25 November 2021: Articles 
A Case of COVID-19-Associated Free-Floating Aortic Thrombus Successfully Treated with Thrombectomy
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment
Lisa Dao1ABDEF, Alina Lund1BEF, Christina D. Schibler1BEF, Christine A. Yoshioka1BEF, Maria Barsky1ACDEFG*DOI: 10.12659/AJCR.933225
Am J Case Rep 2021; 22:e933225






Abstract
BACKGROUND: COVID-19 caused by SARS-CoV-2 infection has been associated with a hypercoagulable state in which patients can be at risk for developing venous and arterial thromboembolic events at a rate as high as 31%. A free-floating aortic thrombus (FFT) is a rare life-threatening complication of a hypercoagulable state. These thrombi require medical, endovascular, or surgical treatment. The optimal treatment modality for FFT occurring in the setting of COVID-19 remains unknown. We present a patient with a COVID-19-associated free-floating descending aortic thrombus that was treated with percutaneous vacuum-assisted thrombectomy (angio-VAC).
CASE REPORT: A 61-year-old man presented to the hospital with dyspnea and hypoxia and was diagnosed with severe COVID-19 pneumonia. Initial chest computed tomography angiography (CTA) did not show pulmonary emboli or thrombi. Inflammatory markers (D-dimer, lactate dehydrogenase, ferritin, fibrinogen) were tracked every other day. After several measurements of decreasing D-dimer values, there was a noticeable increase in D-dimer level and continued dependence on high levels of supplemental oxygen. A repeat chest CTA showed an FFT, confirmed by transesophageal echocardiogram. Cardiothoracic surgery and interventional radiology teams performed successful angio-VAC percutaneous removal, confirmed with intravascular ultrasound. The patient was subsequently discharged with a 3-month supply of apixaban.
CONCLUSIONS: Minimally invasive endovascular removal of an FFT is a therapeutic option, as anticoagulation alone carries the risk of partial lysis and repeat embolization. Clinicians can consider this endovascular treatment option paired with therapeutic anticoagulation. Further guidelines on monitoring and treatment of possible COVID-19-associated thrombosis are needed, particularly when the risk of embolization is high.
Keywords: COVID-19, Thrombectomy, Thrombosis, COVID-19, Humans, Male, SARS-CoV-2
Background
A free-floating aortic thrombus (FFT) is a non-adherent thrombus that floats in the aortic lumen. Overall, an FFT is a rare phenomenon that is seldom seen in the absence of aortic aneurysm or atherosclerotic disease. When diagnosed in an otherwise normal aorta, the event is usually associated with a variety of conditions that predispose a patient to arterial thrombus formation, such as a genetic condition of hypercoagulability, trauma, malignancy, or prior surgery [1,2]. The diagnosis is typically made after an embolic event, but FFT can also be found incidentally or postmortem. Imaging modalities for localization include computed tomography angiography (CTA) and transesophageal echocardiogram [3,4]. Once diagnosed, traditional treatment options for FFT include anticoagulation, thrombectomy, thrombolysis, and endovascular grafting [5,6].
A more recent condition implicated in FFT formation is infection with the SARS-CoV-2 virus. Given the novelty of the SARSCoV-2 virus, the incidence of FFT and the best course of treatment in COVID-19 is still unknown. Although there are reports of COVID-19-associated arterial thromboembolisms, including FFT, there has been only 1 other report of thrombectomy for a COVID-19-associated thrombus discussed in the literature [7–10]. The present case describes a patient with COVID-19-related acute respiratory distress syndrome found to have an incidental FFT that was successfully treated with percutaneous vacuum-assisted aortic thrombectomy.
Case Report
The patient was a 61-year-old man with a history of hyper-tension who presented to the hospital for worsening cough and exertional dyspnea. On admission, polymerase chain reaction testing for SARS-CoV-2 was positive. He rapidly developed acute hypoxic respiratory failure, requiring supplemental oxygen through a high-flow nasal cannula (HFNC). Initial diagnostic imaging with CT pulmonary angiogram, performed owing to an initial elevation of D-dimer, hypoxia, and tachycardia, revealed extensive bilateral multifocal and confluent ground-glass opacities, but no thrombi (Figure 1). During the patient’s hospital course, he was treated with a 10-day course of dexamethasone, 5-day course of the antiviral medication remdesivir, pharmacologic thromboprophylaxis, and convalescent fresh frozen plasma under the FDA emergency use authorization.
