01 October 2021: Articles 
Bilateral Facial Palsy and Hyperreflexia as the Main Clinical Presentation in Guillain-Barré Syndrome
Unusual clinical course, Challenging differential diagnosis
Ghada Albuainain1ABCDEF*DOI: 10.12659/AJCR.932757
Am J Case Rep 2021; 22:e932757






Abstract
BACKGROUND: Guillain-Barré syndrome (GBS) is an autoimmune disease of the peripheral nervous system. It has multiple presentations, demyelinating or axonal, according to the pattern of injury. In general, there are cardinal symptoms, such as areflexia and ascending symmetrical lower limb weakness. GBS has multiple different variants. Acute inflammatory demyelinating polyradiculoneuropathy (AIDP) is the most common type. Other known variants are acute motor and sensory axonal neuropathy, acute motor axonal neuropathy, acute sensory neuropathy, acute pan dysautonomia, and Miller Fisher syndrome.
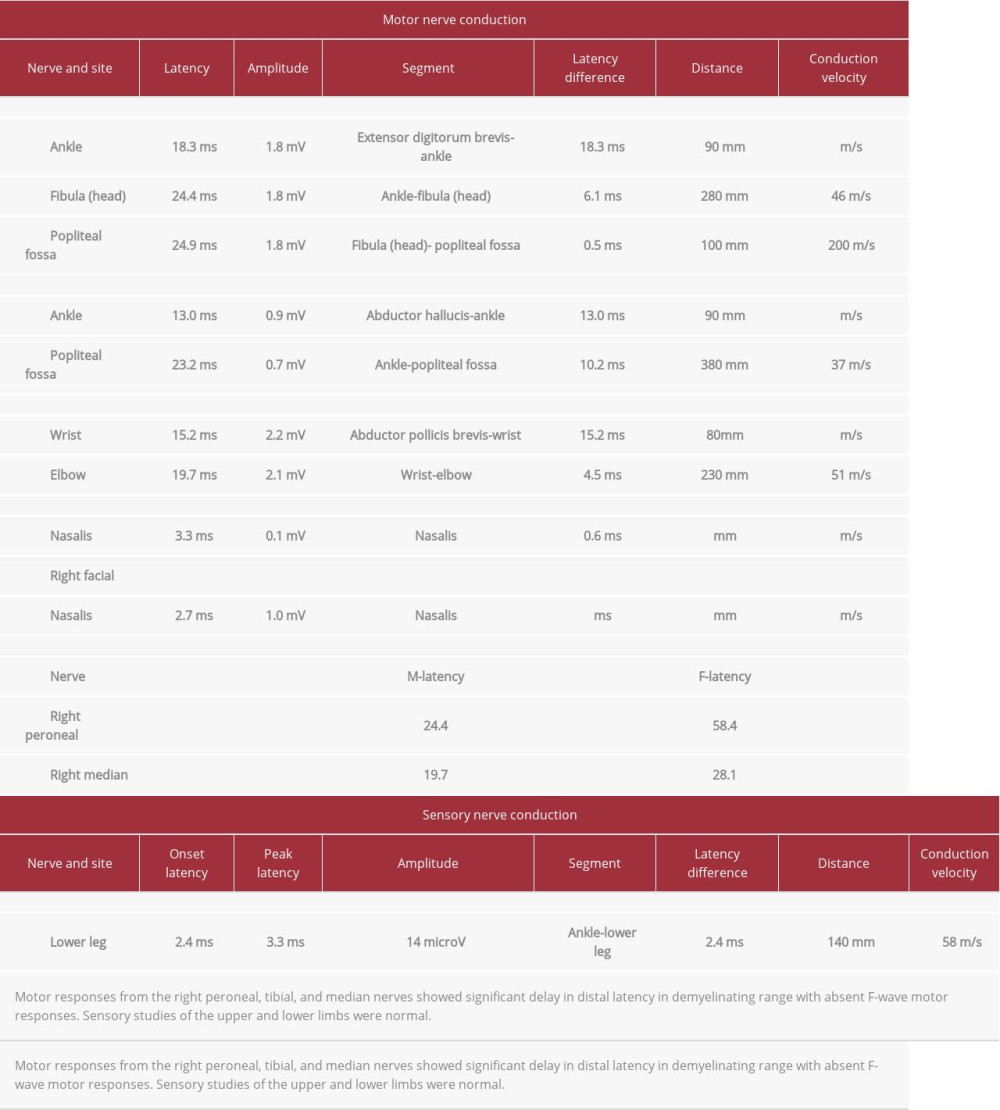
CASE REPORT: In the present case, the patient had initial symptoms of distal bilateral paresthesia and 12 days later he developed left facial muscle weakness, a decrease in ability to taste, and right facial muscle weakness. Two days later the patient said he did not have limb weakness. On examination, he had bilateral lower motor facial palsy, the power in his upper and lower right limbs was 4/5, and he had bilateral upper limb hyperreflexia. Results of a nerve conduction study were consistent with acute demyelinating polyneuropathy with secondary axonal loss. The patient was treated with immunoglobulin G, 0.4 mg/kg/d for 5 days, and fully recovered.
