04 October 2021: Articles 
Optimizing Early Rehabilitation Intervention: Insights from Different Outcomes in 2 Patients with Severe COVID-19
Unusual setting of medical care
Yose Waluyo1ABCDEF*, Sari Rajwani Artika2BCDEF, Insani Nanda Wahyuni2BCDEF, Septianto Dwi Valen2BEF, Nuralam Sam1ABCDEFDOI: 10.12659/AJCR.933329
Am J Case Rep 2021; 22:e933329






Abstract
BACKGROUND: Coronavirus disease 2019 (COVID-19) is an emerging infectious disease first reported in Wuhan, China in December 2019 that has subsequently become pandemic worldwide. The more severe the symptoms, the more comprehensive and complex are the methods needed to treat patients. The World Health Organization (WHO) has highlighted the role of rehabilitation as one of the pillars in COVID-19 management, considering its advantages. It has been implemented in some countries’ guidelines, but it is not stated in Indonesia’s guideline. Thus, rehabilitation intervention is sometimes neglected or delayed. This case report aims to describe the possible benefit of optimizing the rehabilitation program during hospitalization.
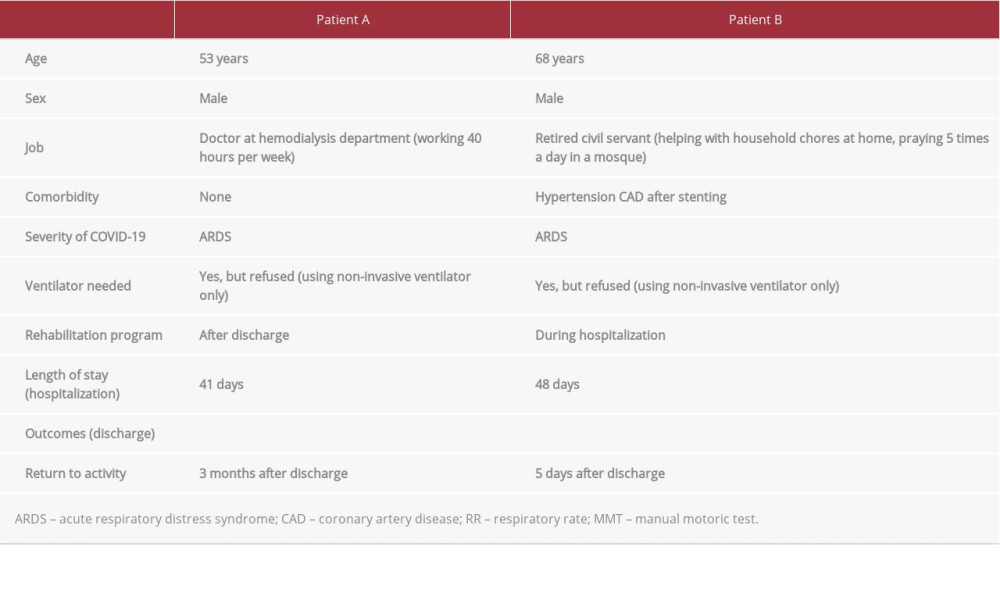
CASE REPORT: We describe 2 patients with severe COVID-19: Patient A was a 53-year-old man without comorbidities and Patient B was a 68-year-old man with several comorbidities. Patient A was discharged from the hospital with respiratory sequelae (dyspnea, cough, and desaturation) and muscle weakness in both limbs after 2 months of hospitalization without rehabilitation intervention. Then, he returned to work 3 months after rehabilitation. Patient B was discharged without any significant sequelae after undergoing rehabilitation during hospitalization.
CONCLUSIONS: Early physical rehabilitation in severe cases of COVID-19 has several potential benefits, including improved muscle strength, physical function, and quality of life, as well as reduced health care costs and length of stay (LOS). We believe that an early rehabilitation program in severe cases of COVID-19 is needed, but the physician still has to consider the patients’ condition and capacity into to decide what kind of exercise should be programmed by the team.
Keywords: COVID-19, Physical and Rehabilitation Medicine, severe acute respiratory syndrome coronavirus 2, COVID-19, Hospitalization, Humans, Pandemics, Quality of Life, SARS-CoV-2
Background
Coronavirus disease 2019 (COVID-19) is an emerging infectious disease first reported in Wuhan, China in December 2019 that has subsequently become pandemic worldwide [1]. Huang et al reported several symptoms of COVID-19, ranging from no symptoms to severe symptoms. Fever, cough, myalgia or fatigue, and developed dyspnea are the most common symptoms. Less common symptoms are sputum production, headache, hemoptysis, and diarrhea [2]. The life-threatening form of respiratory failure, acute respiratory distress syndrome (ARDS), usually develops in COVID-19 patients within 8-12 days from onset [3,4]. The more severe the symptoms, the more comprehensive and complex are the methods needed to treat the patient.
