18 June 2022: Articles 
A Rare Case of Combined Choriocarcinoma and Placental Site Trophoblastic Tumor Presenting as Skin Lesion: A Case Report
Unusual clinical course, Challenging differential diagnosis
Tulika Chatterjee1EF*, Annia Martial1EF, Sahitya Settypalli2E, Larry Lindahl3EFDOI: 10.12659/AJCR.936451
Am J Case Rep 2022; 23:e936451






Abstract
BACKGROUND: Despite the tendency to metastasize widely, Gestational Trophoblastic Neoplasia (GTN) is one of the most curable solid tumors with chemotherapy.
CASE REPORT: A 41-year-old female, G4P2A2, presented with a slowly growing lump on the left side of the scalp associated with a headache. The patient had intermittent, sharp left eye pain which radiated to the side of her face, photophobia, early morning blurring of vision, and nausea. Palpation over scalp lesion produced deep retro-orbital pain and pain was exacerbated with bending over. An ophthalmological evaluation was unremarkable. Ultrasonography (USG) of the left scalp showed an intramuscular mass superficial to the left frontal bone. During excision biopsy, the mass was found to be invading the frontal bone. Histopathology showed a metastatic trophoblastic tumor with mixed features of choriocarcinoma and placental site trophoblastic tumor. A pregnancy test was positive, the beta HCG level was elevated but USG did not show intrauterine pregnancy. CT head demonstrated an intracranial, dural-based mass that extended against the brain but did not breach the pial membrane. CT chest, abdomen, pelvis, and PET scan showed no evidence of metastatic disease. She was successfully treated with resection of the transcranial lesion followed by aggressive chemotherapy – Etoposide, Methotrexate, Actinomycin-D, Vincristine, and Cyclophosphamide.
CONCLUSIONS: This was an unusual case of GTN due to its primary presentation as skin metastasis, without any lung metastasis and no identifiable primary lesion. It is also very unusual to see a combination of choriocarcinoma and placental site trophoblastic tumor cells in the same tumor mass.
Keywords: Choriocarcinoma, gestational trophoblastic disease, Neoplasm Metastasis, Trophoblastic Tumor, Placental Site, Adult, Antineoplastic Combined Chemotherapy Protocols, Cyclophosphamide, Etoposide, Female, Humans, Methotrexate, Pain, Placenta, Pregnancy, Uterine Neoplasms, Vincristine
Background
Gestational trophoblastic neoplasia (GTN), especially chorio-carcinoma is an aggressive neoplasm arising out of the uterine body with a very high propensity for metastasis [1]. Fortunately, it is also very susceptible to chemotherapy with cure rates of more than 90%, even in high-risk patients with the presence of widespread metastases [2]. It was the first medically cured solid cancer in 1956 [3]. The lungs, liver, and central nervous system are the most frequent organs that GTN metastasizes to. GTN can have a variety of presentations, but it is rare for it to metastasize to the skin. We present a rare case of GTN with primary presentation as skin metastasis, without any lung metastasis and no identifiable primary lesion. This case was also very unusual as histopathology showed a combination of choriocarcinoma and placental site trophoblastic tumor cells in the same tumor mass.
Case Report
A 41-year-old female presented to the outpatient clinic with a chief complaint of headache with left eye pain, ongoing for a duration of 2 weeks. She also complained of a growing “lump” on the left side of her scalp which on palpation caused pain “deep in the eye” and it radiated to the side of her face. The headaches were worse in the morning, associated with nausea and intermittent episodes of vomiting. She had noticed a blurring of vision in the morning to the extent that she was not able to read the wall clock. She normally did not wear corrective eyeglasses. The headache worsened when she bent over. She denied any fever, chills, or weight loss. Prominent physical examination findings were a left-sided scalp swelling of approximately 3 cm diameter, photophobia, and blurring of vision in the left eye. Deep retro-orbital pain could be reproduced by palpation on the left temporal region scalp mass. Complete blood count and erythrocyte sedimentation rate were within normal limits and C-reactive protein was mildly elevated at 0.90 mg/dl. An urgent ophthalmological evaluation was normal. Ultrasound of the mass showed soft tissue mass lying immediately superficial to the frontal bone measuring 3.5×3.0×0.6 cm with diffuse internal blood flow.