CONCLUSIONS: Facial diplegia is one of the GBS variants that presents rarely as pure bilateral facial weakness or is preceded by bilateral lower limb weakness. The present case underscores that patients with GBS may have facial diplegia before weakness. Also, they may not have areflexia as a cardinal feature, and instead, hyperreflexia may be seen. Although hyperreflexia has been reported in association with the acute motor axonal variant, the present case shows that hyperreflexia also can be found with AIDP.
Keywords: Facial Nerve Diseases, Guillain-Barre Syndrome, Reflex, Abnormal, Autoimmune Diseases, Facial Paralysis, Humans, Miller Fisher Syndrome
Background
Guillain-Barré syndrome (GBS) is a group of autoimmune diseases that affect mainly the peripheral nervous system, commonly with either a demyelinating or axonal pattern. The incidence is 1.1 to 1.8 per 100 000 persons per year worldwide [1] and the mortality rate varies from 0% to 8%, with a higher rate in patients who require mechanical ventilation or who are very elderly or have multiple comorbidities [2]. GBS can have motor, sensory, and/or autonomic manifestations. They differ according to the pattern of involvement.
The present case report describes a patient who had an unusual clinical course because he developed distal limb paresthesia and facial diplegia without limb weakness. He had mild right weakness in his right limb 2 days after experiencing weakness in his facial muscles, whereas limb weakness usually precedes facial muscle weakness. In similar cases, early diagnosis and management are crucial because facial muscle weakness portends a poor prognosis and patients should be assessed urgently for the need for ventilatory support [3]. Also, the presence of hyperreflexia with facial diplegia indicates a need to consider other differential diagnoses, but it should not delay management.
Case Report
In January 2018, a 37-year-old right-handed man who had no chronic medical conditions presented with a 2-week history of distal limb paresthesia and a severe occipital headache. These symptoms were associated with generalized fatigue and loss of the ability to taste, which had started 12 days before. He then developed left facial weakness, followed by right facial weakness 2 days later. The patient had no change in level of consciousness and no fever, diarrhea, or stress preceded his symptoms. In the past 6 months, he had lost 23 kg because of being on a restrictive diet.
On physical examination, the patient was a conscious, oriented, and alert middle-aged man who was stable but unable to close his eyes completely, raise his eyebrows, blow his cheeks, purse his lips, or smile, but who had preserved sensation in his face. His muscle tone was normal on motor examination but he had a power of 4/5 in his right distal upper and lower limb and 5/5 in his left limbs. The patient’s reflexes were +1 in his lower limbs and +3 in his upper limbs, based on plantar examination. His plantar reflexes, sensation, gait, and coordination were normal.
Laboratory test results were normal, including screening for HIV, angiotensin-converting enzyme, and Lyme disease. A cerebrospinal fluid (CSF) analysis showed only slight elevation in immunoglobulin G with no evidence of albumin cytological dissociation.
Neuroimaging studies including contrast-enhanced magnetic resonance imaging (MRI) of the brain and spine were normal.
The results of a nerve conduction study were consistent with acute inflammatory demyelinating polyradiculoneuropathy (AIDP) with secondary axonal loss (Table 1)
Based on the patient’s history, clinical presentation, and laboratory workup, we diagnosed him with AIDP-GBS. We treated him with i.v. immunoglobulin G (IVIg), 0.4 g/kg/d for 5 days, for a total dose of 40 g. The patient recovered 5 days after starting IVIg and at 1-month follow-up, he had mild facial palsy.
Discussion
GBS is an immune-mediated disease of the peripheral nervous system that is associated with a provoking factor, such as infection with
There are multiple variants of GBS. The most common ones are AIDP, Miller Fisher syndrome, acute motor axonal neuropathy (AMAN), and acute sensorimotor axonal neuropathy (AMSAN). Other variants are Bickerstaff encephalitis and pharyngeal-cervical-brachial and bifacial weakness.
