27 July 2022: Articles 
Fatal Sequelae of Reperfusion Injury in Postoperative Gastric Bypass
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment
Zachary J. Naser1ABEF, Karleigh R. Curfman1ABEF*, Meaghan M. Marley1ABEF, D'Arcy N. Duke1ABEFDOI: 10.12659/AJCR.936270
Am J Case Rep 2022; 23:e936270






Abstract
BACKGROUND: Obesity is a pandemic that is currently uncontrolled. In the surgical population, bariatric surgery is a sustainable and attractive option. However, both obesity and surgery can independently increase the risk for venous thromboembolism and subsequent significant and even fatal adverse effects.
CASE REPORT: We present the unique case of a 63-year-old woman who developed substantial venous thrombosis in the postoperative period following a laparoscopic hiatal hernia repair and Roux-en-Y gastric bypass. Venous thrombosis following surgery is a known possible complication, but we felt that this case required reporting due to the extreme extent of thrombosis and the significant course of events that occurred following her readmission. Due to the increased thrombus burden, the patient developed phlegmasia cerulea dolens and required operative thrombectomy. With restoration of blood flow following the procedure, the patient’s clinical status rapidly declined, likely due to reperfusion injury. Ultimately, she developed multisystem organ failure, which included the constellation of shock, hypoxic respiratory failure, acute renal failure, shock liver, and, finally, cardiopulmonary arrest.
CONCLUSIONS: As the authors of this paper, we were especially inclined to report this particular case as the patient’s clinical course was exceedingly complex due to her presenting phlegmasia cerulea dolens. The course was further complicated postoperatively by the detrimental sequelae of massive reperfusion injury, which likely eventually led to her death. We felt this pertinent to present because, after an extensive PubMed literature review, this sequence of events following gastric bypass surgery has yet to be reported in the literature.
Keywords: Abdominal Obesity Metabolic Syndrome, Gastric Bypass, venous thromboembolism, Female, Humans, Middle Aged, Obesity, Postoperative Period, Venous Thrombosis
Background
Obesity is a pandemic that is ravaging through the global population, and it is worst in the United States of America (USA) [1]. Among high-income countries, the USA has the highest mean body mass index (BMI) for both men and women, and over two-thirds of adults in the USA over the age of 20 are over-weight or obese; with obesity affecting 93.3 million Americans (39.8%) [1,2]. The increasing BMI is also associated with increasing risk for morbidities and mortality, and roughly 20% of deaths in the USA annually are associated with obesity [2]. Despite the surging prevalence of obesity, the ability of most treatments to provide effective and sustainable results is low [1]. Surgical procedures, however, have been able to provide an option for successful long-term results in addition to providing benefits regarding obesity-related comorbidities, and reduce the risk of death [1]. Therefore, there has been increasing demand for bariatric surgery, especially in the USA, where approximately 256 000 bariatric surgeries are performed annually [3].
Although bariatric surgery has become popular and can provide substantial results, it is important to understand that these major procedures are not without consequences and postoperative complications are common. A wide variety of complications have been frequently associated with bariatric surgery, mainly including postoperative bleeding, wound infection, venous thromboembolism (VTE), and urinary tract infection (UTI) [4]. These complications alone can be severe, but they are also associated with significant additional consequences such as reoperation, intensive care unit admission, hospital readmission, end-organ dysfunction, and death [4]. Of these complications, VTE and its own constellation of associated complications are pertinent to report within this review. It has been reported that bariatric surgery patients have an even higher risk of VTE development than their non-bariatric surgical counterparts [5]. This increase is believed to be related to 2 different sources: elevated VTE risks that accompany obesity and its comorbidities, as well as risks associated with the demanding and often difficult bariatric surgery [5]. Given this, we present the case of a bariatric patient whose postoperative course was complicated by massive VTE and subsequent reperfusion injury. Due to her tumultuous and complex course from her complications, she eventually died due to the disease. Our extensive literature search was unable to find any other similar reports of postoperative bariatric patients that developed such destructive VTE and overwhelming reperfusion injury, and therefore felt that this case was pertinent to report.
Case Report
Our patient was a 63-year-old woman with history of a transient ischemic attack, reflux, hypertension, and hyperlipidemia who had previously undergone successful laparoscopic sleeve gastrectomy. She had no significant reported family history and her regular medications only included vitamin supplements. Initially, she had experienced weight loss, but over the ensuing years had gained weight and was following with our institution’s bariatric institute. Recently, she developed worsening gastroesophageal reflux disease (GERD) symptoms and underwent esophagogastroduodenoscopy, pertinent for a large hiatal hernia. Given her weight gain, GERD symptoms, and hiatal hernia, she was moved to the operating room (OR) for a laparoscopic hand-assisted hiatal hernia repair and conversion of her sleeve gastrectomy to a Roux-en-Y gastric bypass (RYGB). The procedure was technically difficult due to vast adhesive disease, but was otherwise uncomplicated. Her inpatient postoperative course was uneventful and she was discharged home in stable condition on postoperative day (POD) 4. She followed up at our outpatient bariatric institute on POD 8, and was found to be progressing appropriately.
