14 July 2022: Articles 
Selinexor in Patients from Argentina with Multiple Myeloma Treated with Multiple Prior Therapies: A Case Series
Unusual setting of medical care
Guillermina RemaggiDOI: 10.12659/AJCR.936505
Am J Case Rep 2022; 23:e936505






Abstract
BACKGROUND: Numerous treatment options are available for patients with multiple myeloma (MM). Because of the course of the disease, most patients will experience serial relapse or the MM will become refractory to most of these treatments, leaving patients with few or no treatment options over time. Selinexor, a treatment with a novel mechanism of action, is an oral selective inhibitor of nuclear export (SINE) compound that blocks exportin 1, the major nuclear exporter of tumor suppressor proteins.
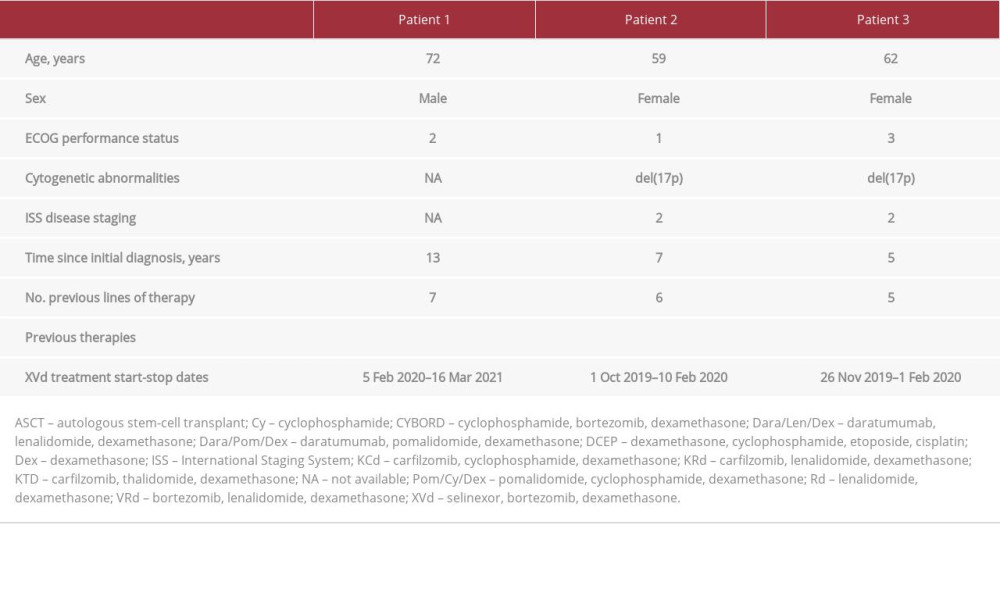
CASE REPORT: In this case series, we report on treatment with the weekly oral administration of selinexor combined with bortezomib and dexamethasone (XVd) in 3 patients from Argentina who were heavily treated (5-7 prior therapies) for MM that relapsed or was refractory to each previous treatment. Two patients had the high-risk cytogenetic abnormality del(17p). All 3 patients experienced efficacy with XVd reaching a best response of partial response or very good partial response. These responses were consistent with those of patients from the BOSTON study who were treated with XVd but were less heavily pretreated (1-3 prior therapies) and had a shorter median time since diagnosis of MM (7 years vs 3.7 years). The 3 patients experienced adverse events (AEs) that included nausea, thrombocytopenia, asthenia, and fatigue, which were similar to the most commonly reported AEs associated with selinexor treatment.
CONCLUSIONS: With its oral administration, novel mechanism of action, and responses in heavily pretreated patients, selinexor may help to address an important clinical need in the treatment of patients with relapsed/refractory MM.