Rehabilitation has several advantages, such as optimizing health and functional outcomes and facilitating early discharge from the Intensive Care Unit (ICU) [5]. The WHO has highlighted the role of rehabilitation as one of the pillars of COVID-19 management [6]. Some countries’ guidelines also recommend early rehabilitation in acute care hospitals, including early mobilization, respiratory management, and functional exercises, such as in Switzerland, Australia, and Poland [7–9]. However, it is unclear when is the best time to start rehabilitation to maximize benefits for COVID-19 patients. Unfortunately, the rehabilitation approach is not in Indonesia’s guidelines for COVID-19 management. Therefore, rehabilitation is sometimes neglected or delayed [10]. This neglected or delayed action may end up costing more and causing other disadvantages for the patient.
Here, we report 2 cases of severe COVID-19. This case report aims to describe the possible benefits of an early rehabilitation program in patients with COVID-19 during their hospitalization to maintain and improve the quality of life (return to work), as well as reduced length of hospitalization and healthcare cost.
Case Reports
PATIENT A:
A 53-year-old man came to the rehabilitation clinic by wheel-chair with lower-extremities weakness, shortness of breath, cough, and dependence on supplemental oxygen after 2 months of hospitalized due to severe COVID-19. Based on his history, the patient was initially admitted to the ICU due to ARDS. He did not get any rehabilitation program from when he was admitted until discharge from the hospital. No comorbidities were reported.
The initial physical examination in the clinic revealed respiratory rate (RR) 45 breaths per minute, oxygen saturation 92% on 4 liters/min oxygen via nasal cannula and 82–86% without any oxygen support, hip flexor and extensor MMT grade 1, knee extensor and flexor MMT grade 2, and plantar flexion and extension MMT grade 2. We also found muscle atrophy in his lower extremities, including the quadriceps, gastrocnemius, and hamstring muscles, as well as hamstring tightness and pain in the quadriceps area.
The rehabilitation team consisted of a PMR (physical medicine and rehabilitation) specialist and physiotherapists. The PMR specialist determined the health problems of the patient, and designed the rehabilitation program, including the therapy, frequency, intensity, and duration. He also evaluated the progress of rehabilitation every 2 weeks. The physiotherapists performed the physical therapies, as instructed by the PMR specialist, using modalities and exercises such as neuromuscular electrical stimulation (NMES), gradual strengthening exercise, breathing exercise, gentle stretching, aerobic exercise, and core stability exercise 3 times a week for 3 months. NMES was done for quadriceps muscles, tibialis anterior muscles, and erector spinae muscles. NMES stimulates the nerves in muscles to restore function and strength, prevent muscle atrophy, and reduce muscle spasms. Gentle stretching was done for ham-string muscles and gluteal muscles. Stretching aims to help improve flexibility and reduce tightness. Gradual strengthening exercise aims to increase muscle tone, followed by muscle strengthening. Core stability exercise was performed to strengthen the deep muscles, including the pelvic floor muscles, transversus abdominis, multifidus, internal and external obliques, rectus abdominis, erector spinae, and diaphragm. The exercises were core strengthening, such as prone extension and active straight leg raise. Aerobic exercises were performed using an ergo-cycle to improve the cardiopulmonary capacity and breathing exercise, which is essential to perform in all stages of COVID-19 disease, especially in severe cases.
After 3 months of the rehabilitation program, the patient could breathe adequately, with a 96–98% oxygen saturation without any oxygen support, and he could walk independently, with MMT grade 5 for all lower-extremity muscles.
PATIENT B:
A 68-year-old man presented with shortness of breath for 2 weeks. He had a cough with massive sputum, runny nose, and malaise, but no fever. The symptoms worsened 2 days before admission. Crackles were heard all over his lung fields. He was afraid to be brought to the hospital due to the COVID-19 outbreak. A week before he experienced symptoms, he had met with a sick relative.
There was a history of coronary stenting 6 months ago. He had uncontrolled hypertension. The vital signs at admission were: blood pressure 139/83 mmHg; pulse rate 97 bpm; respiratory rate 30 breaths per min temperature 36.9°C; and oxygen saturation was 83% on 5 L oxygen per min via nasal cannula. He tested positive for the PCR swab test and brought to the ICU. He was referred to the PMR specialist by a pulmonologist for rehabilitation. The rehabilitation therapies started on the ninth day of hospitalization.