Nine days into hospitalization, his pulmonary symptoms appeared to plateau, but he continued to require significant supplemental oxygen support through HFNC. His inflammatory markers, including high-sensitivity C-reactive protein, lactate dehydrogenase, ferritin, and D-dimer, showed a distinct rise after initially starting to downtrend (Table 1). This was most notable in his D-dimer value that increased almost 3-fold, from 2350 ng/mL to 6840 ng/mL (Figure 2). D-dimer is known to rise within 4 days of a thrombotic event and fall within 1 week of the event [11]. Owing to the patient’s sharp rise in D-dimer level and inability to wean from HFNC, there was concern for an interval thrombotic event. A repeat CT pulmonary angiogram was performed, which did not show any pulmonary emboli but revealed a new incidental finding of a 1.4-cm nodular filling defect within the distal aortic arch and proximal descending thoracic aorta, suggestive of an FFT (Figure 1). A transesophageal echocardiogram (Figure 3), followed by a CT aortogram, confirmed the presence of a 1.14×0.87-cm mobile thrombus in the distal aortic arch and proximal descending aorta. In both imaging modalities, the aorta was noted to be normal in size and structure without any evidence of aneurysm or dissection.
After the FFT was discovered, therapeutic anticoagulation with a heparin drip was initiated. The case was discussed jointly among the cardiothoracic surgery, vascular surgery, and interventional radiology teams, with a final decision to perform aortic mechanical thrombectomy using the Angio-Vac device (AngioDynamics, Latham, NY, USA). During the procedure, an aortic angiogram and intravascular ultrasound of the aorta ensured complete removal of any residual thrombus and confirmed no further embolization of the thrombus. The patient underwent the procedure with successful aspiration of the FFT. The specimen was sent for pathology testing, which identified only fibrin material (Figure 4).
The patient tolerated the procedure well and without complications. His inflammatory markers steadily decreased (Table 1). He was transitioned from a heparin drip to a direct-acting oral anticoagulant, apixaban (Eliquis), which he was instructed to continue for a duration of 3 months. The patient was successfully weaned to a nasal cannula and discharged to a skilled nursing facility for further rehabilitation owing to his physical deconditioning.
Discussion
Despite its novelty, the SARS-CoV-2 virus is an emerging disease that has already been implicated as a cause of coagulopathy. Increased rates of venous and arterial thromboembolisms occurring in individuals with COVID-19 have been reported [12]. While venous thrombotic events seem to occur more frequently, arterial thrombotic events, such as floating aortic thrombus, have also been described [7,8]. The pathophysiology of COVID-19-associated thrombosis and coagulopathy is thought to be secondary to a severe derangement of homeostasis due to an excessive immunologically mediated thrombogenic and hyperinflammatory response to SARS-CoV-2 infection. Laboratory features of patients with SARS-CoV-2 infection highlight this increase in inflammation and disruption in the production of coagulation factors and include elevated levels of D-dimer, factor VIII, fibrinogen, PT/aPTT, IL-6, TNF-alpha, and IL-1beta. The systemic cytokine production leads to platelet activation and interaction with neutrophils, creating neutrophil extracellular traps, which further stimulate fibrin deposition and thrombin production, leading to micro and macro thrombosis [13–15].
Diagnosing FFT in COVID-19 can be rather difficult because the clinical presentation of FFT can significantly vary, ranging from life-threatening distal embolization to other organs to asymptomatic disease [16]. While many FFTs are diagnosed after an embolic event, some are found incidentally or postmortem [3]. Some institutions have adopted the use of inflammatory markers as a surrogate for monitoring disease severity; however, there are no clear guidelines on the use of inflammatory markers to detect possible thrombosis secondary to COVID-19. The present case describes the use of inflammatory markers to further support a suspicion for new thrombosis. It is unclear whether the increases in D-dimer and high-sensitivity C-reactive protein in this case were coincidental findings or true correlates of a new thrombosis. Further data regarding inflammatory markers and their correlation with development of new thrombotic events needs to be obtained before additional inferences can be made. Because COVID-19 coagulopathy is a disturbance of homeostasis, some institutions have explored using clot waveform analysis, viscoelastic testing, and thrombin generation to detect a hypercoagulable state with promising results [13–15]. Perhaps guidelines should also address the use of these more precise tests of hypercoagulability in patients with COVID-19 in place of the less precise inflammatory markers that are more commonly used.
