28 November 2021: Articles 
Acute Fatty Liver of Pregnancy
Management of emergency care, Rare disease
Ademayowa Ademiluyi1AEF*, Dominic O. Amakye1EF, Nicola Jackson1AE, Shion Betty1EDOI: 10.12659/AJCR.933252
Am J Case Rep 2021; 22:e933252






Abstract
BACKGROUND: Acute fatty liver of pregnancy (AFLP) is a rare obstetric emergency resulting from microvesicular infiltration of the liver by fat, leading to liver failure. It usually presents at 36 weeks of gestation, and risk factors include twin pregnancy and low BMI. The presentation of AFLP is nonspecific, requiring a high index of suspicion. The Swansea Criteria is used to aid diagnosis.
CASE REPORT: Case 1: A 23-year-old woman, G1P0 at 39 weeks of gestation, presented to the hospital with a 1-week history of fever, nausea, vomiting, and diarrhea. Examination revealed a gravid uterus with generalized abdominal tenderness. Laboratory investigations revealed elevated liver enzymes, with elevated total bilirubin and an INR of 1.26. CBC showed leukocytosis. Abdominal ultrasound was normal. Workup for other etiologies, including acetaminophen and salicylate overdose and infections, was negative. The Swansea score for AFLP was 8, confirming the AFLP diagnosis. An emergency Cesarean-section was performed, causing liver enzymes to improve over 3 days. Case 2: A 41-year-old woman, G1P1 with a twin gestation at 36 weeks, presented with a 3-day history of abdominal pain. She was jaundiced, with right upper quadrant tenderness. Laboratory investigations showed elevated liver enzymes and total bilirubin, with an INR of 1.26. Workup for viral hepatitis and autoimmune etiology was negative. Salicylate levels were within normal limits. She met criteria for AFLP and underwent emergency Cesarean-section. Liver enzymes improved over 4 days.
CONCLUSIONS: AFLP is a potentially life-threatening medical condition. From our experience, prompt diagnosis and early delivery leads to improved maternal and fetal outcomes.
Keywords: Acute Fatty Liver Of Pregnancy, Liver Diseases, Liver Failure, Acute, Cesarean Section, Fatty Liver, Female, Humans, Pregnancy, Pregnancy Complications, young adult
Background
Acute fatty liver of pregnancy (AFLP) is a life-threatening disease that occurs mostly around 36 weeks of gestation and is characterized by fatty infiltration of the liver, which causes hepatic failure. The prevalence is estimated to be 1 to 3 cases per 10 000 deliveries [1]. AFLP is an obstetric emergency that can be detrimental to the fetus and mother. Given the medical advances that have been made over the years, maternal and fetal mortality has decreased. However, developing nations could see a higher mortality rate because of their lack of capacity to provide intensive care [8]. Here we present 2 patients in their 36th week of pregnancy who developed acute liver failure.
Case Reports
CASE 1:
A 23-year-old woman, who was gravida 1 para 0 at 39 weeks of gestation with no significant past medical history, presented to the Emergency Department (ED) with a 1-week history of nausea, vomiting, and diarrhea. She also had abdominal pain associated with fevers, with a maximum temperature of 38.9°C. She was on prenatal vitamins and no other medications.
On physical examination, she was lethargic, and her vital signs were significant for tachycardia at 100 beats per min. Otherwise, all vital signs were within normal limits. No scleral icterus was found on examination. Her abdomen was soft and nondistended, but there was generalized tenderness to palpation in all quadrants. The Murphy sign was negative, and bowel sounds were normoactive.
Initial laboratory blood work revealed a bicarbonate level of 8 mmol/L, and blood urea nitrogen and creatinine levels were 22 and 2.0 mg/dL, respectively. The alkaline phosphatase level was 324 U/L (reference range, 32–126 U/L), aspartate transaminase (AST) was 833 U/L (range, 12–50 U/L), and alanine transaminase (ALT) was >500 U/L (range, 7–52 U/L). The total bilirubin was 3.5 mg/dL, prothrombin time was 14.4 s, and international normalized ratio (INR) was 1.26.
The complete blood count showed leukocytosis of 18 100 cell/ µL, with 90% neutrophilia, platelet count of 295 000 cell/µL, ammonia of 79 umol/L, acetaminophen level <10, and glucose level of 52 mg/dL. An abdominal ultrasound showed normal liver echogenicity, with no ascites or hepatomegaly. Further workup, including a hepatitis panel and rubella and Leptospira antibody tests, was negative. Using the Swansea Criteria, she was diagnosed with AFLP. The patient underwent an emergent Cesarean section on day 1 of hospitalization after severe fetal distress was noted. Her liver function subsequently began to improve. AST and ALT levels improved to 89 U/L and 152 U/L, respectively, and total bilirubin and ALP levels normalized. The patient was discharged on day 3 of hospitalization with a healthy baby girl.
