13 June 2022: Articles 
A 65-Year-Old Woman with an Enlarged Tongue Due to Amyloidosis
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Hani H. Mawardi1ABDEF*, Sara K. Akeel1BDEF, Sarah Alfarabi AliDOI: 10.12659/AJCR.936192
Am J Case Rep 2022; 23:e936192






Abstract
BACKGROUND: Amyloidosis is a clinical condition characterized by the extracellular deposition of insoluble, abnormal amyloid fibrils in various body tissues. It is generally categorized into 2 forms – localized and systemic – with a wide range of signs and symptoms. This case report discusses the localized amyloidosis involvement of the oral cavity and its treatment.
CASE REPORT: A 65-year-old woman presented to the oral medicine clinic reporting painless tongue enlargement, which has been slowly progressing over several years, leading to difficulty in tongue movement, eating, and swallowing. Extra-oral examination showed a prominent lower lip with rubbery consistency. Intra-oral examination revealed a significantly enlarged tongue almost filling the whole oral cavity with dental indentations evident on all tongue surfaces and multiple, deep ulcerative craters of various sizes ranging from 2 to 5 mm in diameter. Histopathological examination under light microscope using hematoxylin and eosinophil and Congo red stain were diagnostic for amyloidosis. Further investigation with the Rheumatology Department, including renal and liver function tests, as well as echocardiography, were conducted and ruled out systemic involvement of other body organs. The patient was treated with weekly intra-lesional triamcinolone injections, with significant improvement.
CONCLUSIONS: We report a rare case of localized amyloidosis presenting as macroglossia. Although the most effective management in tongue amyloidosis is surgical resection, conservative management in cases of localized oral amyloidosis presenting as macroglossia with weekly intra-lesional triamcinolone injections can be an effective approach, providing patients with better quality of life. Future studies exploring treatment modalities for similar cases with limited oral involvement are warranted.
Keywords: Amyloid, Amyloidosis, Macroglossia, Aged, Female, Humans, Quality of Life, Tongue, Triamcinolone
Background
Amyloidosis is a clinical condition characterized by the extracellular deposition of insoluble, abnormal amyloid fibrils in body tissues [1]. Consequently, these deposits can progressively replace natural tissues and alter the affected organ structure and function, depending on disease stage and severity [2]. Amyloidosis can present as 1 of 4 types: primary, secondary, familial, and senile amyloidosis. Primary type (AL) involves the light chain and it is caused by plasma cell dyscrasias, potentially affecting multiple organs. Secondary type (AA) involves protein A circulating throughout the body, mainly affecting the kidneys and liver. Familial type (ATTR) can present as a result of mutation in transthyretin (TTR), and it mainly involves the liver and nervous system. Senile type (ATTRwt) is known as TTR wild-type and it usually affects the heart [2]. The incidence of amyloidosis varies based on geographical location. For instance, the reported incidence in the UK was around 500 new cases annually, with an estimated 0.5–1.0 deaths/100 patients [3]. The reported incidence in the Danish population was 3.56 per 100 000 person-years [4]. Amyloidosis can be hereditary in origin or acquired as a complication of a primary disease with unclear patho-physiology [2]. Based on the extent of the disease, management can include corticosteroids, chemotherapy, laser ablation, and/or surgical resection, with the aim of providing supportive measures and controlling the patient’s symptoms, as no cure is currently available [5].
In general, amyloidosis can be localized, where it affects a particular organ such as the skin or oral cavity, whereas it is considered systemic when involving several body tissues such as viscera, blood vessel walls, and connective tissues [2]. Primary amyloidosis is a condition in which macroglossia with dental indentation can present as an clinical finding [6]. Other clinical features include yellowish plaques or nodules distributed in the oral cavity [6]. However, it can also be a localized disease with no involvement of other organs [6]. Other sites with possible localized involvement include the skin and respiratory and urogenital tracts [2]. In these clinical situations, full body investigations are needed to rule out systemic involvement. Overall, diagnosis of amyloidosis relies on clinical evaluation combined with pathological examination using Congo red staining under crossed polarized light [2].
