02 August 2021: Articles 
Acquired Thrombotic Thrombocytopenic Purpura Without Anti-ADAMTS13 Antibody Caused by Influenza A (H1N1) Virus Successfully Treated by Plasma Exchange: A Case Report
Challenging differential diagnosis, Diagnostic / therapeutic accidents, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Keisuke Kubo1ABDEF*, Tomohiro AbeDOI: 10.12659/AJCR.932251
Am J Case Rep 2021; 22:e932251






Abstract
BACKGROUND: Thrombotic microangiopathy, characterized by microangiopathic hemolytic anemia, thrombocytopenia, and organ damage by microvascular thrombosis, has a high mortality rate; therefore, early diagnosis and treatment are important. Thrombotic thrombocytopenic purpura is caused by a deficiency of a disintegrin-like and metalloproteinase with thrombospondin type 1 motifs 13 (ADAMTS13), and results in thrombotic microangiopathy. Influenza virus causes thrombotic thrombocytopenic purpura by inducing immunoglobulin G autoantibodies against ADAMTS13. We report a rare case of thrombotic thrombocytopenic purpura caused by influenza A without anti-ADAMTS13 antibody that was treated by plasma exchange.
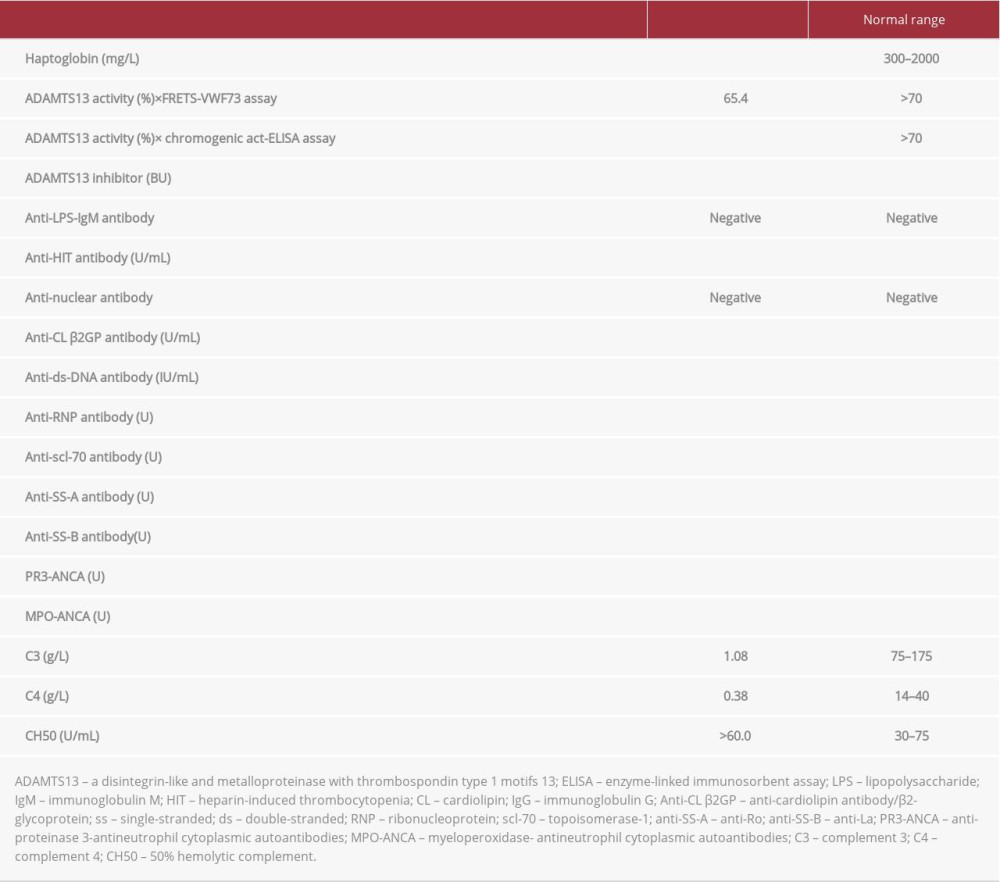
CASE REPORT: A 57-year-old woman was admitted to our hospital because of hypoxemia. We diagnosed pneumonia and disseminated intravascular coagulation. Despite treatment, she developed thrombocytopenia, and we diagnosed thrombotic microangiopathy and started plasma exchange. With a PLASMIC score of 6 points and neuropsychiatric symptoms, we strongly suspected thrombotic thrombocytopenic purpura and started rituximab. However, ADAMTS13 activity by FRETS-VWF73 assay was 65%, and anti-ADAMTS13 antibody was negative. After 4 plasma exchanges and 2 rounds of rituximab, platelet numbers and lactate dehydrogenase and creatinine concentrations normalized on the 16th day of hospitalization. Subsequently, influenza A (H1N1) was identified in a nasopharyngeal swab collected on admission. Plasma enzyme-linked immunosorbent assay testing for chromogenic ADAMTS13 activity showed a significant decrease (<0.5%). Therefore, we diagnosed thrombotic thrombocytopenic purpura caused by influenza A without anti-ADAMTS13 antibody.