Keywords: Multiple Myeloma, Selinexor, Antineoplastic Combined Chemotherapy Protocols, Argentina, Dexamethasone, Humans, Hydrazines, Neoplasm Recurrence, Local, Triazoles
Background
Multiple myeloma (MM) is an incurable disease characterized by an excess of monoclonal plasma cells found mostly in the bone marrow but also in peripheral blood and extramedullary sites [1]. Clinical signs of MM are associated with the effects of the M protein and/or cytokines released by the malignant cells followed by end-organ damage with hypercalcemia, renal dysfunction, anemia, lytic bone lesions, and susceptibility to infection.
Despite its apparent intractable nature, the survival rate of MM has improved over the years, with a 5-year survival rate of 27.57% in 1987 compared with 56.49% in 2012, while the number of new cases per 100 000 has increased from 5.93 in 1987 to 6.8 in 2017 [2]. Despite dramatic improvements in the treatment of MM, for most patients, the likelihood of deep and durable response decreases with each subsequent treatment regimen, with the eventual development of multiply refractory disease [3], leaving the patients with no remaining treatment options.
Using agents with novel mechanisms of action can effectively treat MM that is refractory to currently available therapeutic options. Selinexor, an oral selective inhibitor of nuclear export (SINE) compound that blocks exportin 1 (XPO1) and forces nuclear accumulation and activation of tumor suppressor proteins, inhibits nuclear factor κB and reduces oncoprotein messenger RNA translation. Based on the results from the phase 3 BOSTON trial [4], selinexor in combination with bortezomib and dexamethasone (XVd) received FDA approval in December 2020 for the treatment of adult patients with MM who have received at least 1 prior therapy. Additionally, the XVd regimen along with 2 other regimens, including selinexor plus dexamethasone in combination with pomalidomide (XPd) or daratumumab (XDd), have been added to the National Comprehensive Cancer Network guidelines for the treatment of relapsed MM [5].
Here, we describe the treatment and outcomes of 3 patients with heavily pretreated relapsed/refractory MM (5 to 7 prior therapies) who received weekly treatment with XVd in hospitals in Argentina. Common Adverse Events Evaluation Criteria v5.0 were used to evaluate adverse drug reactions. The patients were not part of a selinexor clinical trial. All the patients received the medication under the Karyopharm Expanded Access Program because they had exhausted all available treatment options with possible satisfactory outcomes in Argentina.
Case Reports
PATIENT 1:
A 72-year-old man with symptoms of anemia, hypercalcemia, and lytic bone lesions was diagnosed in January 2007 with IgA MM, stage unknown (the Revised International Staging System [R-ISS] score was not available), and the assessment for cyto-genetic risk also was not available. At diagnosis, the patient had hypertension, which was managed with standard of care.
The patient was treated with 7 different regimens for MM before XVd treatment was initiated (see Table 1). With the first-line therapy of thalidomide and dexamethasone and ASCT, the patient reached complete response before relapse in February 2011, at which time the patient was referred to the current clinic. The second line of therapy was cyclophosphamide, bortezomib, and dexamethasone plus pamidronate for 6 cycles and maintenance with bortezomib for 2 years. The best response, very good partial response, was reached in October 2012 and lasted until relapse in October 2013. Each of the subsequent lines of therapy had a best response of partial response and those responses lasted from 15 to 30 months before relapse. The most recent regimen before XVd was daratumumab plus dexamethasone. During the last MM relapse before XVd treatment began, the patient had several infections including pneumonia, Clostridioides difficile infection or pseudomembranous colitis, and salmonellosis. These infections were successfully treated with standard of care. At different times after diagnosis and before treatment with XVd, the patient had several comorbidities (coronary artery disease, venous thrombosis, upper gastrointestinal bleeding, and thrombocytopenia), which were managed with no complications and without modifying the XVd treatment regimen. The patient’s Eastern Cooperative Oncology Group (ECOG) performance status was 2.