However, she came to the Emergency Department (ED) on POD 18 after having shortness of breath, left lower leg pain, and swelling, which were limiting her ambulation. Upon ED arrival, she became hypotensive and unresponsive and subsequently developed cardiopulmonary arrest, underwent cardiopulmonary resuscitation until return of spontaneous circulation, was intubated with rapid sequence intubation, and admitted to the care of the Intensive Care Unit (ICU) team. She was found to be extremely acidotic at presentation (pH 7.19, bicarbonate 10, lactic acid 17, base excess −16.4), and had signs of acute hypoxic respiratory and renal failure (Table 1). Due to her presentation, she underwent computed tomography (CT) imaging, inclusive of pulmonary embolism protocol, which was negative for abnormalities aside from enlarged left common iliac, external iliac, and common femoral veins with associated edema of the left thigh. Upon ICU transfer, the general surgery team was consulted due to her recent procedure. On physical examination, the left leg had substantial swelling, purple discol-oration, and was cold to touch. Therapeutic anticoagulation was started and vascular surgery was immediately contacted due to concerns of phlegmasia cerulea dolens (PCD). As the patient’s clinical status was not improving and without other identifiable causes, she was taken to the OR on anticoagulation for a combined diagnostic laparoscopy and lower-extremity venogram. Diagnostic laparoscopy was first performed, which showed pink viable bowel and no identified abnormalities. A venogram was then performed via an 8-French catheter through the left popliteal vein, showing extensive, acute, nearly occlusive left iliac (Figure 1) and femoral (Figure 2) venous thrombosis from the iliac confluence to the distal femoral vein just proximal to the popliteal vein. A clot retrieval system was used to perform the thrombectomy, and after passage of the device 7 times, all appreciable acute thrombus was believed to be removed on completion venogram. However, following surgery, her clinical status rapidly deteriorated; she developed multisystem organ failure, shock liver, respiratory failure, and disseminated intravascular coagulation, required increasing vasopressor support. She continued to have significant acidosis, and continuous renal replacement therapy was started due to her worsening renal failure (Table 1). On POD 1, the patient was noted to have a tense left lower extremity, with bullous formation of the skin overlying the thigh and calf, mottled digits, and no identifiable pulses or Doppler signals. Due to suspicion of compartment syndrome, she was returned to the OR and underwent a 4-compartment calf fasciotomy, where the muscle appeared viable and without abnormality. As the patient’s thigh was also tense, a fasciotomy was performed, which revealed copious brown fluid, and pale, unresponsive muscle, concerning for tissue death. After the operation, she was transferred back to the ICU, but several hours later she again had cardio-pulmonary arrest. Resuscitation was attempted, but she eventually died due to her disease process.
Discussion
Obesity is a disease that is extremely prevalent in our current society. The USA has the highest rates of obesity among high-income countries, with the majority of the adult population being overweight or obese [1]. Due to the sustainability of weight loss following surgery, bariatric procedures have become an enticing option to those for whom alternative weight loss measures have failed. However, despite the remarkable appeal and often outstanding results associated with surgical weight loss procedures, these operations are not exempt from serious consequences. Our patient likely died from multisystem organ failure related to injury from her post-bariatric surgery VTE and subsequent reperfusion injury. Although this is an exceedingly rare case of a post-bariatric surgery complication, awareness is encouraged for other postoperative bariatric complications, which are much more common. A meta-analysis performed by Chang et al included over 161 000 patients who underwent bariatric surgery and reviewed rates of complications such as bleeding, stoma stenosis, leak, vomiting, reflux, gastrointestinal symptoms, and nutritional and electrolyte abnormalities [1]. They found that 17% of patients in randomized control trials and 10% of patients in observational studies developed complications related to their bariatric surgery, with the highest rate occurring in gastric bypass procedures [1]. An additional report of postoperative bariatric complications consisting of bleeding, VTE, leak, wound infection, pneumonia, UTI, myocardial infarction, and stroke, as well as their impacts (end-organ dysfunction, reoperation, ICU admission, readmission, and mortality), was reviewed [4]. They found that the most common postoperative complications were bleeding (0.7%), wound infection (0.5%), UTI (0.3%), VTE (0.3%), and anastomotic leak (0.2%) [4]. They also concluded that VTE was the complication with the greatest impact on re-admission rates and mortality, bleeding had the greatest effect on ICU admission and reoperation, and leakage had the greatest influence on end-organ dysfunction [4]. Furthermore, additional evidence of the seriousness of complications was recently published, which again showed an overall postoperative complication rate of 16% [6]. Subsequent data from this study showed that postoperative bleeding was the most common complication, at an increased rate of 2.5%, and identified other similar significant complications, including anastomotic leak, stenosis, internal hernia, VTE, bowel strangulation, sepsis, and death [6].