CONCLUSIONS: We present a rare case of thrombotic thrombocytopenic purpura without anti-ADAMTS13 antibody caused by influenza A virus successfully treated by plasma exchange. Influenza A may reduce ADAMTS13 activity without inducing autoantibodies.
Keywords: Influenza A virus, Plasma Exchange, Purpura, Thrombotic Thrombocytopenic, Thrombotic Microangiopathies, Influenza A Virus, H1N1 Subtype, Influenza, Human
Background
Thrombotic microangiopathy (TMA) is a syndrome characterized by microangiopathic hemolytic anemia (MAHA), thrombocytopenia, and organ damage owing to microvascular thrombosis. TMA is classified as hemolytic uremic syndrome (HUS), thrombotic thrombocytopenic purpura (TTP), atypical hemolytic uremic syndrome (aHUS), and secondary TMA [1]. TMA has a rapid progression of symptoms and a high mortality rate, and even in surviving patients, organ damage is common; therefore, early diagnosis and emergency treatment, including plasma exchange, are important [2,3].
TTP is caused by a congenital or acquired deficiency of a disintegrin-like and metalloproteinase with thrombospondin type 1 motifs 13 (ADAMTS13), a von Willebrand factor-cleaving enzyme, which prevents cleavage of the ultra-large von Willebrand factor multimer (UL-VWFM), resulting in platelet aggregation, platelet thrombus formation, and TMA. The diagnosis of TTP is based on a marked decrease in ADAMTS13 activity (<10%). TTP treatment involves plasma therapy, such as with fresh frozen plasma infusion and plasma exchange [4–6].
TTP is classified into 2 forms: congenital (familial) and acquired TTP. Acquired TTP is caused by the production of immunoglobulin (Ig) G-type autoantibodies against ADAMTS13, which is called immune-mediated TTP (iTTP), while congenital
TTP (Upshaw-Schulman syndrome; USS) is caused by a congenital deficiency of ADAMTS13; acquired TTP is the most common form (>95%) [4–6]. Anti-ADAMTS13 antibody is the key finding in the diagnosis of acquired TTP.
Influenza virus causes TTP by inducing IgG autoantibodies against ADAMTS13, resulting in decreased ADAMTS13 activity [7]. We report a rare case of TTP caused by influenza A (H1N1) without anti-ADAMTS13 antibody that was treated by plasma exchange.
Case Report
The patient was a 57-year-old woman with an unremarkable medical history. She developed upper respiratory symptoms and visited a nearby hospital 1 week later. She had a dry cough, general malaise, and a fever of 39°C, which made it difficult for her to move. On the same day, the patient was admitted to our hospital for further investigation and treatment of hypoxemia.
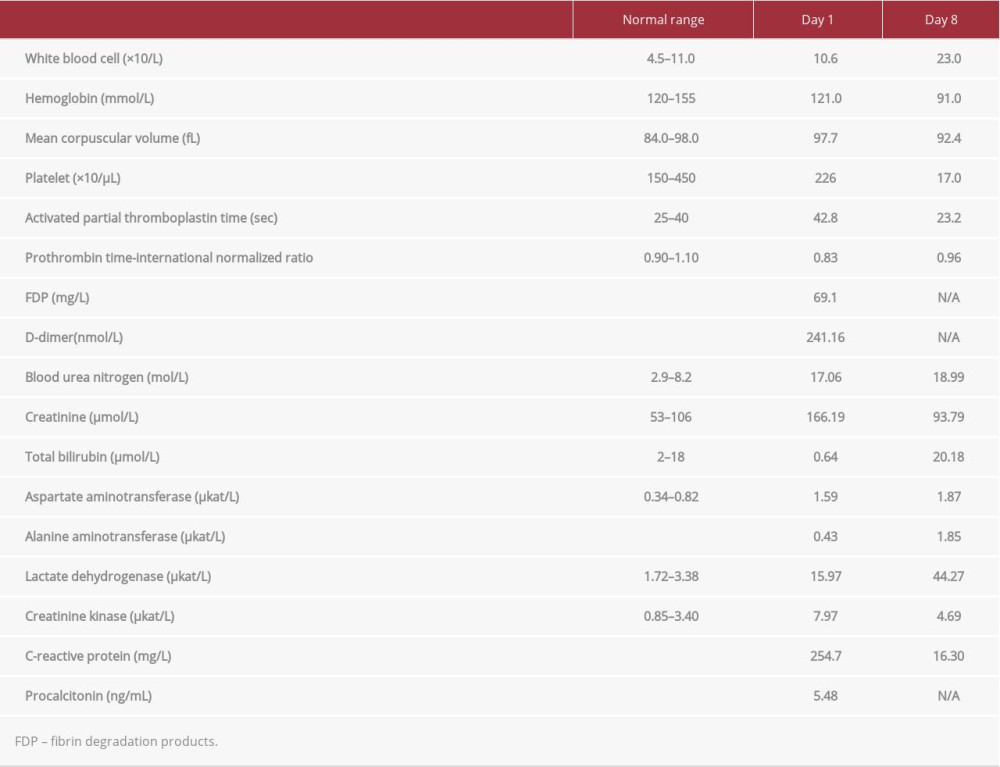
On admission, the patient’s vital signs were as follows: body temperature: 36.7°C, blood pressure: 105/77 mmHg, pulse: 90/min, respiratory rate: 24/min, oxygen saturation (SpO2): 76% (while receiving O2 at 15 L/min), Glasgow coma scale (GCS) score: E3 V4 M6. No jugular venous distension was seen, wet rales were auscultated in the chest during full inspiration, and peripheral cyanosis was present. Blood laboratory testing (Table 1) showed an increased inflammatory response; renal dysfunction; aspartate aminotransferase (AST), lactate dehydrogenase (LDH), and creatinine kinase (CK) elevation; and coagulation abnormalities. Urinary pneumococcal antigen and