On February 5, 2020, a regimen of 80 mg/week of selinexor plus 1.3 mg/m2 of bortezomib (days 1, 8, 15, and 22), and 40 mg/week of dexamethasone was initiated. Owing to the patient’s clinical status and underlying baseline thrombocytopenia, the starting dose of selinexor was lower than the approved dose in the XVd regimen of 100 mg QW. In August 2020, the patient reached a partial response, determined by the monoclonal IgA protein level (0.8 g/dL in January 2020 and 0.3 g/dL in August 2020) and improvement in the MM clinical symptoms of anemia, bone pain, and thoracic plasmacytoma. Grade 2 nausea and grade 4 thrombocytopenia related to XVd were reported. Nausea was managed with ondansetron and olanzapine and lasted 3 to 4 days. Thrombocytopenia was managed with eltrombopag (50 mg/day). Preclinical data have demonstrated decreased thrombopoietin signaling with selinexor is reversible with thrombopoietin receptor agonists, and eltrombopag has been shown to be effective in patients with persistent thrombocytopenia [7]. Treatment with 80 mg/week of selinexor plus 1.3 mg/m2 of bortezomib (Days 1, 8, 15, and 22), and 40 mg/week of dexamethasone continued until March 16, 2021, when treatment was stopped because the patient was diagnosed with COVID-19. At the time of the COVID-19 diagnosis, the MM response to XVd had changed from partial response to disease progression. The patient died on April 19, 2021, of COVID-19-related pneumonia.
PATIENT 2:
A 59-year-old woman was diagnosed in May 2012 with IgA MM (R-ISS stage 2) and had a cytogenetic profile that showed del(17p). Genetic profiling was not repeated after treatment. The patient had a history of active breast cancer, which required radiotherapy while she was receiving the first line of therapy for MM. The patient also had the comorbidity of esophagus achalasia related to amyloidosis and required surgical treatment before XVd therapy was started.
The patient was treated with 6 prior lines of therapy (Table 1) before treatment with XVd, reaching a best response of complete response with bortezomib, lenalidomide, and dexamethasone plus ASCT in October 2014, which lasted until July 2015, when disease progression was diagnosed. Two of the 3 subsequent lines of therapy were terminated because of disease progression; treatment with the third therapy of daratumumab, pomalidomide, and dexamethasone was stopped because of cytopenia. On October 1, 2019, 6 weeks after treatment with the sixth line of therapy (pomalidomide, bortezomib, and dexamethasone) ended, XVd was initiated with 100 mg/week of selinexor plus 1.3 mg/m2 of bortezomib on days 1, 8, 15, and 22 and 20 mg of dexamethasone on days 1, 2, 8, 9, 15, 16, 22, 23, 29, and 30. The ECOG performance status was 1 at XVd initiation. Selinexor was reduced to 80 mg at the beginning of cycle 2 because of grade 2 nausea and grade 4 thrombocytopenia; the latter was treated with eltrombopag (50 mg/day). The last dose of selinexor was administered on February 10, 2020. The best response with XVd treatment was very good partial response in January 2020, with a decreased monoclonal IgA protein level (3.73 g/dL at baseline to 0.32 g/ dL) and improved clinical symptoms, including less bone pain. Treatment with XVd was stopped on February 10, 2020 because of an abrupt loss of response and disease progression with severe thrombocytopenia and grade 3 asthenia related to XVd, although the contributing role of disease progression could not be ruled out. Thrombocytopenia was treated with increasing doses of eltrombopag, with no improvement, supporting a major role for disease progression. After treatment with XVd, the patient received carfilzomib, cyclophosphamide, and dexamethasone with GCSF and eltrombopag, with no disease response. The patient died in March 2020 of disease progression.
PATIENT 3:
A 62-year-old woman received a diagnosis in March 2014 of IgA MM (R-ISS stage 2) and the del(17p) cytogenetic abnormality. Genetic profiling was not repeated after treatment. At the time of the MM diagnosis, the patient had hypertension which was under control; the remainder of her medical history was considered unremarkable.