This report describes a case of amyloidosis localized only to the tongue, resulting in macroglossia significantly impacting the patient’s quality of life. The proposed treatment and case management are discussed in this case report.
Case Report
A 65-year-old woman presented to the Oral Medicine Clinic reporting painless tongue enlargement that started several years ago and had been slowly progressing, leading to difficulty in tongue movement, eating, and swallowing. A few weeks before her visit, she started experiencing painful ulcerations in the tongue lasting 4–5 days, which further complicated her daily routine. The patient’s medical history was significant for hyper-tension, for which she was receiving an angiotensin-converting enzyme (ACE) inhibitor. The patient had no known allergies and had never smoked. Extra-oral examination showed a prominent lower lip with rubbery consistency. Intra-oral examination revealed a significantly enlarged tongue almost filling the whole oral cavity, with dental indentations evident on all tongue surfaces and multiple, deep ulcerative craters of various sizes ranging from 2 to 5 mm in diameter (Figure 1). Upon palpation, all oral tissues, including the labial mucosa, were firm with thick and rubbery consistency. Histopathological examination of tissue obtained from the mid-dorsal tongue revealed normal surface epithelium with underlying connective tissue showing eosinophilic deposits of globular amorphous material in the lamina propria with hematoxylin and eosin (H&E) staining (Figure 2). Congo red staining of the specimen showed vascular connective tissue with orange-red deposits in the lamina propria under normal light and areas of apple-green birefringence of the amyloid deposits under polarized light, which is diagnostic for amyloidosis.
Consultation with the Rheumatology Service was requested to confirm the localized deposition of amyloid material only in the oral cavity without other body organ involvement. Part of the patient workup, renal and liver function tests, as well as echocardiogram and cardiac enzymes, were carried out and all were within normal limit. Due to the patient’s age and potential medical co-morbidities and risk of mortality, surgical intervention was excluded as a treatment option per patient preference. The patient was managed with series of intra-lesional triamcinolone injections every 2 weeks over 6 months, without any complications (Figure 3). Thereafter, an acceptable reduction in tongue size and restoration of function was noted.
Discussion
Amyloidosis is a general diagnosis with various forms, including localized (eg, brain in Alzheimer disease, genito-urinary tract, or skin) and systemic involvement (eg, light chain and amyloid A protein deposits in multiple organs) [2]. In general, localized amyloidosis tends to be non-life-threatening in nature, and more likely to be driven by immunoglobulin light chain amyloidosis (AL) deposition [7–9]. Based on the affected organs and severity, amyloidosis signs and symptoms vary and can include edema, fatigue, weight loss, nephropathy, cardiomegaly or interstitial pulmonary edema [2]. Due to the lack of specific blood test or radiography, diagnosis of amyloidosis can often be challenging and is based entirely on clinical findings [2].
Macroglossia is defined as a long-term, painless enlargement of the tongue, in which it extends beyond the alveolar ridge or crest at resting position [10]. It can be classified as either true macroglossia as in acromegaly or relative as in Down’s syndrome relative to the size of other oral structures [10]. Slowly progressive macroglossia can be an early sign of systemic amyloidosis (25%), and it is the only site involved in 9% of all amyloidosis cases [11]. It typically manifests as an enlarged tongue with a rubbery-hard consistency and limited mobility. Other clinical findings of oral amyloidosis can include yellow-white nodules, purple bulla-like masses, ecchymosis, and/or white patch-like lesions [12]. In some cases, tongue enlargement is overlooked by clinicians, unless reported by the patient, and can be associated with difficulty in performing regular daily functions of eating and speaking. Histopathological examination of biopsied tissues is usually diagnostic when examined with Congo red stain under polarizing light demonstrating the fibril deposits as apple-green birefringence [13]. Once identified, complete body screening for amyloid should be conducted via immunofixation of serum and urine to measure monoclonal immunoglobulin levels combined with free light-chain assay [2]. At present, the optimal management of amyloidosis is still unclear [2]. However, localized cases in the oral cavity may not require systemic therapy and can be managed with local agents such as serial intra-lesional steroid injections. More advanced cases with minimal or no response to localized treatment may require surgical intervention to debulk the tongue and improve the quality of life [14].