We diagnosed respiratory failure owing to pneumonia of unknown cause and disseminated intravascular coagulation (DIC). Considering bacterial pneumonia, atypical pneumonia, acute exacerbation of interstitial pneumonia, and influenza pneumonia as factors contributing to respiratory failure, we started ceftriaxone 2 g/day, levofloxacin 500 mg/day, steroid pulse therapy (methylprednisolone 1 g/day for 3 days), and peramivir 600 mg. Recombinant human thrombomodulin 380 U/kg was used to treat the DIC.
On the third day of hospitalization, the patient’s platelet count decreased to 37.0×103/μL, and platelet transfusion was performed; however, the platelet count remained low. On the 8th day, we diagnosed the patient with TMA due to the presence of fragmented erythrocytes in the blood smear, thrombocytopenia, elevated LDH concentration, and renal dysfunction (Table 1), and we initiated plasma exchange. The stool culture and serum antibody levels for enterohemorrhagic
We performed 4 plasma exchanges at 50 mL/kg/day and administered rituximab at 375 mg/m2 once a week for 2 weeks. On the 16th day, platelet numbers returned to the normal range, and LDH and creatinine concentrations normalized. Antimicrobial therapy was terminated on the 7th day. After pulse therapy, the corticosteroid was tapered over 2 weeks because almost all autoantibodies, including anti-ADAMTS13 antibody, were negative. During the course of treatment, the patient developed a rectal ulcer and pulmonary embolism, which improved with treatment; she was discharged to home on the 41st day. Three months after discharge, the patient had not relapsed; Figure 2 shows her progress during hospitalization.
Subsequently, we submitted the nasopharyngeal sample collected on admission to the National Institute of Public Health and the Environment, which identified influenza A virus (H1N1) infection. Plasma was collected at the same time as the samples submitted for the FRETS-VWF73 assay, for enzyme-linked immunosorbent assay (ELISA) testing for chromogenic ADAMTS13 activity, to the Department of Blood Transfusion Medicine, Nara Medical University, which identified a significant decrease (<0.5%). We therefore diagnosed the patient as having TTP caused by influenza A without anti-ADAMTS13 antibody. After plasma exchange and without immunosuppressive therapy, the ADAMTS13 activity 2 weeks after initial treatment was 25.5% and the patient did not have relapse of TTP.
Discussion
This was a case of TMA of unknown cause that was successfully treated with plasma exchange. Initially, ADAMTS13 activity was not significantly decreased and autoantibodies were negative, but later, ADAMTS13 activity was markedly decreased. The cause of the TMA was influenza A (H1N1).
The present case is considered anti-ADAMTS13 autoantibody-negative acquired TTP. Because the patient experienced no relapse, and the ADAMTS13 activity increased without immunosuppressive therapy, the possible pathogenesis of TTP is non-immune-mediated TTP. We administered recombinant soluble thrombomodulin to treat the DIC. Although soluble thrombomodulin inhibits ADAMTS activity in vitro [8], it did not cause the acquired TTP in the present case because the FRETS-VWF73 showed normal ADAMTS13 activity. Therefore, influenza A virus (H1N1) may inhibit ADAMTS13 without inducing autoantibodies.
