09 November 2022: Articles 
Necrotizing Soft-Tissue Infection of the Trunk Resulting From Wound Caused by a Centipede: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care
Yasutaka Tanaka1ABCDEF*, Takashi Mato1ADEF, Shoma Fujiya1B, Yuri Furuhashi1D, Tomotaka Takanosu1AD, Nobutaka Watanabe1D, Takafumi ShinjoDOI: 10.12659/AJCR.937869
Am J Case Rep 2022; 23:e937869






Abstract
BACKGROUND: Centipede envenomation is usually mild, but a review of the existing literature revealed a more serious course in a small proportion of patients. In fact, necrotizing soft-tissue infections have been reported following centipede stings in a small number of cases and require early diagnosis and treatment because of a high mortality rate.
CASE REPORT: A 78-year-old man was stung by a centipede on the left abdomen. Treatment with antimicrobial agents was started due to cellulitis, but extensive erythema developed from the left chest to the left buttock. Six days after being stung, he visited our hospital. Necrotizing soft-tissue infection was diagnosed and treated immediately with antibiotics and debridement on the left side of the abdomen and chest. Group A Streptococcus was detected in the fascia. The wound was left partially open and washed daily, resulting in gradual improvement of the wound condition. On hospitalization day 8, the open wound was able to be closed. Antimicrobial therapy was completed on hospitalization day 16. The patient showed good progress.
CONCLUSIONS: Centipede stings are not rare in tropical and subtropical regions, and most occurrences of centipede envenomation cause only local symptoms. However, we believe that even wounds caused by centipedes should be monitored, given the possibility of subsequent severe infection, as in the present case. In addition, the causative organisms identified in the present patient with necrotizing soft-tissue infection following a centipede sting were commensal bacteria of the skin. Future research is thus needed to clarify the relationship between these causative organisms and centipedes.
Keywords: Cellulitis, Emergency Medicine, Multiple Organ Failure, Streptococcal Infections, Male, Animals, Humans, Aged, Chilopoda, Soft Tissue Infections, Streptococcus pyogenes, Anti-Bacterial Agents
Background
Centipede stings are not rare in tropical and subtropical regions. Many patients do not seek medical attention after such events because most occurrences of centipede envenomation are mild and cause only local symptoms. Many kinds of envenomation have been reported, and anaphylaxis caused by some types of envenomation has also been described [1,2]. However, in some reports, secondary infection following centipede stings has proven more problematic than symptoms arising from the centipede venom [3]. A small number of wounds caused by centipedes develop into severe skin infections, such as necrotizing soft-tissue infections, which have a high mortality rate and require early diagnosis and treatment [4]. We describe a case of necrotizing soft-tissue infection of the trunk, secondary to a wound caused by a centipede.
Case Report
A 78-year-old man was stung on the left abdomen by a centipede in rural Japan 6 days before presentation to our hospital. The centipede was about 5 cm long, and the patient identified the arthropod as a member of the genus
The patient’s medical history included angina pectoris, for which he was taking an antiplatelet medication. He had no history of diabetes mellitus or use of immunosuppressive agents or corticosteroids.
On presentation, the patient had a heart rate of 92 beats/min, blood pressure of 88/45 mmHg, respiratory rate of 18 breaths/ min, and temperature of 37.6°C. He was clearly aware. On physical examination, extensive erythema and tenderness were observed on the left side from the chest to the buttocks (Figure 1). A painful ulcer and necrosis were observed on the left side of the abdomen (Figure 2). A small amount of pus was drained from the ulcer. Blood tests revealed an increased inflammatory response and renal dysfunction (Table 1). Computed tomography showed no gas production or abscess formation apparent in the abdominal wall.
The treatment course was as follows. At the time of hospitalization, circulatory and respiratory failure were observed. Renal dysfunction was also observed. The sequential organ failure assessment score was 11 on the day of admission. We diagnosed septic shock. Systemic management was initiated with ventilation and antihypotensive agents. After submitting blood cultures, antimicrobial therapy was started with meropenem, vancomycin, and clindamycin. A tetanus vaccination was also administered. On the day of admission, debridement was performed from the left side of the chest to the lateral abdomen. A skin incision was made from the left axilla to the buttock, revealing cloudy exudate. The external oblique fascia was sampled and submitted for pathological examination and bacterial culture examination. Parts of the external oblique fascia, latissimus dorsi fascia, and pectoralis major fascia were excised, and all darkened adipose tissue was removed. The wound was left partially open and cleaned daily. On hospitalization day 2, the antimicrobial agents were changed to ampicillin and clindamycin. Pathological examination revealed extensive necrosis of the fascia and neutrophilic infiltration (Figure 3). Fascia culture tests revealed group A Streptococcus (GAS) on hospitalization day 3. Blood culture tests were negative. Starting on hospitalization day 4, cefotaxime was used. The wound condition gradually improved with daily washing. On hospitalization day 8, the open wound could be closed. Antimicrobial therapy was terminated on hospitalization day 16. The patient showed good progress and was transferred to another hospital for rehabilitation on hospitalization day 31.