The rehabilitation team consisted of a PMR specialist, a general practitioner, physiotherapists, and nurses. The PMR specialist was responsible for determining the problem and designing the rehabilitation program, including the therapy, frequency, intensity, duration, and time of day, and also evaluated the progress of rehabilitation with the pulmonologist every day. The general practitioner had the responsibility in the ward to report patient’s condition, especially for the necessary changes such as heavy sputum production, desaturation, and weakness. The physiotherapists conducted the therapy based on the PMR specialist’s instructions, with 1 session a day for 30–45 min. The nurses helped to position and mobilize the patient early with 5–8 sessions per day for 5–15 min or for as long as the patient can tolerate it.
We conducted rehabilitation therapies every day for 39 days with the following exercises: prone position+postural drainage+breathing exercise to improve dyspnea; active ROM exercise+breathing exercise (deep breathing+pursed lips breathing) to strengthen respiratory muscles; stretching+breathing exercise+chest expansion exercise to help thoracic expansion; postural drainage+effective cough breathing to help airway clearance, and gradual mobilization+walking as the patient could tolerate+active ROM exercise to strengthen extremities muscles.
We did follow-up every 3 days, and in each evaluation we observed improvement of his condition, such as reduction of sputum, improvement of symptoms and general condition, and chest X-ray improvement. Dyspnea improved on day 15 and coughing was reduced on day 21. Since day 24, the patient was only supported by oxygen 7–10 L/min via non-rebreathing mask, and the oxygen dosage gradually decreased. On day 39 he only needed oxygen 2–4 L/min via nasal cannula. On day 45 oxygen administration was discontinued. On day 48, with oxygen saturation 97%, the patient was discharged and continued self-isolation at home.
Discussions
As shown in Table 1, both of these patients had severe COVID-19. Even though Patient B was older than Patient A and had comorbidities, his outcomes were much better. Patient A underwent a long rehabilitation program after discharge, resulting in financial burden to the patient and family. The better outcome in Patient B might be the result of an earlier rehabilitation approach during hospitalization.
Bagnato et al highlighted the muscle weakness after ICU care due to COVID-19 in their case report. The patient was moved to the rehabilitation unit after a negative PCR swab test obtained on day 68 of hospitalization and spent 60 more days to improved her muscle strength with rehabilitation intervention [11]. Jaewon et al reported the case of a critically ill inpatient who received early rehabilitation intervention. After receiving 3 sessions of rehabilitation therapy, lower-limb muscle strength, balance function, and gait speed considerably improved on day 38 [12]. These case reports are similar to our finding in this study. They also emphasize the importance of optimizing the early rehabilitation in COVID-19 patients.
Based on WHO guidelines on COVID-19 management, early rehabilitation programs were recommended to be performed [6]. To the best of our knowledge, no clinical study has evaluated early rehabilitation effects on COVID-19 patients to date. However, an earlier rehabilitation program for acute respiratory failure in the ICU setting has been proven to increase survival rate, increase successful extubation rate, reduce mechanical ventilation (MV) duration, reduce ICU and hospital stays, and lower medical costs [13].
Early rehabilitation in COVID-19 patients, especially in severe cases, is still debatable in terms of the exact time of rehabilitation. Li stated that there is still much skepticism about rehabilitating severe COVID-19 patients; however, there are several therapies that can be performed, such as applying breath training in the prone position, moderate head elevation, active/passive mobilization of limbs, and also sitting and standing by the bedside [14]. Based on Kurtais et al reported that COVID-19 patients who developed acute respiratory distress syndrome (ARDS) should have limited exercise, such as passive movement and secretion control [15]. However, Righetti et al recommended ventilation for 12–16 h a day in the prone position for patients with severe ARDS, which should be discontinued if the patient exhibits hemodynamic instability [16]. Semi-prone, prone, semi-sitting, and sitting position are recommended for severe COVID-19 patients with spontaneous breathing or non-invasive ventilator support are clinically stable. Patients who have recovered from ARDS and are in the early phase of severe COVID-19 may benefit from active exercises and electrical muscle stimulation (EMS) to prevent ICU-acquired weakness [15,17]. Critical COVID-19 patients who are unconscious or sedated still need early mobilization and exercises such as positioning with 45° head up in bed, passive movement for all joints, and postural changes by gradually increasing the antigravity position to semi-sitting position might also prevent decubitus, and/or neuromuscular electrical stimulation to prevent the sequelae after being in bed for many days [18–20]. These therapeutic approaches must be selected based on the clinical condition of the patient and are important for the prevention of skin lesions, immobilized sequelae, and disabilities [17,19,20]. Active mobilization should be considered once the patient’s sedation is reduced to avoid severe myopathy and physical disability, but is not recommended if the patient is clinically unstable [17]. In addition, it has been shown in patients with severe COVID-19 who received physical, respiratory, and cognitive rehabilitation based on their clinical state have a shorter length of stay and improved cognitive function [21].