ADAMTS13 activity tested by the FRETS-VWF73 assay was not significantly decreased, while its activity tested by the chromogenic ADAMTS13-act-ELISA assay showed a marked reduction. The possible reasons why these 2 methods showed significantly different results may be differences in the substrate between these assays. Because the FRETS-VWF73 assay showed sufficient ADAMTS13 activity in this case, the ADAMTS13 cleavage site of the FRETS-VWF73 substrate may be overexposed compared to that of the human von Willebrand factor. The ADAMTS13 cleavage site of von Willebrand factor may become hidden upon the binding of GST and His tags to VWF73, because the clinical course clearly matched the results of the chromogenic ADAMTS13-act-ELISA assay. Comparisons of the sensitivity of these 2 assays have been heterogeneous [9,10]; thus, similar TTP cases may have been inaccurately undiag-nosed by the FRETS-VWF73 assay.
Our patient showed signs of DIC. The findings in patients with TMA are similar to those in patients with DIC, namely thrombocytopenia and organ damage. Patients with TMA require early diagnosis and treatment because of the rapid progression, high mortality rate, and high incidence of organ damage, even in surviving patients, while patients with DIC are mainly treated by treating the underlying disease. TMA is not associated with coagulopathy, generally. As reported by Wada et al [11] and previous reports of TTP owing to influenza [12–15], TMA and DIC can be associated. It is important to diagnose TMA even in the presence of coagulopathy.
Definitive differentiation between TTP, HUS related to Shigatoxin-secreting
Conclusions
We present a rare case of TTP without anti-ADAMTS13 antibody caused by influenza A virus (H1N1) successfully treated by plasma exchange. Influenza A may reduce ADAMTS13 activity without inducing autoantibodies. Once TMA is diagnosed, plasma exchange should be started as soon as possible because the immediate differentiation of the causes of TMA is difficult. Efforts to differentiate the underlying causes should be made to determine subsequent treatments.
Figures
References:
1.. George JN, Nester CM, Syndromes of thrombotic microangiopathy: N Engl J Med, 2014; 371; 654-66
2.. Azoulay E, Bauer PR, Mariotte E, Expert statement on the ICU man-agement of patients with thrombotic thrombocytopenic purpura [published correction appears in Intensive Care Med. 2020;46(3): 570–71]: Intensive Care Med, 2019; 45; 1518-39
3.. Azoulay E, Knoebl P, Garnacho-Montero J, Expert statements on the standard of care in critically ill adult patients with atypical hemolytic uremic syndrome: Chest, 2017; 152; 424-34
4.. Zheng XL, Vesely SK, Cataland SR, ISTH guidelines for treatment of thrombotic thrombocytopenic purpura: J Thromb Haemost, 2020; 18; 2496-502
5.. Scully M, Hunt BJ, Benjamin S, Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies: Br J Haematol, 2012; 158; 323-35
6.. Matsumoto M, Fujimura Y, Wada H, Diagnostic and treatment guidelines for thrombotic thrombocytopenic purpura (TTP) 2017 in Japan: Int J Hematol, 2017; 106; 3-15
7.. Bitzan M, Zieg J, Influenza-associated thrombotic microangiopathies: Pediatr Nephrol, 2018; 33; 2009-25
8.. Crawley JT, Lam JK, Rance JB, Proteolytic inactivation of ADAMTS13 by thrombin and plasmin: Blood, 2005; 105; 1085-93 3
9.. Joly B, Stepanian A, Hajage D, Evaluation of a chromogenic commercial assay using VWF-73 peptide for ADAMTS13 activity measurement: Thromb Res, 2014; 134; 1074-80
10.. Valsecchi C, Mirabet M, Mancini I, Evaluation of a new, rapid, fully automated assay for the measurement of ADAMTS13 activity: Thromb Haemost, 2019; 119; 1767-72
11.. Wada H, Matsumoto T, Suzuki K, Differences and similarities between disseminated intravascular coagulation and thrombotic microangiopathy: Thromb J, 2018; 16; 14
12.. Koh YR, Hwang SH, Chang CL, Thrombotic thrombocytopenic purpura triggered by influenza A virus subtype H1N1 infection: Transfus Apher Sci, 2012; 46; 25-28
13.. Jonsson MK, Hammenfors D, Oppegaard O, A 35-year-old woman with influenza A-associated thrombotic thrombocytopenic purpura: Blood Coagul Fibrinolysis, 2015; 26; 469-72
14.. Kosugi N, Tsurutani Y, Isonishi A, Influenza A infection triggers thrombotic thrombocytopenic purpura by producing the anti-ADAMTS13 IgG inhibitor: Intern Med, 2010; 49; 689-93
15.. Ning J, Guan X, Li X, Case of acquired thrombotic thrombocytopenic purpura associated with influenza A (H1N1) virus and literature review: J Paediatr Child Health, 2021; 57; 282-85
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133