VTE is a known postoperative complication of many surgeries, and has been proven to have deleterious consequences in patients undergoing bariatric procedures, as illustrated by the present case [4]. In bariatric surgery, there are 2 proposed risks for VTE development [5] due to the association with obesity and the increased technical difficulty of the cases [5]. Obesity is related to many procoagulable states, such as decreased mobility, hypertension, diabetes mellitus, obstructive sleep apnea, venous stasis, and chronic inflammation [5]. Additionally, these difficult procedures have been linked to increased risk of VTE due to longer operative times, endothelial damage from anastomoses, complications, concomitant conditions (such as hernia repair), and extended immobility [5]. Therefore, in post-bariatric surgery, the occurrence of VTE is 0.3–5.4% [3]. Most importantly, roughly 80% of these VTE appear after discharge, and in those with post-discharge VTE, the mortality rate increases by 28-fold, from 0.09% to 2.6% [5].
The development of VTE after bariatric surgery is especially applicable in our patient, as it likely occurred after discharge from the hospital; without VTE formation, she would not have developed PCD and experienced reperfusion injury with its damaging associated sequelae. Reperfusion injury has been defined as paradoxical exacerbation of cellular dys-function and death following the restoration of blood flood to previously ischemic tissue [7]. Although blood flow is necessary to provide oxygen to tissues, return of oxygen to previously ischemic tissue is associated with detrimental results. Restoration of blood flow results in creation of superoxide anions and hydrogen peroxide, which encourages hydroxyl radical formation, promotes release of inflammatory mediators, disrupts cell permeability, and leads to cell death [7]. In addition, prolonged ischemia causes stasis and wedging of red blood cells, resulting in stacking that damages the endothelial surfaces [8]. Furthermore, intraluminal platelets in venules induce a thrombotic cascade, leukocytes occlude capillary lu-mens, and increased permeability results in edema and hemo-concentration [8]. The combination of all of these factors, in addition to external compression from edema, results in the “no-reflow phenomenon”, which is malperfusion and permanent vessel closure despite adequate revascularization [8]. Moreover, reperfusion can lead to a diffuse inflammatory response when inflammatory mediators are released, resulting in extravascular third spacing and development of compartment syndrome [8]. The effects of reperfusion can also be seen systemically. The lungs and cardiovascular system are most commonly affected by reperfusion-induced multisystem organ failure, and cause 30–40% of associated ICU mortality related to this pathology [8]. It is believed that the inflammatory mediators activate endothelial cells in remote organs resulting in hypotension and hypovolemia by means of increased circulation of degradation products, activation of the clotting cascade, vascular luminal occlusion, and diffuse vascular permeability [8]. There is a paucity of literature on the appropriate management strategy for PCD and the subsequent reper-fusion syndrome that can occur. Some recommendations for management have included algorithms based on physical examination features like cyanosis, blistering, gangrene, sensorimotor dysfunction, or pulselessness in conjunction with the time since symptom onset [8]. From this assessment, recommendations include anticoagulation along with either mechanical thrombectomy or amputation, depending on the severity of the PCD and risk of reperfusion injury [8].
Conclusions
Our patient underwent bariatric surgery and developed significant venous thrombus as an outpatient. This rapidly progressed to phlegmasia cerulea dolens, which necessitated several operations. Although excellent restoration of blood flow was achieved, an uncontrollable reperfusion injury occurred, which led to advanced systemic alterations and likely caused her death. To the best of our knowledge, this is the first time this constellation of events has occurred following bariatric surgery. As evidenced by the data reviewed in this paper, obesity rates are increasing, which can increase the risk for VTE formation, as does undergoing bariatric surgery. Although this is the only identified suspected case of fatal reperfusion injury after bariatric surgery, weight reduction surgery is becoming more common and the majority of post-bariatric VTE occur after the patient is discharged. Therefore, we caution practitioners that this entity may be underdiagnosed and may increase in frequency. Due to the extreme severity of this pathology and the popularity of bariatric surgery, we implore physicians to be cognizant of the associated VTE risks and to have a heightened suspicion in this clinical setting. Acknowledging the paucity of confirmed management guidelines, early recognition and intervention appear to be essential, as adequate reperfusion can be both limb- and life-saving.