CASE 2:
A 41-year-old woman, gravida 2 para 1, who was pregnant with a twin gestation at 36 weeks of gestation, presented to the ED with abdominal pain, chills, nausea, vomiting, and light-headedness of 3 days. She had a past medical history of hypothyroidism. She was taking prenatal vitamins, and her medications included acetaminophen 1000 mg to 2000 mg every 4 h over the last 3 days prior to presentation at the hospital.
On arrival to the ED, her blood pressure was 144/86 mmHg, heart rate was 89 beats per min, temperature was 36.1°C, and respiratory rate was 20 breaths per min. On physical examination, she was found to have scleral icterus, yellowish discoloration of the skin, right upper quadrant abdominal tenderness, present normoactive bowel sounds, and uterine fundus palpable 1 cm below the xyphoid process. Laboratory evaluation showed leukocytosis of 13.6 cell/µL, with 79% neutrophil predominance, platelet count of 181 000 cell/µL, creatinine level of 2.07 mg/dL (baseline creatinine 0.7–0.9 mg/dL), albumin of 3.2, total protein of 6.1, total bilirubin of 4.2, with direct bili-rubin of 2.87 mg/dL, AST >500, ALT >1000, ALP of 409, INR of 1.34, PT of 15.2, PTT of 45.9, glucose of 56 mg/dL, negative hepatitis panel, ferritin of 231.9, LDH of 997, acetaminophen level of 16.1, salicylate level <2.5, C-reactive protein level of 3.99, ceruloplasmin of 45, negative antinuclear antibodies, and fibrinogen of 88. A right upper quadrant ultrasound of the abdomen showed mild increased echogenicity of the liver, which could be seen with fatty infiltrates.
She was diagnosed with AFLP and underwent a Cesarean section of a monochorionic diamniotic twin gestation on day 2 of hospitalization. On day 4 of hospitalization, her laboratory findings improved, including AST of 145, ALT of 142, ALP of 301, total bilirubin of 3.9 mg/dL, creatinine of 1.23 mg/dL, fibrinogen of 198, and INR of 1.1. She was discharged home with healthy twin baby boys.
Discussion
Acute fatty liver disease of pregnancy (AFLP) is a rare and potentially fatal disease, which usually affects women in their third trimester of pregnancy. Its incidence ranges from 1: 7000 to 1: 15 000 in the United States. Rarely, it can present at as early as 22 weeks, but it is usually seen after 30 weeks of gestation. The pathophysiology of AFLP is related to defects in fatty acid metabolism during pregnancy. Long-chain 3-hydroxyacyl CoA dehydrogenase (LCHAD) is one of the most commonly documented enzymes affected in patients with AFLP. Common risk factors associated with AFLP include, but are not limited to, nulliparity with a male fetus, multiple pregnancies, low body mass index less than 20 kg/m2, and preeclampsia [6].
The clinical presentation for AFLP includes persistent nausea and vomiting, which occurs in 80% of patients, lethargy, abdominal pain, and jaundice. Some patients with AFLP can also rarely present with pancreatitis [3]. AST and ALT levels are usually elevated 5 to 10 times the upper limit of normal [2]. Clinical signs and symptoms as well as laboratory findings are key instruments that can help in making the diagnosis and also in differentiating AFLP from other diseases commonly seen in pregnancy, such as intrahepatic cholestasis of pregnancy, HELLP syndrome, and preeclampsia. Having a broad differential is very important in pregnant woman because most of these pathologies can present similarly. AFLP can further be differentiated from other pathologies, like preeclampsia and HELLP syndrome, with the presence of abnormal synthetic liver function, which can present as an elevated INR and encephalopathy [2]. It has also been documented in the literature that COVID-19 can cause an elevation in liver enzymes, which subsequently corrects after delivery [9]. Unlike other similar pathologies, AFLP can present with other laboratory abnormalities, as listed in Table 1. Tools like the Swansea criteria in addition to a thorough history and physical examination can help narrow down these differentials.
Swansea criteria have been put forward as a tool to aid in the diagnosing of AFLP. In a small study of about 24 patients, the Swansea criteria was found to be effective, with a sensitivity of 100% and specificity of 57%. It was also found to have a positive predictive value of 85% and a negative predictive value of 100% [8]. The Swansea criteria are positive when at least 6 of the 15 criteria are fulfilled. Since AFLP is a diagnosis of exclusion, the Swansea criteria is intended to be used when other diagnoses have been excluded or are less likely.
Our first patient met 8 of 15 of the Swansea criteria (Table 1): vomiting, abdominal pain, encephalopathy, elevated bilirubin >0.8 mg/dL, leukocytosis greater than 11 000 cell/µL, elevated AST and ALT greater than 400 U/L, elevated bilirubin >0.4 mg/dL, and elevated ammonia, with the absence of other pathologies. Ultrasound did not show the classic hyperechogenic of the liver in the first patient case. Our second patient, on the other hand, had also met 8 of 15 of the Swansea criteria, with an ultrasound showing “bright liver”.