Because clear guidelines on monitoring for thrombosis do not currently exist, the present case further emphasizes the importance of appropriate pharmacologic thromboprophylaxis in all hospitalized patients with COVID-19. Even with proper pharmacological thromboprophylaxis, as this case demonstrates, thromboembolic events occur. The American Society of Hematology currently recommends using prophylactic-intensity anticoagulation over intermediate- and therapeutic-intensity anticoagulation in COVID-19-related critical illness and acute illness. The preliminary results of the REMAP-CAP, ACTIV-4a, ATTACC trials also do not currently support using therapeutic-intensity anticoagulation in patients with COVID-19 [17].
Once discovered, prompt treatment of an FFT is usually suggested, given that the rate of free-floating thrombi embolization has been described to be as high as 75%, compared with 12% for adherent thrombi [16,18]. Currently, however, the optimal treatment approach for aortic FFT is unclear, including those that occur in the setting of COVID-19. Therapeutic options that have been used for FFT include anticoagulation, thrombectomy, thrombolysis, and endovascular grafting [5,6]. The existing literature suggests that a more aggressive surgical approach may be preferable to anticoagulation alone due to the higher likelihood of persistent or recurrence thrombus in individuals primarily treated with anticoagulation [1,3]. The only other case of thrombectomy performed for a COVID-19-associated thrombus described by Schmid et al used an invasive open thrombectomy approach. The present case is unique because it demonstrates successful treatment of a COVID-associated FFT through a minimally invasive approach using percutaneous vacuum-assisted thrombectomy. The advantages of such a technique include decreased procedure time and thus decreased risk of exposure of staff to viral infection and faster postoperative recovery time.
Conclusions
With the increasing prevalence of COVID-19 worldwide, there is undoubtable concern for the subsequent downstream consequences of the disease, including, but not limited to, arterial and venous thromboembolic events. Further investigation to find the optimal method for treatment of and monitoring for resultant arterial and venous thromboembolism is crucial, given the possible morbidity and mortality that can result. This case further emphasizes the role of pharmacologic thromboprophylaxis in patients with COVID-19 that is stressed by the American Society of Hematologists and Cardiologists as well as the International Society on Thrombosis and Haemostasis. This case is one of the first in the literature to demonstrate the successful use of minimally invasive thrombectomy for treatment of a COVID-19-associated FFT.
Figures
References:
1.. Fayad ZY, Semaan E, Fahoum B, Aortic mural thrombus in the normal or minimally atherosclerotic aorta: Ann Vasc Surg, 2013(3); 282-90
2.. Fischer ML, Matt P, Kaufmann BA, An unusual cause of thromboembolic disease: Cardiovasc Med, 2015; 18; 229-30
3.. Tigkiropoulos K, Karamanos D, Tympanidou M, Aortic arch floating thrombus complicated by distal embolization in a patient with malignancy: Case Rep Vasc Med, 2018; 2018; 2040925