The patient previously was treated with 5 lines of therapy (Table 1) reaching a best response of complete response in December 2014 through September 2017 with the first-line treatment of cyclophosphamide, bortezomib, and dexamethasone plus ASCT and maintenance with lenalidomide. MM was refractory to subsequent lines of treatment, including a second ASCT. During the last 2 lines of therapy, the patient experienced profound cytopenia, which was treated with GCSF and transfusions. On November 26, 2019, approximately 1 month after the fifth line of therapy (daratumumab, pomalidomide, and dexamethasone) was stopped, XVd was initiated with 100 mg/week of selinexor plus 1.3 mg/m2 of bortezomib on days 1, 8, 15, and 22 and 20 mg dexamethasone on days 1, 2, 8, 9, 15, 16, 22, 23, 29, and 30. The ECOG performance status was 3 at the start of XVd treatment. The dose of selinexor was reduced to 80 mg in December 2019 because of grade 2 nausea (treated with oral ondansetron and 2.5 to 5 mg/day of oral olanzapine), grade 2 fatigue, and grade 4 thrombocytopenia. The best response with XVd treatment was a partial response, which was determined by monoclonal IgA protein level and improved MM clinical symptoms, including reduced bone pain. Treatment with XVd was stopped on February 1, 2020, because of alveolar hemorrhage and rhinovirus infection related to XVd, previous treatments, and highly refractory MM. No other treatments for MM were administered before the patient died in March 2020 of viral acute respiratory distress syndrome related to XVd, prior therapies, and immune compromise due to MM.
Discussion
Nearly all patients with MM will have a response to first-line therapy, but the clinical course of MM is characterized by eventual relapse and, with each subsequent treatment, earlier recurrence and the development of refractory disease. With the increasing number of new and novel therapies available for MM [5], it is possible for physicians to offer different consecutive therapies, preferably targeting distinct mechanisms, to patients who experience repeated relapses. However, the duration of the responses after each relapse typically decreases with increasing lines of therapy [3], eventually leaving the patient with no treatment options.
In this case series, we report on treatment with the weekly oral administration of XVd, which showed efficacy in each of the 3 patients who were heavily treated for MM that relapsed or was refractory to each previous treatment. Importantly, the 3 patients had MM that was refractory to bortezomib and to the more potent proteasome inhibitor carfilzomib. Of these patients, Patient 1 was treated with 7 prior lines of therapy before XVd treatment was initiated, reaching a best response of partial response after 6 months of treatment. This response was maintained for 7 months before the patient died from COVID-19-related pneumonia. The other 2 patients, both with the del(17p) cytogenetic abnormality, received 5 to 6 prior lines of treatment for MM. After 4 months of treatment, Patient 2 reached a very good partial response before the patient experienced disease progression. After approximately 2 months of XVd, Patient 3 reached a response of partial response. The 3 patients not only experienced efficacy with the XVd treatment, but the types of responses were in line with the best overall response of patients from the BOSTON study, who were treated with selinexor (100 mg/dose), bortezomib (1.3 mg/ m2), and dexamethasone (20 mg/dose), although the patients in the BOSTON study were much less heavily pretreated, with 51% receiving just 1 prior therapy and having a shorter median time since initial diagnosis [4]. These differences indicated that the XVd treatment had efficacy in the patients in the present case series even though they were in poorer health with much more refractory disease than were the patients in the BOSTON study. Using selinexor in the earlier lines may further enhance its activity and deliver improved tolerance [8]. XVd treatment in the BOSTON trial was initiated earlier in patients with less refractory MM (1–3 previous lines of therapy) and better overall health and resulted in significantly greater overall response rate and progression-free survival than in those treated with Vd. A recent expert review concluded that selinexor holds potential for being used in combination with highly active triplets in newly diagnosed multiple myeloma, based in part on the favorable response rates in the STOMP [9] and BOSTON trials [10].
The AEs experienced by the patients in the present case series included nausea, thrombocytopenia, asthenia, and fatigue. These AEs were similar to the most commonly reported AEs associated with selinexor treatment [11] and with the AEs in the BOSTON study, in which nausea and fatigue were the most frequently reported nonhematologic AEs (50% and 42%, respectively) and thrombocytopenia the most common hematologic AE (60%). As in the BOSTON study, these events were managed with standard supportive care; although, treatment was stopped for Patient 2 because of disease progression which led to thrombocytopenia and asthenia. An infectious event led to termination of treatment for Patient 3.