An excisional biopsy was planned and intraoperatively, it was found that the scalp mass was deeper than subcutaneous tissue and extended to the frontal bone itself with some osseous invasion. The extracranial mass was completely excised and during excision, extensive hemorrhage from the mass and bone was encountered, requiring bone wax use to achieve hemostasis. While pathology reports of the specimen were awaited, a CT head was planned. A precautionary urine pregnancy test was positive. The β-hCG level was 5924 mIU/ml which was elevated above the discriminatory level. Transvaginal ultrasound showed no intrauterine pregnancy, normal adnexa and uniform 0.2 cm thick endometrium. Differential diagnoses at this time included completed spontaneous portion, early intrauterine pregnancy, and occult ectopic pregnancy. Repeat β-hCG values after 48 hours were slightly decreased to 5371 mIU/ml. Based on the declining β-hCG numbers, a recent spontaneous abortion was presumed. CT head demonstrated a dural-based mass projecting from the inner table of the left frontal bone, measuring 2.2 to 2.3 cm in maximum thickness, 4.1 to 4.2 cm in oblique anteroposterior extent, and 3.9 cm cranio-caudally. Intracranial mass effect was demonstrated, with 2 to 3 mm subfalcine deviation to the right. It was now evident the previously resected mass had infiltrated the calvarium into the intracranial space. Magnetic resonance imaging (MRI) with contrast demonstrated a heterogeneous pattern of enhancement of the intracranial mass. There was a small area of irregular enhancement at the deep margin of the intracranial component which was concerning for infiltration into the leptomeninges or potentially the cortex of the underlying left frontal lobe (Figure 1). At this point, the differential diagnosis included aggressive dural-based neoplasms such as hemangiopericytoma, hemangioendothelioma, and angiosarcoma, as well as other neoplastic lesions such as lymphoma, chloroma, and metastatic disease. Meanwhile, the β-hCG level reached 7062 mIU/ml, 6 days after the first β-hCG measurement. CT chest, abdomen, and pelvis with contrast demonstrated no evidence of metastatic disease. While the pathology reports from the first surgical resection were still pending, the patient underwent left frontal craniotomy, resection of the intracranial lesion with titanium mesh cranioplasty. During the procedure, the dura was found to be grossly involved. The brain tumor extended against the brain with no breach of the pial membrane. The mass itself was very firm, gray and red in color and hemorrhagic. Pathology reports from the first surgical specimen were consistent with a metastatic trophoblastic tumor with mixed features of choriocarcinoma and placental site trophoblastic tumor. Due to the rarity of the diagnosis, slides were sent to another institution for confirmation and the pathological diagnosis was verified from the external institution as well. Histopathology of the specimen from the intracranial mass, from the second surgery was identical to the external mass.
Histology reports described the mass as 4.1×4.0×1.0 cm red-pink, rubbery, nodular mass. Sectioning revealed a lobulated pink-dull white and focally hemorrhagic stroma with scattered dilated vessels consistent with a high-grade hemorrhagic tumor (Figure 2). Cytotrophoblasts were seen as mononucleated polygonal cells with clear cytoplasm and large vesicular nucleoli. Syncytiotrophoblasts were identified as large multinucleated cells with abundant eosinophilic cytoplasm and oval hyperchromatic nuclei (Figure 3). There was marked variation in nuclear size and shape with numerous anaplastic forms including multinucleated and degenerating cells. Malignant cells are seen to invade vascular channels and adjacent bone. The additional immunohistochemistry studies revealed diffuse neo-plastic cell expression of HCG on the syncytiotrophoblasts and variable Human placental lactogen (HPL) positivity (Figure 4). There was no cellular localization of pankeratin (Oscar), factor VIII, cytokeratin 7 and GATA-3. Antisera to HMB45, S100, vimentin, myogenin, smooth muscle actin, desmin, PAX-8, cytokeratin 20, estrogen receptor, thyroid transcription factor, CD34, and CDX-2 were not reactive.
Positron emission tomography did not show any suspicious hypermetabolic regions. The patient was diagnosed with stage IV gestational trophoblastic neoplasm according to the International Federation of Gynecology and Obstetrics (FIGO) classification system.