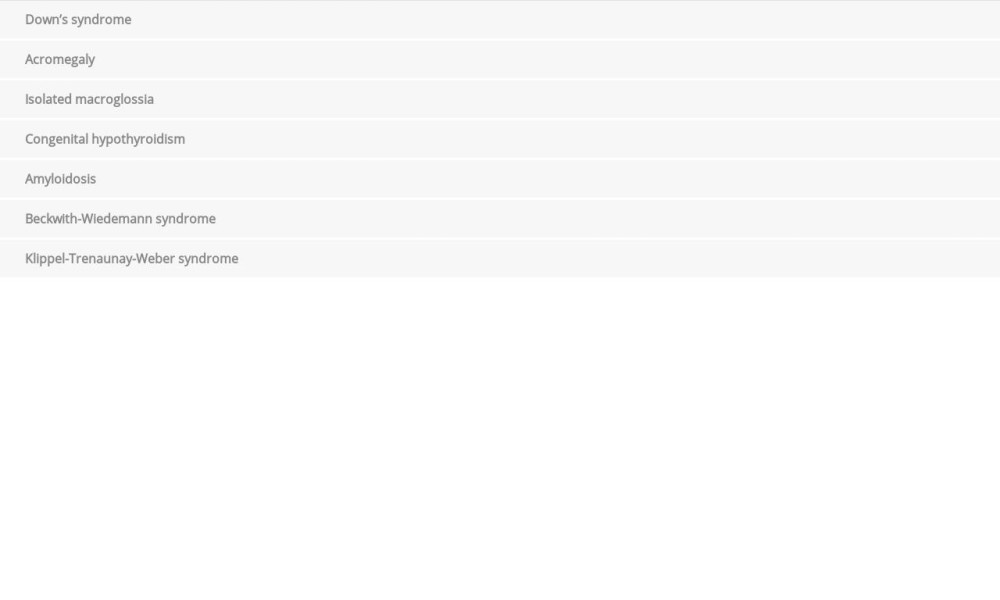
Differential diagnosis of macroglossia include, in addition to amyloidosis, Down’s syndrome and acromegaly (Table 1). Down’s syndrome is the most common genomic condition, affecting 1 of every 787 babies born in the US and is caused by trisomy sapiens chromosome 21 [15]. It is associated with intellectual disability in addition to other medical disorders such as congenital heart disease, celiac disease, and endocrinopathies (eg, short status, diabetes, and thyroid dysfunction) [16]. In the head and neck area, Down’s syndrome patients may present with muscular hypotonia, gothic palate, malocclusion, and false macroglossia [15]. Our patient had no intellectual disability or features suggestive of Down’s syndrome. Furthermore, she had true macroglossia with clear dental indentations. Acromegaly, another differential diagnosis to consider, is a rare condition characterized by somatic overgrowth combined with physical disfigurement as a result of growth hormone overproduction [17]. Common clinical features include soft tissue swelling, arthralgia, hypertension, hyperglycemia, and hyperhidrosis [17]. In the cranio-facial region, acromegaly patients can present with jaw prognathism, thickening of the lips, and pronounced brow protrusion, as well as malocclusion, dental spacing, and macroglossia [17]. In our patient, none of these features were evident. Beckwith-Wiedemann syndrome is a congenital syndrome, which is considered the most common cause of over-growth in infants [18]. Clinical features include abdominal wall defects, exomphalos, umbilical hernia, ear creases or pits, macrosomia, and macroglossia [18]. Other than macroglossia, none of the other features were noted in the current case. Other conditions to consider which include isolated macroglossia are a rare autosomal dominant condition, Klippel-Trenaunay-Weber syndrome and congenital hypothyroidism (Table 1) [10].