Patient 2 and Patient 3 didn’t sustain clinical benefit with XVd for as long as Patient 1; however, the disease responded to this selinexor-containing regimen after approximately 2 to 4 months of treatment, even though both patients were heavily pretreated for MM, had disease refractory to bortezomib and dexamethasone, and had the del(17p) cytogenetic abnormality. This genetic characteristic is an important prognostic factor of treatment outcomes [12] as well as a very high-risk feature and an indicator for poor outcome [13]; although, patients with del(17p) in the BOSTON study had a particularly strong response to XVd as compared with Vd [4].
Conclusions
In conclusion, patients with MM who have been treated with multiple lines of therapies and have limited treatment options available to them may benefit from treatment with XVd. This benefit may also include patients with high-risk cytogenetic abnormalities. In the context of the Phase 3 BOSTON study, these data suggest that use of the simple, once weekly XVd regimen may be particularly effective when used earlier in the course of disease in patients with less refractory MM and better overall health.
References:
1.. Anderson KC, Progress and paradigms in multiple myeloma: Clin Cancer Res, 2016; 22(22); 5419-27
2.. Howlader N, Noone AM, Krapcho M: Changes over time – new cases, deaths, 5-year survival. Myeloma — Cancer Stat Facts.SEER Cancer Statistics Review, 1975–2017, Bethesda, MD, National Cancer Institute Available from: []https://seer.cancer.gov/csr/1975_2017/
3.. Kumar SK, Therneau TM, Gertz MA, Clinical course of patients with relapsed multiple myeloma: Mayo Clin Proc, 2004; 79(7); 867-74
4.. Grosicki S, Simonova M, Spicka I, Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): A randomised, open-label, phase 3 trial: Lancet, 2020; 396(10262); 1563-73
5.. , NCCN Clinical Practice Guidelines in Oncology: Multiple Myeloma; version 1.2022 Updated August 16, 2021. [cited 2021 August 24]
6.. Durie BG, Harousseau JL, Miguel JS, International uniform response criteria for multiple myeloma: Leukemia, 2006; 20(9); 1467-73
7.. Gavriatopoulou M, Chari A, Chen C, Integrated safety profile of selinexor in multiple myeloma: Experience from 437 patients enrolled in clinical trials: Leukemia, 2020; 34(9); 2430-40
8.. Richter J, Madduri D, Richard S, Chari A, Selinexor in relapsed/refractory multiple myeloma: Ther Adv Hematol, 2020; 11; 2040620720930629
9.. Gasparetto C, Schiller GJ, Tuchman SA, Once weekly selinexor, carfilzomib and dexamethasone in carfilzomib non-refractory multiple myeloma patients: Br J Cancer, 2022; 126(5); 718-25
10.. Mo CC, Jagannath S, Chari A, Selinexor for the treatment of patients with previously treated multiple myeloma: Expert Rev Hematol, 2021; 14(8); 697-706
11.. Mikhael J, Noonan KR, Faiman B, Consensus recommendations for the clinical management of patients with multiple myeloma treated with selinexor: Clin Lymphoma Myeloma Leuk, 2020; 20(6); 351-57
12.. Czyż J, Jurczyszyn A, SzudySzczyrek A, Autologous stem cell transplantation in the treatment of multiple myeloma with 17p deletion: Pol Arch Intern Med, 2020; 130; 106-11
13.. Corre J, Perrot A, Caillot D, del(17p) without TP53 mutation confers a poor prognosis in intensively treated newly diagnosed patients with multiple myeloma: Blood, 2021; 137(9); 1192-95
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952658
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953243
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952989
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953049
Most Viewed Current Articles
07 Dec 2021 : Case report
22,697,854
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,914
174,914
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,026
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,962
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133