A detailed obstetrics history was elicited, the patient had a 12-year-old and a 20-month-old child. She had a history of 2 previous molar pregnancies several years ago, after the birth of the 12 yr old and before the birth of the 20-month-old child. Genetic testing of the products of the conception of the previous molar pregnancies was unfortunately not done. The WHO FIGO scoring for GTN for the patient was 12, with age more than 40 years, term antecedent pregnancy, over 13 months from index pregnancy, largest tumor size between 3 and ≤5 cm, intracranial metastatic lesion. A score of more than equal to 7 is considered high risk [4].
The patient was treated with 4 cycles of aggressive chemo-therapy: Etoposide, Methotrexate, Actinomycin D alternating weekly with Vincristine and Cyclophosphamide (EMA-CO) regimen. Following completion of chemotherapy, an MRI brain was repeated which showed expected post-operative changes with no evidence of recurrent neoplasm. Five months after completion of chemotherapy, she became pregnant against medical advice and successfully carried the pregnancy to full term. Four months postpartum β-hCG surveillance was started again and levels were checked every 3 months for one year followed by 6 monthly surveillance and all values were below 2 mIU/ml. Following pregnancy, she received a CT chest, abdomen, and pelvis which showed no evidence of metastatic disease within the chest, abdomen, and pelvis. At the time of writing this report, 3 annual surveillance MRI brain and CT chest abdomen, and pelvis were negative for recurrent disease.
Discussion
Gestational trophoblastic disease (GTD) was first defined more than a century ago as a group of disorders caused by abnormal proliferation of the placental trophoblasts [5,6]. The tropho-blasts produce β-hCG and it is thus it is elevated in all forms of GTD [6,7]. The nature of the GTD depends on the proliferative capacity of the constituent trophoblast, ranging from benign complete/partial hydatidiform moles to malignant entities like an invasive hydatidiform mole, gestational choriocarcinoma (GC), placental site trophoblastic tumor (PSTT) and epithelioid trophoblastic tumor (ETT). The above-mentioned malignant forms of GTN are collectively called Gestational Trophoblastic Neoplasia (GTN) [6,7].
Histologically, hydatidiform moles consist of a trophoblastic proliferation of chorionic villi with stromal edema within the villi. Invasive moles are characterized by trophoblastic overgrowth with penetration into the myometrium [7]. Gestational choriocarcinoma consists of sheets of primitive trophoblastic cells lacking villous structures with a propensity for vascular invasion [5,7]. PSTT is made up of intermediate trophoblastic cells at the placental site. ETT develops due to the neoplastic transformation of intermediate trophoblasts of chorion laeve [5,7].
The incidence of GTD is highest in Southeast Asian countries while it is lowest in European and North American countries [5]. The incidence of GTD in North America and Europe has remained constant between 1–2/1000 deliveries [8]. Worldwide, the incidence of GTD has been decreasing likely due to the improved nutritional status of women in underdeveloped countries [2,3].
GTD incidence is higher in both extremes of maternal age, with bimodal risk distribution [5,7]. Previous spontaneous abortion doubles the risk of molar pregnancy and a previous GTD is associated with 10 times increased risk of molar pregnancy [2,3].
Choriocarcinoma is the most common and the most aggressive form of GTN [3,9]. Choriocarcinoma can arise from any form of previous pregnancy like a normal pregnancy, ectopic pregnancy, spontaneous abortion, or hydatidiform moles but it arises most commonly from complete hydatidiform moles [6,7,9].
Even though choriocarcinoma as a neoplasm has over a 90% cure rate with chemotherapy, there are certain patients who are at high risk for treatment failure, especially with single-agent chemotherapy. Prior chemotherapy, β-HCG level of over 40,000 mIU/ml at the time of diagnosis, antecedent term pregnancy, metastasis to the brain or liver, and duration of more than 4 months since last pregnancy are considered indicators of poor prognosis and higher mortality rate [10]. Even though our patient’s pretreatment highest β-HCG level was 5924 mIU/ ml, she was still a high-risk patient because she had a full-term pregnancy over 20 months prior to her presentation and had intracranial metastasis. That is why aggressive combination chemotherapy, EMA-CO, was chosen for her treatment. There are reports of using other combination chemotherapy like Cisplatin, Etoposide and Cyclophosphamide (CEC) and Methotrexate, Dactinomycin and Etoposide (MDE) with good outcomes [10].