Histologically, the deposition of the eosinophilic acellular amorphous material is characteristic for amyloid deposit, which can be confirmed with Congo red or other stains such as Crystal violet or Thioflavin T, examined under florescence microscopy [2]. Fibrin can also show the same deposits with plasminogen deficiency [19]. In this rare disease, fibrin deposits in the conjunctiva and/or the gingiva can result in destructive changes in the tissues[19]. For such cases, special stains should be used for better differentiation among types [19]. Excessive hyalinized collagen deposits seen in hyaline fibromatosis syndrome may have a similar histological presentation [20]. It is a rare autosomal disease with genetic mutation of ANTXR2. It is usually seen in childhood, commonly as gingival enlargement and sometimes with skin lesions [20]. Another rare disease in children is lipid proteinosis, which is an inherited autosomal disease characterized by mutation in the extracellular matrix gene and commonly affecting the vocal cords and larynx [20]. Other conditions such as scleroderma and submucous fibrosis can have similar features microscopically, with differences in clinical presentation [20]. Clinical and radiographic correlations are necessary in such cases to reach the proper diagnosis.
The reported case represents localized amyloidosis in the form of macroglossia with significant impact on patient’s quality of life. The tongue ulceration noted in this case was more likely to be related to trauma with function, which increased the patient’s discomfort. Based on the current literature, the treatment of choice for localized amyloidosis is surgical resection/ excision, but observation can be an option in mild cases [2,20]. This option in general is associated with several morbidities such infection, bleeding, and post-surgical loss of function [2]. Considering the low prevalence of tongue involvement with amyloidosis, no consensus on the best treatment options for similar cases is available. Most of the proposed surgical resection options are merely dependent on case reports and small case series [21]. In addition, localized cutaneous amyloidosis was reported to be treated with various approaches, including steroids use [22]. This case was managed with a conservative approach based on the patient’s preference, and she was willing to experiment with different approaches. The application of intra-lesional steroid injections is generally accepted as a safe and simple treatment option with documented positive outcome [23–25]. In addition, anticipated complications are limited to pain and minimal bleeding afterward [23].
Although localized cases can recur following treatment, they are less likely to progress to more systemic involvement [11]. In general, the overall prognosis of oral amyloidosis is good, unless it is associated with systemic involvement, which can lead to a poor prognosis, with a median survival of 2 years. In particular, multiple myeloma combined with amyloidosis accounts for 6–15% of all cases [26]. These have variable prognosis, based on the multiple myeloma status [26]. Other systemic conditions that may be associated with amyloidosis include tuberculosis, rheumatoid arthritis, Crohn’s disease, and Hodgkin’s lymphoma. All these conditions can have an impact on disease prognosis and have to be ruled out as part of the patient’s work-up [2].
Conclusions
We have reported the case of a patient with localized amyloid deposition presenting as macroglossia with no involvement of other body organs. Non-invasive management with weekly intra-lesional triamcinolone injections were effective in reducing the tongue size and providing the patient with better quality of life. Future studies to explore other treatment modalities for similar cases with limited involvement are warranted.