Conclusions
Early rehabilitation in patients with severe COVID-19 has several potential benefits, including improved muscle strength, physical function, and quality of life, as well as reduced health care costs and length of stay (LOS). We believe that an early rehabilitation program in severe cases of COVID-19 is needed, but the physician still has to consider the patients’ conditions and capacity in deciding which exercises will be programmed.
References:
1.. Harapan H, Itoh N, Yufika A, Coronavirus disease 2019 (COVID-19): A literature review: J Infect Public Health, 2020; 13(5); 667-73
2.. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395(10223); 497-506
3.. Li X, Ma X, Acute respiratory failure in COVID-19: Is it “typical” ARDS?: Crit Care, 2020; 24(1); 1-5
4.. Hu Y, Sun J, Dai Z, Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis: J Clin Virol, 2020; 127(April); 104371
5.. : Rehabilitation considerations during the COVID-19 outbreak, 2020; 1-22, PAHO-WHO
6.. Zeng B, Chen D, Qiu Z, Expert consensus on protocol of rehabilitation for COVID-19 patients using framework and approaches of WHO International Family Classifications: Aging Med, 2020; 3(2); 82-94
7.. Eggmann S, Kindler A, Perren A, Early physical therapist interventions for patients with COVID-19 in the acute care hospital: A case report series: Phys Ther, 2021; 101(1); 1-9
8.. Mrozkowiak M, The concept of rehabilitation treatment after COVID-19 infection: Pedagog Psychol Sport, 2021; 7(1); 11
9.. Thomas P, Baldwin C, Bissett B, Physiotherapy management for COVID-19 in the acute hospital setting: Clinical practice recommendations: J Physiother, 2020; 66(2); 73-82
10.. Burhan E, Susanto AD, Nasution SA: Guidelines for the Management of COVID-19 Edition 3, 2020, Indonesian Society of Internal Medicine Available at: https://www.papdi.or.id/download/983-pedoman-tatalaksana-covid-19-edisi-3-desember-2020
11.. Bagnato S, Boccagni C, Marino G, Critical illness myopathy after COVID-19: Int J Infect Dis, 2020; 99; 276-78
12.. Beom J, Jung J, Hwang I, Cho Y: Early rehabilitation in a critically ill inpatient with COVID-19 December, 2020; 2020; 858-61
13.. Chou W, Lai CC, Cheng KC, Effectiveness of early rehabilitation on patients with chronic obstructive lung disease and acute respiratory failure in intensive care units: A case-control study: Chron Respir Dis, 2019; 16; 1479973118820310
14.. Li J, Rehabilitation management of patients with COVID-19: Lessons learned from the first experience in China: Eur J Phys Rehabil Med, 2020; 56(3); 335-38
15.. Kurtaiş Aytür Y, Pulmonary rehabilitation principles in SARS-COV-2 infection (COVID-19): A guideline for the acute and subacute rehabilitation: Turkish J Phys Med Rehabil, 2020; 66(2); 104-20
16.. Righetti RF, Onoue MA, Politi FVA, Physiotherapy care of patients with coronavirus disease 2019 (COVID-19) – a Brazilian experience: Clinics, 2020; 75; e2017
17.. Lazzeri M, Lanza A, Bellini R, Respiratory physiotherapy in patients with COVID-19 infection in acute setting: A Position Paper of the Italian Association of Respiratory Physiotherapists (ARIR): Monaldi Arch Chest Dis, 2020; 90(1) :monaldi.2020.1285
18.. Candan SA, Elibol N, Abdullahi A, Consideration of prevention and management of long-term consequences of post-acute respiratory distress syndrome in patients with COVID-19: Physiother Theory Pract, 2020; 36(6); 663-68
19.. Vitacca M, Carone M, Clini EM, Joint statement on the role of respiratory rehabilitation in the COVID-19 crisis: The Italian Position Paper: Respiration, 2020; 99(6); 493-99
20.. Brugliera L, Spina A, Castellazzi P, Rehabilitation of COVID-19 patients: J Rehabil Med, 2020; 52(4); jrm00046
21.. Iannaccone S, Castellazzi P, Tettamanti A, Role of rehabilitation department for adult individuals with COVID-19: The Experience of the San Raffaele Hospital of Milan: Arch Phys Med Rehabil, 2020; 101(9); 1656-61
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952107
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952658
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953243
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952989
Most Viewed Current Articles
07 Dec 2021 : Case report
22,640,312
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,831
174,831
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,997
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,925
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133