The diagnosis of GBS is based on a patient’s clinical presentation and electrophysiological findings, which differ according to the variant. While the AIDP variant is the most common, the classical clinical presentation is bilateral symmetrical ascending weakness with hyporeflexia and electrophysiological evidence of demyelination, such as decreased motor nerve conduction velocity, prolonged distal motor latency, increased F-wave latency, conduction blocks, and temporal dispersion. Another variant is AMAN. It is acute axonal and usually preceded by a
Bilateral facial weakness is a variant present in 14% of patients with GBS [3]. It is usually accompanied by limb pares-thesia and areflexia with absence of ophthalmoplegia or limb weakness [4]. The presence of facial weakness usually signifies poor prognosis and is indicative of a possible need for ventilatory support [3]. Therefore, early management is crucial. In our patient, the presence of hyperreflexia and development of limb weakness after weakening of facial muscles underscores the importance of early diagnosis and exclusion of other differential diagnoses, such as infectious, metabolic, vascular, neoplastic, and immunological diseases.
The most common infectious cause of bilateral facial weakness is Lyme disease, which is a spirochetal infection transmitted by a tick bite. It is endemic in the United States and patients with it present with multiple disseminated erythema migrans within days to weeks of the tick bite. After that, they develop cardiological and neurological manifestations.
Our patient reported no history of travel to an endemic area or exposure to a tick bite. He also had no skin lesion.
We also considered sarcoidosis because 50% of patients with it have a neurological manifestation of the disease that includes facial diplegia. However, our patient’s calcium level was normal and testing for angiotensin-converting enzyme was negative.
A computed tomography scan, angiogram, and perfusion all were sufficient to rule out vascular causes and brain stem lesions. Testing for erythrocyte sedimentation rate, C-reactive protein, and an immunological workup were negative, which ruled out vasculitis as a cause of facial diplegia that occurs with polyarteritis nodosa, systemic lupus erythematosus, and Sjogren syndrome.
A contrast-enhanced MRI of the patient’s brain and CSF analysis showed no evidence of multiple sclerosis. In addition, the radiological images ruled out any neoplastic causes, such as leukemia, lymphoma, or pontine glioma.
Simultaneous bilateral facial palsy is rare, but GBS is one of the most common differential diagnoses for this presentation. It usually occurs in ascending patterns. In most cases, limb weakness precedes facial muscle weakness, except for isolated facial diplegia as a rare variant of GBS in which limb weakness may not occur [4]. Our patient developed facial weakness before limb weakness, which is unusual. He also presented with hyperreflexia, which reportedly is seen mainly with the acute motor axonal variant and usually preceded by
Other cases have been reported of patients with GBS who presented with acute facial diplegia, but most of them had associated paresthesia and decreased deep tendon reflexes [4]. Loss of taste is usually not appreciated by patients with uni-lateral facial palsy, but it is noticed when there is bilateral facial palsy when both chorda tympani branches of facial nerves are affected.
Our patient’s presentation was unusual, in that he had acute facial diplegia that preceded lower limbs weakness, along with hyperreflexia. There was no evidence of albumin cytological dissociation and a nerve conduction study was suggestive of demyelinating polyneuropathy.
Conclusions
Facial diplegia is a common presentation of GBS, which typically but not exclusively occurs after ascending lower limb weakness. Patients with GBS can have facial diplegia as their only symptom or before limb weakness. Areflexia is not always a cardinal feature of the condition instead hyperreflexia has been reported but in association with an AMAN variant, which was not the case in our patient, who had AIDP. Given a presentation such as our patient’s, careful assessment, early diagnosis, and consideration of other differential diagnoses are crucial.
References:
1.. McGrogan A, Madle GC, Seaman HE, de Vries CS, The epidemiology of Guillain-Barré syndrome worldwide. A systematic literature review: Neuroepidemiology, 2009; 32(2); 150-63
2.. Benamer HT, Bredan A, Guillain-Barré syndrome in Arab countries: A systematic review: J Neurol Sci, 2014; 343(1–2); 221-23
3.. D’Amore A, Viglianesi A, Cavallaro T, Guillain-Barré syndrome associated with acute onset bilateral facial nerve palsies. A case report and literature review: Neuroradiol J, 2012; 25(6); 665-70
4.. Wakerley BR, Yuki N, Isolated facial diplegia in Guillain-Barré syndrome: Bifacial weakness with paresthesias: Muscle Nerve, 2015; 52(6); 927-32
5.. Baheti NN, Manuel D, Shinde PD, Hyperreflexic Guillain-Barré syndrome: Ann Indian Acad Neurol, 2010; 13(4); 305-7
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133