Figures
References:
1.. D’Aguanno V, Ralli M, Artico M, Systemic amyloidosis: A contemporary overview: Clin Rev Allergy Immunol, 2020; 59(3); 304-22
2.. Bustamante JG, Zaidi SRH: Amyloidosis, 2021, Treasure Island (FL), StatPearls
3.. Pepys MB, Pathogenesis, diagnosis and treatment of systemic amyloidosis: Philos Trans R Soc Lond B Biol Sci, 2001; 356(1406); 203-10 ; discussion 210–11
4.. Westin O, Butt JH, Gustafsson F, Two Decades of cardiac amyloidosis: A Danish Nationwide Study: JACC CardioOncol, 2021; 3(4); 522-33
5.. Cohen OC, Wechalekar AD, Systemic amyloidosis: moving into the spotlight: Leukemia, 2020; 34(5); 1215-28
6.. Mishra K, Jandial A, Prakash G, Malhotra P, Macroglossia and amyloidosis: QJM, 2018; 111(11); 835-36
7.. Dhatt R, Walstra F, Munk P, Ng T, Mallinson P, Localized plantar amyloidosis: Case report and review of the literature: Skeletal Radiol, 2021; 50(7); 1467-72
8.. Harris G, Lachmann H, Hawkins P, Sandhu G, One hundred cases of localized laryngeal amyloidosis – evidence for future management: Laryngoscope, 2021; 131(6); E1912-17
9.. Lin XY, Pan D, Sang LX, Chang B, Primary localized gastric amyloidosis: A scoping review of the literature from clinical presentations to prognosis: World J Gastroenterol, 2021; 27(12); 1132-48
10.. Kutti Sridharan G, Rokkam VR: Macroglossia, 2021, Treasure Island (FL), StatPearls
11.. Deng J, Chen Q, Ji P, Oral amyloidosis: A strategy to differentiate systemic amyloidosis involving the oral cavity and localized amyloidosis: Oral Dis, 2019; 25(3); 670-75
12.. Stoopler ET, Sollecito TP, Chen SY, Amyloid deposition in the oral cavity: A retrospective study and review of the literature: Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2003; 95(6); 674-80
13.. Mollee P, Renaut P, Gottlieb D, Goodman H, How to diagnose amyloidosis: Intern Med J, 2014; 44(1); 7-17
14.. McCrossan S, Martin S, Hill C, Tongue reduction for macroglossia: J Craniofac Surg, 2021; 32(5); 1856-59
15.. Vicente A, Bravo-Gonzalez LA, Lopez-Romero A, Craniofacial morphology in down syndrome: A systematic review and meta-analysis: Sci Rep, 2020; 10(1); 19895
16.. Kaczorowska N, Kaczorowski K, Laskowska J, Mikulewicz M, Down syndrome as a cause of abnormalities in the craniofacial region: A systematic literature review: Adv Clin Exp Med, 2019; 28(11); 1587-92
17.. Vilar L, Vilar CF, Lyra R, Lyra R, Naves LA, Acromegaly: Clinical features at diagnosis: Pituitary, 2017; 20(1); 22-32
18.. Sequera-Ramos L, Duffy KA, Fiadjoe JE, The prevalence of difficult airway in children with Beckwith-Wiedemann syndrome: A retrospective cohort study: Anesth Analg, 2021; 133(6); 1559-67
19.. Sivolella S, De Biagi M, Sartori MT, Destructive membranous periodontal disease (ligneous gingivitis): A literature review: J Periodontol, 2012; 83(4); 465-76
20.. Rodrigues-Fernandes CI, de Caceres CBL, Sant’Ana MSP, Oral lesions containing amyloid-like material: Oral Surg Oral Med Oral Pathol Oral Radiol, 2021; 132(2); 190-201
21.. O’Reilly A, D’Souza A, Lust J, Price D, Localized tongue amyloidosis: A single institutional case series: Otolaryngol Head Neck Surg, 2013; 149(2); 240-44
22.. Weidner T, Illing T, Elsner P, Primary localized cutaneous amyloidosis: A systematic treatment review: Am J Clin Dermatol, 2017; 18(5); 629-42
23.. Figueroa AA, Murphy J, Tragos C, Intra-lesional injection of triamcinolone to palatoplasty scar to aid reversal of transverse maxillary relapse after orthognathic surgery: J Craniofac Surg; 2021 [Online ahead of print]
24.. Porter D, Burton JL, A comparison of intra-lesional triamcinolone hexacetonide and triamcinolone acetonide in alopecia areata: Br J Dermatol, 1971; 85(3); 272-73
25.. Cramer JE, Intra-lesional injection of triamcinolone: Aust J Dermatol, 1964; 7; 140-47
26.. Acevedo J, Doros G, Szalat R, Sanchorawala V, Clinical characteristics, treatment regimens, and survival in elderly patients with AL amyloidosis: Clin Lymphoma Myeloma Leuk, 2021; 21(6); 425-26
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133