The interval between antecedent pregnancy and choriocarcinoma may vary from months to years [9]. A case of metastatic choriocarcinoma to the abdominal wall has been reported in a 50-year-old female with last known pregnancy over 20 years prior and like our case, a primary neoplasm could not be identified in this case as well [11]. Another case reported metastatic choriocarcinoma diagnosed in a postmenopausal woman, 38 years after her last pregnancy [12]. Thus, GTD can occur well beyond reproductive years.
Choriocarcinoma has been called the “great masquerader” as it can mimic many conditions including other malignancies like primary lung cancers [12]. It has a very high propensity for hematogenous spread with the lungs (60–75%), liver (15–20%), central nervous system (15–20%), and gastrointestinal tract (10–20%), being the most common sites of metastasis. The skin has rarely been reported as a site of metastasis [10]. It is even rarer for skin lesions to be the initial presentation of GTN as was the case in our patient.
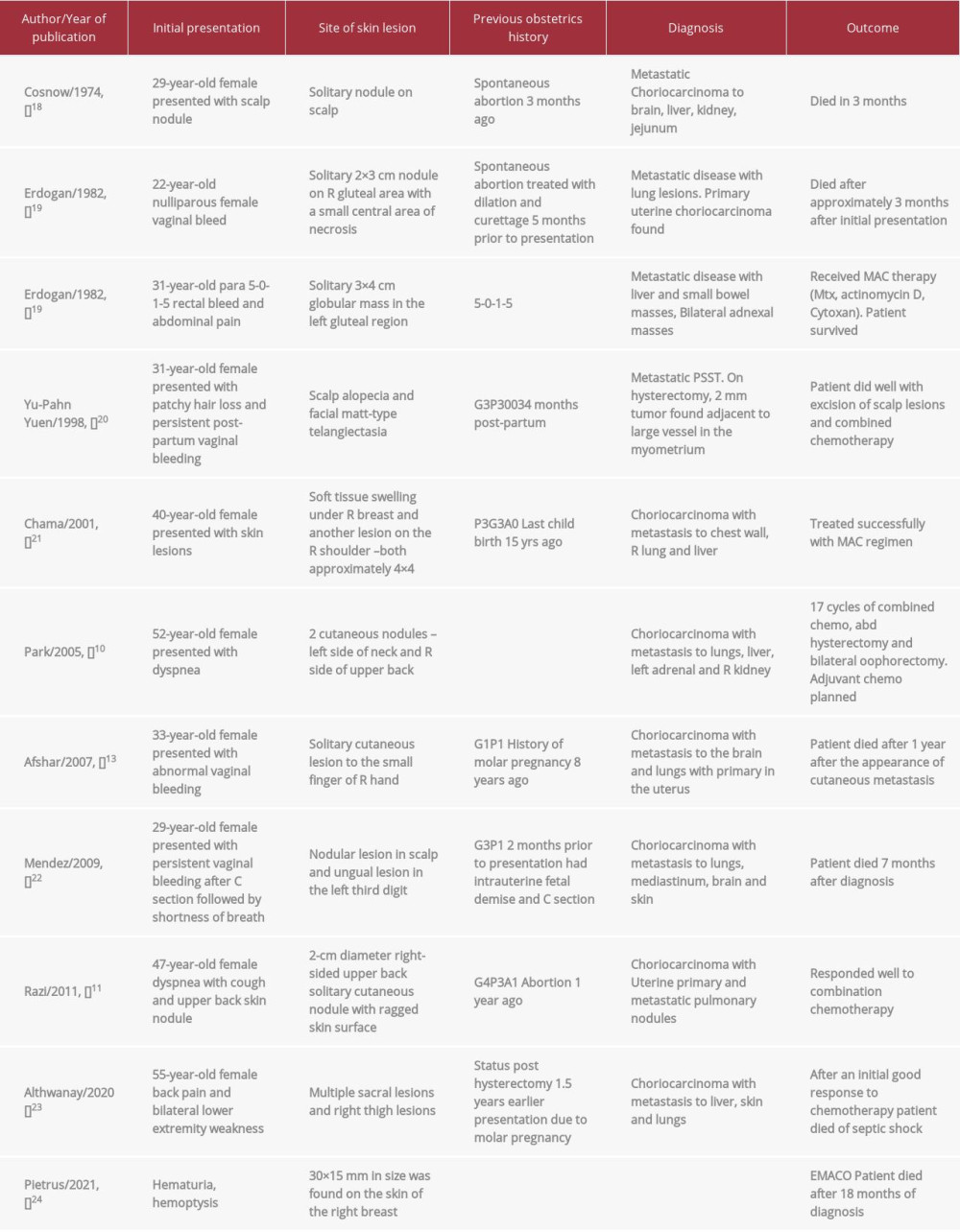
Generally, the metastatic spread of any cancer to the skin is an indicator of widespread dissemination and harbinger of poor prognosis [11,13]. The overall incidence of malignant metastasis to the skin is between 1-and 4% [13]. There are some case reports of testicular or non-gestational choriocarcinoma metastasizing to the skin [14–17] but to the best of our knowledge, there are only eleven cases of GTN with meta-static skin lesions have been reported in the English language [10,11,13,18–24] (Table 1).