4.. Kim SD, Kwang JK, Lee JH, Free floating thrombus of the aorta: An unusual cause of peripheral embolization: J Korean Surg Soc, 2011; 80; 204-11
5.. Piffaretti G, Tozzi M, Mariscalco G, Mobile thrombus of the thoracic aorta: management and treatment review: Vasc Endovasc Surg, 2008; 42(5); 405-11
6.. Weiss S, Bühlmann R, von Allmen RS, Management of floating thrombus in the aortic arch: J Thorac Cardiovasc Surg, 2016; 152(3); 810-17
7.. De Carranza M, Salazar DE, Troya J, Aortic thrombus in patients with severe COVID-19: Review of three cases: J Thromb Thrombolysis, 2021; 51(1); 237-42
8.. Gomez-Arbelaez D, Ibarra-Sanchez G, Garcia-Gutierrez A, COVID-19-related aortic thrombosis: a report of four cases: Ann Vasc Surg, 2020; 67; 10-13
9.. Mosbahi S, Heinisch PP, Schoenhoff F, Berger D, COVID-19-associated aortic arch thrombus: Eur J Cardiothorac Surg, 2020; 58(4); 870
10.. Schmidt P, Vasquez J, Gagliano B, Ascending aortic thrombus with multiple emboli associated with COVID-19: Proc Bayl Univ Med Cent, 2020; 34(1); 178-79
11.. Goldin Y, Pasvolsky O, Rogowski O, The diagnostic yield of D-dimer in relation to time from symptom onset in patients evaluated for venous thromboembolism in the emergency medicine department: J Thromb Thrombolysis, 2010; 31(1); 1-5
12.. Klok FA, Kruip MJHA, van der Meer NJM, Incidence of thrombotic complications in critically ill ICU patients with COVID-19: Thromb Res, 2020; 191; 145-47
13.. Panigada M, Bottino N, Tagliabue P, Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis: J Thromb Haemost, 2020; 18; 1738-42
14.. Campello E, Bulato C, Spiezia L, Thrombin generation in patients with COVID-19 with and without thromboprophylaxis: Clin Chem Lab Med, 2021; 59(7); 1323-30
15.. Fan BE, Ng J, Chan SS, COVID-19 associated coagulopathy in critically ill patients: A hypercoagulable state demonstrated by parameters of haemostasis and clot waveform analysis: J Thromb Thrombolysis, 2020; 51(3); 663-74
16.. Avelino MC, Miranda CL, Sousa CS, Free-floating thrombus in the aortic arch: Radiologia Brasileira, 2017; 50(6); 406-7
17.. Zarychanski R, Therapeutic anticoagulation in critically ill patients with COVID-19 – preliminary report: MedRxiv, 2021; 2021; 21252749 [preprint]
18.. Karalis DG, Chandrasekaran K, Victor MF, Recognition and embolic potential of intraaortic atherosclerotic debris: J Am Coll Cardiol, 1991; 17; 73-78
Figures
Tables
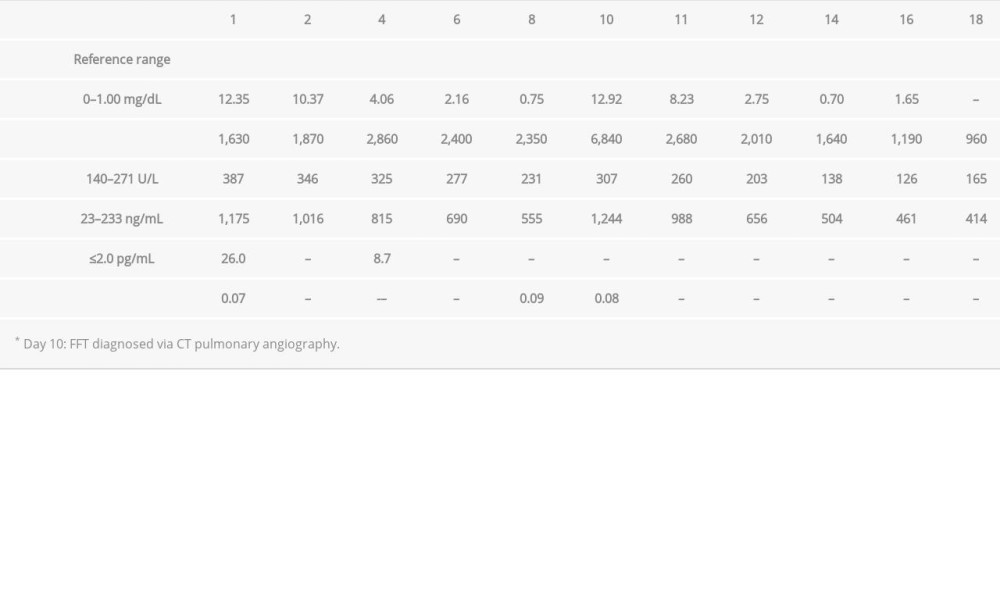 Table 1.. Trends of COVID-19 inflammatory markers, including high-sensitivity C-reactive protein, lactate dehydrogenase, D-dimer, ferritin, interleukin-6, and procalcitonin throughout the hospital course.Table 1.. Trends of COVID-19 inflammatory markers, including high-sensitivity C-reactive protein, lactate dehydrogenase, D-dimer, ferritin, interleukin-6, and procalcitonin throughout the hospital course.
Table 1.. Trends of COVID-19 inflammatory markers, including high-sensitivity C-reactive protein, lactate dehydrogenase, D-dimer, ferritin, interleukin-6, and procalcitonin throughout the hospital course.Table 1.. Trends of COVID-19 inflammatory markers, including high-sensitivity C-reactive protein, lactate dehydrogenase, D-dimer, ferritin, interleukin-6, and procalcitonin throughout the hospital course. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133