Discussion
More than 3500 species of centipedes have been identified worldwide, and they are divided into 5 orders: Scutigeromorpha, Lithobiomorpha, Craterostigmomorpha, Geophilomorpha, and Scolopendromorpha [3]. Centipedes are found mostly in warmer climates around the world and like moist and dark places [5]. Centipedes are often found under stones and in decaying wood in abandoned houses [5]. Many occurrences of centipede envenomation are caused by the order Scolopendromorpha [3], which shows overlapping habitats with the residential environment of humans, making cases of centipede envenomation in Asia very common. Symptoms mostly take the form of temporary localized pain, edema, itching, and burning sensations [6]. As most symptoms resolve within days, many patients do not seek medical attention. Localized symptoms are caused by centipede toxins, which include histamine, serotonin, and phospholipase A2 [3]. Some reports have advised that “warming is helpful because venom is heat sensitive” [1,6], but the evidence for this is not well established. Past reports have stated that tetanus toxoid should be administered [1], but prophylactic antimicrobials for wound infection are not indicated in all cases [2,7]. However, these treatments have not been studied on a large scale. Considering the present case, we think that thorough cleaning is warranted after a centipede sting, and if symptoms do not improve, antibacterial treatment should be implemented without hesitation.
One of the more serious symptoms of centipede envenomation is anaphylaxis. Centipede and bee venoms reportedly share some antigens, suggesting the potential for cross-reactivity [2,7]. If a patient is allergic to bees, clinicians should also be wary of anaphylaxis following centipede envenomation. In the present case, the patient had been working as a forest ecologist for many years and had possibly experienced bee and centipede stings in the past. Although redness and hypotension can also be seen in anaphylactic shock, the course in this case was hardly typical of an allergic reaction or anaphylactic symptoms. Erythema spread rapidly from the localized area in our patient, and symptoms worsened over time. There was little concern that he had anaphylactic symptoms. The main cause of the severe symptoms in the present case appeared to be infection. Necrotizing soft-tissue infections or similarly severe soft-tissue infections have been reported following centipede stings (Table 2) [8–10]. In most cases, patients present with symptoms such as pain and redness. Patients often take several days to visit the hospital, and some patients may die without antimicrobial therapy and debridement. All centipedes in the reported fatal cases were Scolopendra, and the causative organisms identified in those cases were all methicillin-sensitive
Necrotizing soft-tissue infection is well known to occur after skin and mucous membrane injuries due to events including burns, trauma, and insect bites [11]. Both MSSA and GAS are commensal bacteria of the skin. Although the patient did not remember scratching the wound, indigenous bacteria are likely to have invaded from the damaged region following the centipede sting. On the other hand, as with some animal bites, the possibility of invasion and infection by bacteria living on the centipede’s jaws and limbs cannot be ruled out. However, in our literature search, we could not find any literature regarding commensal bacteria on the centipede; future studies are expected. For our patient, whether streptococci were present on the centipede’s jaws and limbs remains unclear.