Out of the above cases, 4 patients had the primary clinical presentation of metastatic skin lesions [11,18,20,21], as the presentation in our case where skin lesion was the first patient complaint. Cosnow described a case of a 29 yr old female with a recent history of spontaneous abortion who presented with a solitary scalp nodule, a biopsy of which revealed the diagnosis of choriocarcinoma. The patient had metastasis to multiple organs and succumbed to the disease [18]. Another case of metastatic choriocarcinoma presented with skin lesions on the chest wall after 15 years of childbirth [21]. Razi et al reported a case of choriocarcinoma which presented as a metastatic cutaneous nodule on the upper back. The patient had a history of abortion 1 year ago [11]. Yuen reported a case of placental site trophoblastic tumor metastatic to the skin which presented as alopecia neoplastica [20]. Among the twelve cases of GTN metastasizing to the skin, this was the only case of PSST, the rest were choriocarcinoma cases.
Placental site trophoblastic tumor (PSTT) is a rare form of GTN arising from the placental implantation site and consists of mononuclear intermediate gestational trophoblastic cells. PSST constitutes only 1–2% of all GTN cases [20]. It can occur months or years after a term of gestation. It has a lesser tendency of vascular invasion but has a propensity for lymphatic metastasis. During the earlier stages, PSST is known to be confined to the uterus with metastasis seen only in 10% of cases. Late cases can metastasize, especially to the lung and vagina.
PSST is known to produce lower levels of serum β-hCG than choriocarcinoma and is less sensitive to chemotherapy [20,25].
In our case, the patient’s tumor histology revealed a mixed trophoblastic tumor consisting of features of both choriocarcinoma and PSTT. In literature, there have been 6 reported cases of mixed PSST and choriocarcinoma [12,25,26]. Even though PSST is known to be less responsive to chemotherapeutic agents like methotrexate and actinomycin-D, combination chemotherapy like EMACO [25,26] was used to treat our patient successfully. The sensitivity of the neoplasm to chemotherapy would depend on the ratio of the cytotrophoblasts and syncytiotrophoblasts of choriocarcinoma to the intermediate trophoblasts of PSST.
Conclusions
Early diagnosis of GTN is imperative as it is one of the few cancers which can be completely cured with chemotherapy, even in the widely metastatic stage [12].
Our case is an example of how GTN can mimic other conditions and have a varied presentation. Knowledge of GTN, a high level of suspicion, and a thorough obstetric/gynecological history can aid in the diagnosis and successful treatment of GTN.