Elevated hepatic transaminases, hyperbilirubinemia, and coagulopathy appear to be nearly universal in patients with AFLP. Encephalopathy, elevated ammonia levels, hypoglycemia, and transient diabetes insipidus are relatively specific for hepatic injury and strongly support the diagnosis of AFLP but may be present in a minority of patients with the condition. The remaining features of the Swansea criteria are less specific in differentiating AFLP from other disorders [5]. The definitive management of AFLP is prompt delivery of the fetus and supportive care. Improvement is usually observed in 1 to 2 days after delivery [4]. Maternal mortality rates in patients with AFLP have improved in recent decades, with global mortality now being below 10% [6]. One in five women have reported having recurrent AFLP, with most cases being mild [7]. LCHAD was not tested in any of our patients because this test was not available at our facility.
Our patients continued to improve clinically during their hospitalization. Their AST and ALT levels trended downward following Cesarean section.
Conclusions
In conclusion, having a very high index of suspicion for AFLP is imperative in preventing maternal and fetal demise. Because AFLP is a rare disease, most of our understanding and education are based on small retrospective case reports [8]. More research needs to be done to properly understand this rare and fatal condition.
Tables
Table 1.. Swansea criteria.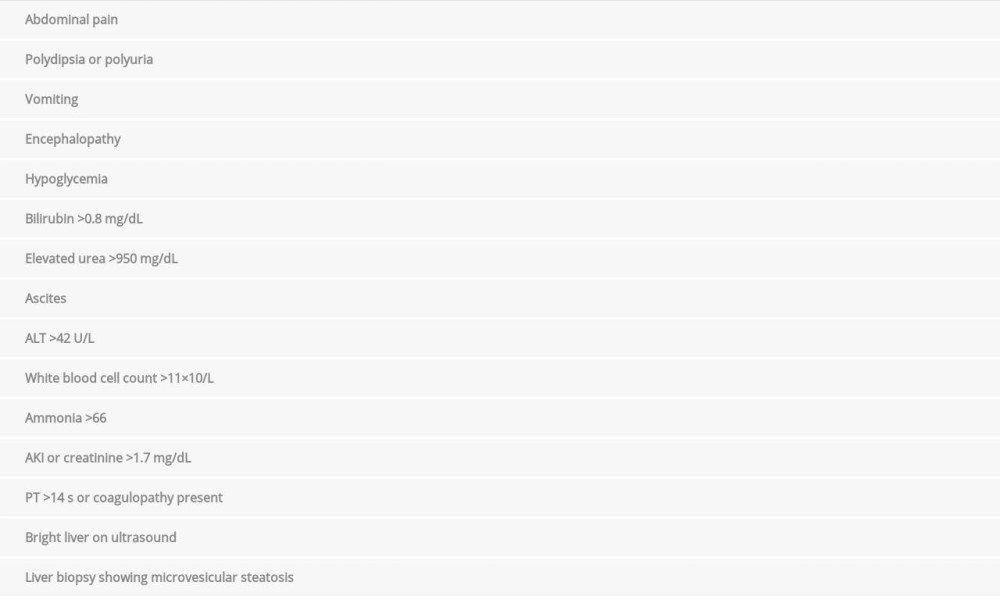
References:
1.. Naoum EE, Leffert LR, Chitilian HV, Acute fatty liver of pregnancy: Pathophysiology, anesthetic implications, and obstetrical management: Anesthesiology, 2019; 130(3); 446-61
2.. Tran TT, Ahn J, Reau N, ACG Clinical Guideline: Liver disease and pregnancy: Am J Gastroenterol, 2016; 111(2); 176-94
3.. Moldenhauer JS, O’Brien JM, Barton JR, Sibai B, Acute fatty liver of pregnancy associated with pancreatitis: A life-threatening complication: Am J Obstet Gynecol, 2004; 190(2); 502-5
4.. Ziki E, Bopoto S, Madziyire MG, Acute fatty liver of pregnancy: A case report: BMC Pregnancy Childbirth, 2019; 19; 259
5.. Morton A, Laurie J, Physiological changes of pregnancy and the Swansea criteria in diagnosing acute fatty liver of pregnancy: Obstet Med, 2018; 11(3); 126-31
6.. de Vasconcelos GA, Ascensão TC, Santos SI, Acute fatty liver of pregnancy: Rare, but potentially fatal: Am J Case Rep, 2020; 21; e921122
7.. Glavind J, Boie S, Glavind E, Fuglsang J, Risk of recurrent acute fatty liver of pregnancy: Survey from a social media group: Am J Obstet Gynecol MFM, 2020; 2(2); 100085
8.. Liu J, Ghaziani TT, Wolf JL, Acute fatty liver disease of pregnancy: Updates in pathogenesis, diagnosis, and management: Am J Gastroenterol, 2017; 112(6); 838-46
9.. Nkeih C, Sisti G, Schiattarella A, Elevated transaminases in a COVID-19 positive patient at term of gestation: A case report: Acta Biomed, 2020; 91(3); e2020002
Tables
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133