy by administering only the probiotic preparation for the next few months (month 3 to month 6). The evaluated parameters improved until the 6th month, when the uveitis recurred (Figure 1). The BCVA was 2/10 (sphere −1.75=cylinder −1.25 axis 180°), the IOP was 25 mmHg, and the Tyndall effect showed 2+ cellular proteins. Therefore, we decided to prescribe the same combined treatment (topical steroids, atropine, and probiotics) again for 1 month (month 7). A decrease in ocular inflammation with a gain in BCVA was recorded, and steroids and atropine were discontinued for the following 5 months (month 8 to month 12). At the last checkup (12 months), she showed a BCVA of 3/10 in the right eye (sphere −1.25=cylinder −1.0 axis 180°), normal color vision, and ocular motility. A slit lamp examination identified a reduction of cellular proteins in the Tyndall effect (Figure 2A 2B,) and mutton-fat keratic precipitates (Figure 3A, 3B). The iris presented with persistent posterior synechia. The IOP was 14 mmHg and a posterior subcapsular cataract had developed before our combination treatment due to the high doses of previously administered steroids. The fundus examination showed a pink optic disc, normal fovea, and normal retinal vessels. We observed a normal vitreal cavity without vitreous flows. The OCT examination showed normal macular thickness with no RPE dystrophy and no flow in the vitreous.
During the follow-up period performed each month for the following 12 months (month 13 to month 24), she did not have any adverse events related to the administration of the probiotics and no changes occurred in the fellow eye. The BCVA remained stable at 10/10 (sphere −1.75=cylinder −1.25 axis 180°). We did not observe any signs of ocular inflammation or development of AAU in the left eye. The IOP remained stable (14±5 mmHg), the lens was clear, and no fundus alteration was observed. The OCT (Figure 4A, 4B) showed normal macular thickness with no RPE dystrophy. She currently takes the pro-biotic mixture 4 times a year (2 months on and 1 month off).
All the procedures performed in this case report were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The patient provided written informed consent for publication of this case report.
Discussion
This case report suggests that a probiotic cocktail supplementation reduces the number of recurrences of AAU in patients. The possible explanation could be a lower activation of cellular immunity (regulatory T cells/IL-17), which stops the signal of the inflammatory cascade that is the first step toward uveal inflammation. It has been suggested that epigenetic changes promote the development of the disease in a mouse model. Tbx21 and Rorc are the master transcription factors for the differentiation of helper and regulatory T cells [11,12]including T regulatory cells (Treg cells. The retinal hypomethylation of deoxyribonucleic acid factors was highlighted in the RPE-choroidal tissues of mice with experimental anterior uveitis and related to the production of IFNg and IL-17 [7]. The up-regulation of miRNA-223 triggered inflammation through the T cells and myeloid dendritic cells. The altered serum levels of miRNA-223 were related to microbiome dysbiosis, and a case-control serum comparison of miRNA profiles highlighted the presence of uveitis-associated miRNA clusters. Verhagen et al identified a group of 6 miRNAs related to the inflammatory signaling cascades, including the transcription factors mitogen-activated protein kinase, forkhead box, and vascular endothelial growth factor [13]environmental, and-relatively unexplored-epi-genetic factors. MicroRNAs (miRNAs. An integrated therapeutic approach is essential to obtain good clinical results to protect patient sight. Our study is in agreement with the findings of Askari et al [14], who demonstrated that dietary supplementation with probiotics improved the ocular symptoms in a patient with anterior uveitis in Behcet’s syndrome.
This is a period of great scientific ferment for microbiota research in ophthalmology. The role of the gut microbiome in human disease is beginning to emerge. Recent literature [14] supports our approach and contributes to improving the course of inflammatory diseases, including uveitis. These studies confirmed the presence of a gut-eye axis and a link between the gut microbiota alteration and ocular disease. Understanding the microbiome profiles associated with disease states can further our understanding of the variations in disease phenotypes and responses to treatment. This opens the way for a better understanding of the gut-eye axis and ways it can contribute to a good prognosis of uveitis. The mechanisms of these associations have recently become clearer. However, a number of critical barriers still exist and further studies are needed to prove the role of the gut microbiome in ocular disease, which could lead to developments in alternative or adjunctive local or systemic therapies to modulate the ocular surface and gut microbiota.
Conclusions
This is the case report of a patient with a 3-year history of anterior uveitis treated with a combination of steroids and dietary probiotic supplementation, suggesting that probiotics are able to reduce the number of recurrences of the disease. Combined therapy can relieve the signs and symptoms of AAU and create a new complementary therapy for its treatment, possibly by suppressing the systemic inflammation.
Figures
References:
1.. Forrester JV, Kuffova L, Dick AD, Autoimmunity, autoinflammation, and infection in uveitis: Am J Ophthalmol, 2018; 189; 77-85
2.. Sng CCA, Ang M, Barton K, Uveitis and glaucoma: New insights in the pathogenesis and treatment: Prog Brain Res, 2015; 221; 243-69
3.. González MM, Solano MM, Porco TC, Epidemiology of uveitis in a US population-based study: J Ophthalmic Inflamm Infect, 2018; 8(1); 6
4.. Huang X, Ye Z, Cao Q, Gut microbiota composition and fecal metabolic phenotype in patients with acute anterior uveitis: Investig Ophthalmol Vis Sci, 2018; 59(3); 1523-31
5.. Horai R, Caspi RR, Microbiome and autoimmune uveitis: Front Immunol, 2019; 10; 232
6.. Wen X, Hu X, Miao L, Epigenetics, microbiota, and intraocular inflammation: New paradigms of immune regulation in the eye: Prog Retin Eye Res, 2018; 64; 84-95
7.. Qiu Y, Zhu Y, Yu H, Dynamic DNA methylation changes of Tbx21 and Rorc during experimental autoimmune uveitis in mice: Mediators Inflamm, 2018; 2018; 9129163
8.. Moutakis K, Hall-Lindberg J, Using the KM visual acuity chart for more reliable evaluation of amblyopia compared to the HVOT method: Acta Ophthalmol Scand, 2004; 82(5); 547-51
9.. Agrawal R, Keane PA, Singh J, Comparative analysis of anterior chamber flare grading between clinicians with different levels of experience and semi-automated laser flare photometry comparative analysis of anterior chamber flare grading between clinicians with different levels of experience and semi-automated laser flare photometry: Ocul Immunol Inflamm, 2016; 24(2); 184-93
10.. Yalçındağ FN, Temel E, Şekkeli MZ, Kar İ, Macular structural changes and factors affecting final visual acuity in patients with Behçet uveitis: Graefes Arch Clin Exp Ophthalmol, 2021; 259(3); 715-21
11.. Fang D, Zhu J, Dynamic balance between master transcription factors determines the fates and functions of CD4 T cell and innate lymphoid cell subsets: J Exp Med, 2017; 214(7); 1861-76
12.. Lazarevic V, Chen X, Shim JH, T-bet represses TH 17 differentiation by preventing Runx1-mediated activation of the gene encoding RORgt: Nat Immunol, 2011; 12(1); 96-104
13.. Verhagen FH, Bekker CPJ, Rossato M, A disease-associated microRNA cluster links inflammatory pathways and an altered composition of leukocyte subsets to noninfectious uveitis: Investig Ophthalmol Vis Sci, 2018; 59(2); 878-88
14.. Askari G, Moravejolahkami AR, Synbiotic supplementation may relieve anterior uveitis, an ocular manifestation in Behcet’s syndrome: Am J Case Rep, 2019; 20; 548-50
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133