Figures
References:
1.. Rao A, Devi R, An unusual presentation of choriocarcinoma: Int J Reprod Contracept Obstet Gynecol, 2017; 6(4); 1668-71
2.. Richter C, Schwartz P, Clinical aspects of gestational trophoblastic disease: Gestational trophoblastic disease: Diagnostic and molecular genetic pathology, 2012; 179-90, USA, Springer
3.. Osborne R, Dodge J, Gestational trophoblastic disease: Obstet Gynecol Clin North Am, 2012; 39(2); 195-212
4.. , FIGO staging for gestational trophoblastic neoplasia 2000. FIGO Oncology Committee: Int J Gynaecol Obstet, 2002; 77(3); 285-87
5.. Hui P, Gestational trophoblastic disease: General aspects: Gestational trophoblastic disease: Diagnostic and molecular genetic pathology, 2012; 1-13, Springer
6.. Cunningham FG, Leveno KJ, Bloom SL, Gestational trophoblastic disease: Williams Obstetrics, 2018, New York, NY, McGraw-Hill Education
7.. Hoffman BL, Schorge JO, Bradshaw KD, Gestational trophoblastic disease: Williams gynecology, 2016, New York, NY, McGraw-Hill Education
8.. Drake RD, Rao GG, McIntire DD, Gestational trophoblastic disease among Hispanic women: A 21-year hospital-based study: Gynecol Oncol, 2006; 103(1); 81
9.. Hui P, Gestational choriocarcinoma: Gestational trophoblastic disease: Diagnostic and molecular genetic pathology, 2012; 127-34, USA, Springer
10.. Park SG, Chang JY, Kim SH, Bang D, Cutaneous metastasis of choriocarcinoma: A case report: J Korean Med Sci, 2005; 20(4); 683-86
11.. Razi T, Yaghoobi R, Feily A, Cutaneous metastasis of postpartum choriocarcinoma: Case report: Acta Dermatovenerol Croat, 2011; 19(1); 69-70
12.. Ramondetta LM, Silva EG, Levenback CF, Burke TW, Mixed choriocarcinoma in a postmenopausal patient: Int J Gynecol Cancer, 2002; 12(3); 312-16
13.. Afshar A, Ayatollahy H, Lotfinejad S, A rare metastasis in the hand: A case of cutaneous metastasis of choriocarcinoma to the small finger: J Hand Surg, 2007; 32(3); 393-96
14.. Chhieng DC, Jennings TA, Slominski A, Mihm MC, Choriocarcinoma presenting as a cutaneous metastasis: J Cutan Pathol, 1995; 22(4); 374-77
15.. Shimizu S, Nagata Y, Han-yaku H, Metastatic testicular choriocarcinoma of the skin. Report and review of the literature: Am J Dermatopathol, 1996; 18(6); 633-36
16.. Toberer F, Enk A, Hartschuh W, Grüllich C, Testicular choriocarcinoma with cutaneous metastasis in a 19-year-old man: J Cutan Pathol, 2018; 45(7); 535-38
17.. Senkal HA, Yılmaz T, Sözeri AB, Metastatic choriocarcinoma: A rare presentation as a neck mass: Ear Nose Throat J, 2013; 92(6); E42
18.. Cosnow I, Fretzin DF, Choriocarcinoma metastatic to skin: Arch Dermatol, 1974; 109(4); 551-53
19.. Ertüngealp E, Axelrod J, Stanek A, Skin metastases from malignant gestational trophoblastic disease: Report of two cases: Am J Obstet Gynecol, 1982; 143(7); 843-46
20.. Yuen YF, Lewis EJ, Larson JT, Scalp metastases mimicking alopecia areata. First case report of placental site trophoblastic tumor presenting as cutaneous metastasis: Dermatol Surg, 1998; 24(5); 587-91
21.. Chama CM, Nggada HA, Nuhu A, Cutaneous metastasis of gestational choriocarcinoma: Int J Gynecol Obstet, 2002; 77(3); 249-50
22.. Méndez K, Avellanet Y, Umpierre S, A rare case of cutaneous metastasis of postpartum choriocarcinoma: P R Health Sci J, 2009; 28(2); 143-45
23.. Althwanay AM, AlMaradheef RA, Althwanay RM, Choriocarcinoma presenting as skin lesions and back pain: Hematol Oncol Stem Cell Ther, 2020; 13(1); 48-50
24.. Pietrus M, Czekaj A, Dziadkowiak D, Metastatic choriocarcinoma presenting as renal colic and skin lesion – case report: Wiad Lek, 2021; 74(7); 1763-66
25.. Gari A, Placental site trophoblastic tumor and choriocarcinoma: An unusual presentation: BMC Res Notes, 2015; 8; 703
26.. Li X, Yu G, Xu W-B, Hua J, A rare case of choriocarcinoma admixed with placental site trophoblastic tumor: Int J Clin Exp Med, 2016; 9(7); 14833-38
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133