Figures
References:
1.. Chang S, Stoll C, Song J, Bariatric surgery: An updated systematic review and meta-analysis, 2003–2012: JAMA Surg, 2014; 149(3); 275-87
2.. Gerardo de Cosio F, Diaz-Apodaca B, Baker A, US obesity mortality trends and associated noncommunicable diseases contributing conditions among white, black, and hispanic individuals by age from 1999 to 2017: SN Compr Clin Med, 2021; 2021(3); 1334-43
3.. , Estimate of bariatric surgery numbers, 2011–2019, 2021, ASMBS Cited 5/17/22. Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers
4.. Daigle C, Brethauer S, Tu C, Which postoperative complications matter most after bariatric surgery? Prioritizing quality improvement efforts to improve national outcomes: Surg Obes Relat Dis, 2018; 14(5); 652-57
5.. El Ansari W, Sathian B, El-Menyar A, Venous thromboembolic events after bariatric surgery: Protocol for a systemic review and meta-analysis: Int J Surg Protoc, 2020; 2020(22); 10-14
6.. Coblijn U, Karres J, de Raaff C, Predicting postoperative complications after bariatric surgery: The Bariatric Surgery Index for Complications, BASIC: Surg Endosc, 2017; 31(11); 4438-45
7.. Cowled P, Filtridge R: Pathophysiology of reperfusion injury. Mechanisms of vascular disease: A reference book for vascular specialists, 2011, Adelaide (AU), University of Adelaide Press
8.. Lessne ML, Bajwa B, Hong K, Fatal reperfusion injury after thrombolysis for phlegmasia cerulea dolens: J Vasc Interv Radiol, 2012; 23(5); 681-86
Figures
Tables
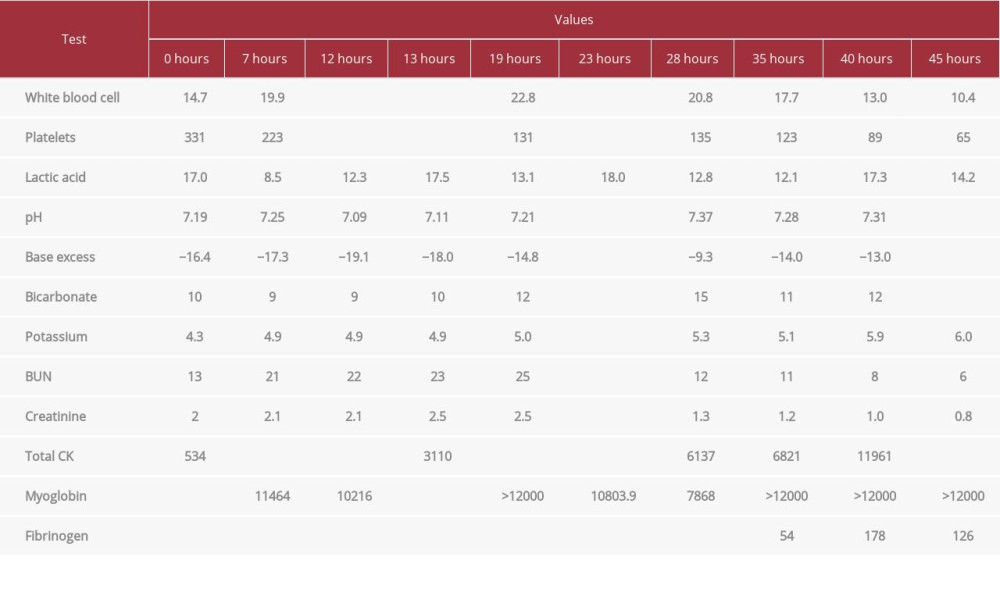 Table 1.. Trend of laboratory values over the hospital course.Representation of patient’s laboratory values over the course of the hospital stay, displaying her acidosis, renal disease, electrolyte imbalance, and rhabdomyolysis.Table 1.. Trend of laboratory values over the hospital course.Representation of patient’s laboratory values over the course of the hospital stay, displaying her acidosis, renal disease, electrolyte imbalance, and rhabdomyolysis.
Table 1.. Trend of laboratory values over the hospital course.Representation of patient’s laboratory values over the course of the hospital stay, displaying her acidosis, renal disease, electrolyte imbalance, and rhabdomyolysis.Table 1.. Trend of laboratory values over the hospital course.Representation of patient’s laboratory values over the course of the hospital stay, displaying her acidosis, renal disease, electrolyte imbalance, and rhabdomyolysis. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133