Conclusions
Although many cases of centipede envenomation and stings are mild, a small number of wounds caused by centipede stings develop necrotizing soft-tissue infection. The wound should therefore be examined carefully and the possibility of severe infection kept in mind. The causative organisms identified in patients with necrotizing soft-tissue infection following centipede stings have been MSSA and GAS. Additional research is necessary to clarify the relationships between causative organisms and centipedes.
References:
1.. Joshua L, Fenderson MD, Centipede envenomation: Bringing the pain to Hawai’i and Pacific Islands: Hawaii J Med Public Health, 2014; 73(11); 41-43
2.. Undheim EA, Fry BG, King GF, Centipede venom: Recent discoveries and current state of knowledge: Toxins (Basel), 2015; 7(3); 679-704
3.. Undheim EAB, King GF: Toxicon, 2011; 57; 512-24
4.. Van Stight SF, de Vries J, Bijker JB, Review of 58 patients with necrotizing fasciitis in the Netherlands: World J Emerg Surg, 2016; 11; 21
5.. Fung HT, Lam SK, Wong OF, Centipede bite victims: A review of patients presenting to two Emergency Departments in Hong Kong: Hong Kong Med J, 2011; 17(5); 381-85
6.. Balit CR, Harvey MS, Waldock JM, Isbister GK, Prospective study of centipede bites in Australia: J Toxicol Clin Toxicol, 2004; 42(1); 41-48
7.. Washio K, Masaki T, Fujii S, Anaphylaxis caused by a centipede bite: A “true” type-I allergic reaction: Allergol Int, 2018; 67(3); 419-20
8.. Puzzo A, Pari C, Bettinelli G, An unusual two-stage infection following a scolopendra bite: Acta Biomed, 2020; 91(14-S); e2020009 30
9.. Uzel AP, Steinmann G, Bertino R, Korsaga A, Necrotizing fasciitis and cellulitis of the upper limb resulting from centipede bite: Two case reports: Chir Main, 2009; 28; 322-25
10.. Serinken M, Erdur B, Sener S: The Internet Journal of Emergency Medicine, 2005; 2; 1-5
11.. Stevens DL, Bryant AE, Necrotizing soft-tissue infections: New Engl J Med, 2017; 377; 2253-65
Figures
Tables
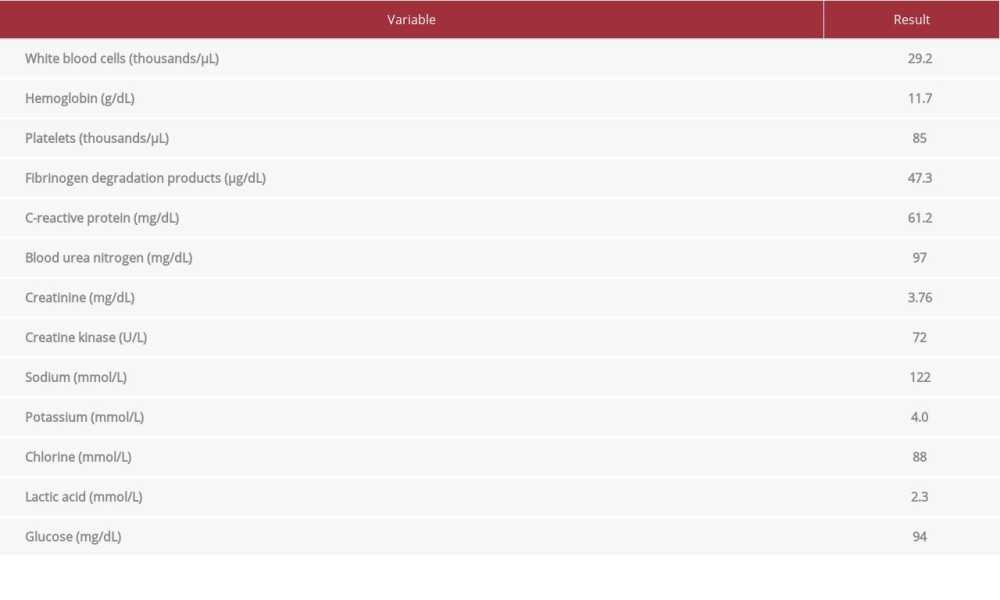 Table 1.. Results of blood tests on presentation to our hospital.
Table 1.. Results of blood tests on presentation to our hospital.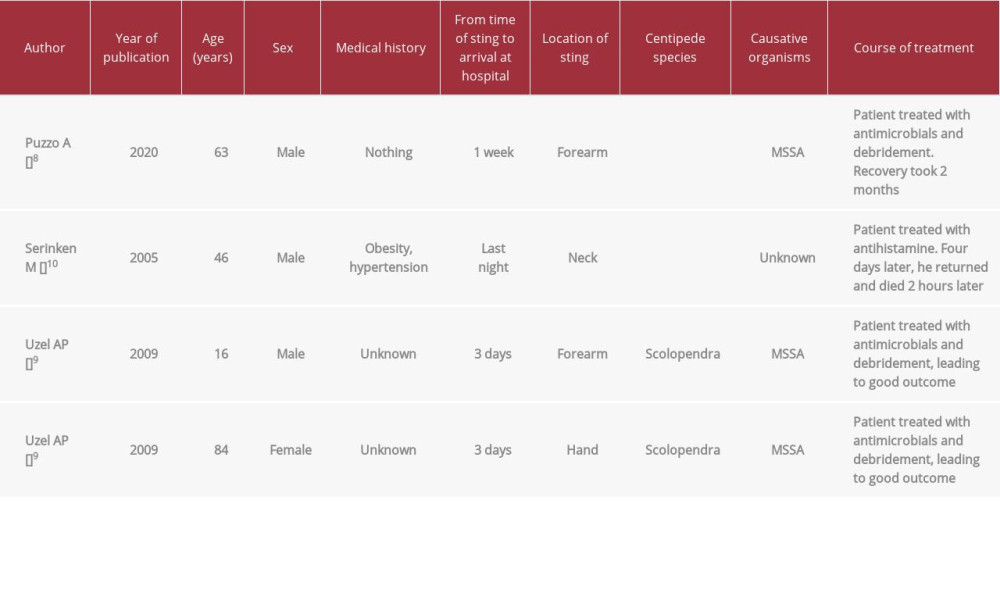 Table 2.. Past reports of necrotizing soft-tissue infections or similar severe soft-tissue infections caused by a centipede sting.Table 1.. Results of blood tests on presentation to our hospital.Table 2.. Past reports of necrotizing soft-tissue infections or similar severe soft-tissue infections caused by a centipede sting.
Table 2.. Past reports of necrotizing soft-tissue infections or similar severe soft-tissue infections caused by a centipede sting.Table 1.. Results of blood tests on presentation to our hospital.Table 2.. Past reports of necrotizing soft-tissue infections or similar severe soft-tissue infections caused by a centipede sting. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133