28 September 2023: Articles 
Asymptomatic Essential Thrombocytosis Presenting with Extrahepatic Portal Vein Thrombosis: A Case Report
Unusual clinical course, Challenging differential diagnosis, Educational Purpose (only if useful for a systematic review or synthesis)
Yoshikazu Yakami1ABCDEFG*, Toshihiko Yagyu2ABCDEFG, Tomoki Bando2ABCDEFG, Masakazu Hanada2ABCDEFGDOI: 10.12659/AJCR.938547
Am J Case Rep 2023; 24:e938547






Abstract
BACKGROUND: Essential thrombocytosis (ET) is a myeloproliferative neoplasm variant that leads to excessive platelet production in the bone marrow. Janus kinase 2 (JAK2) mutation is observed in 60% of ET cases. The risk of thrombosis increases with the presence of this mutation. ET can cause systemic thrombosis, including extra-portal vein thrombosis (EHPVT). In patients with ET-induced EHPVT, varied symptoms generally occur. However, our case was asymptomatic. This condition is relatively rare.
CASE REPORT: A 49-year-old woman presented to our hospital for a detailed clinical examination 1 month after a health examination, and blood tests revealed microcytic anemia and thrombocytosis. The patient had no current concerns and had no relevant medical or alcohol consumption history. Esophagogastroduodenoscopy demonstrated esophageal varices, with portal hypertension suspected as the underlying cause. Contrast-enhanced computed tomography scans revealed a thrombus in the portal vein, but liver cirrhosis and a tumor were ruled out. JAK2 mutation was positive, which led to myeloproliferative neoplasms being considered as the differential diagnosis. Bone marrow biopsy demonstrated many mature megakaryocytes with large and irregular nuclei and platelet aggregation in the field of view, leading to the diagnosis of ET.
CONCLUSIONS: This case study describes a patient with EHPVT caused by JAK2-positive ET. This case report emphasizes that physicians should consider myeloproliferative neoplasms as part of their differential diagnosis when presented with EHPVT.
Keywords: essential thrombocytosis, Extrahepatic Portal Vein Thrombosis, Female, Humans, Middle Aged, Portal Vein, Thrombocythemia, Essential, Venous Thrombosis, Thrombosis, Thrombocytosis, Bone Marrow Neoplasms
Background
Essential thrombocytosis (ET) is a myeloproliferative neoplasm (MPN) that leads to excessive platelet production in the bone marrow. The incidence of ET is estimated at 1.2 to 3.0 per 100 000 population per year.
In a retrospective study of 1076 patients with ET conducted by the Mayo Clinic, the median age at diagnosis was 58 years (range 18 to 96), 67% were woman, and the median platelet count was 876×109/L (range 451×109 to 3460×109). In a large international study of patients with ET, the 10-year survival rate was 89%. On the other hand, the rates of progression to leukemic or fibrotic transformation were 0.7% and 0.8%, respectively. Thus, most patients could have an almost normal life expectancy [1].
The 2016 World Health Organization (WHO) diagnostic criteria for ET are as follows: 1) platelet count ≥450×109/L; 2) bone marrow biopsy demonstrating proliferation mainly of the megakaryocyte lineage with increased numbers of enlarged, mature megakaryocytes with hyperlobulated nuclei; 3) not meeting the WHO criteria for BCR-ABL1+ chronic myeloid leukemia, polycythemia vera, primary myelofibrosis, myelodysplastic syndromes, or other myeloid neoplasms; and 4) presence of JAK2, calreticulin, or myeloproliferative leukemia virus onco-gene mutation [2].
Most patients with ET harbor a mutation in 1 of 3 genes: Janus kinase 2 (JAK2) V617F (in 60%), CALR (in 20%), or MPL (in 3%). In addition, 10% to 20% of all cases have none of these 3 driver mutations. JAK2 mutation is observed in 60% of ET cases. The risk of thrombosis increases with the presence of this mutation. ET could also potentially cause extrahepatic portal vein thrombosis (EHPVT). EHPVT is an obstruction of the extrahepatic vein with or without involvement of the intrahepatic portal vein or the splenic or superior mesenteric veins. In patients with thrombosis due to MPN, vasomotor symptoms (eg, migraine or pruritus) and constitutional symptoms (eg, night sweats, general fatigue, and weight loss) are generally present [1]. However, the patient in this case report had no symptoms. This condition is relatively rare. Herein, we report an asymptomatic case of ET-induced EHPVT.
Case Report
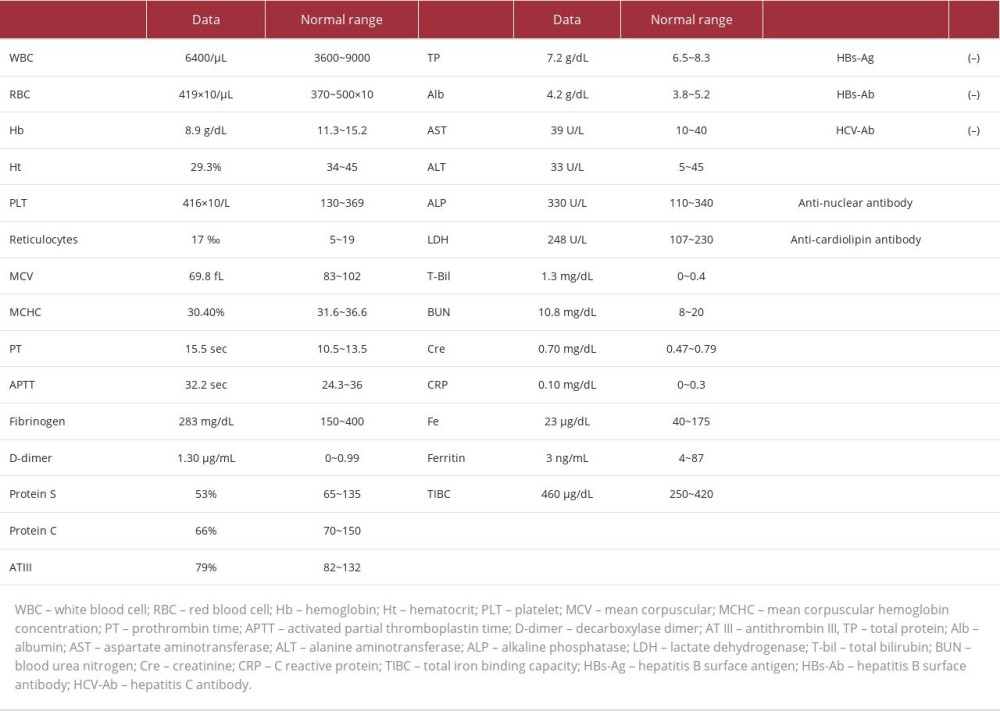
A 49-year-old woman presented to at our hospital for a detailed clinical examination 1 month after a health examination, and blood tests revealed microcytic anemia and thrombocytosis. The patient had no relevant medical or alcohol consumption history and presented with no concerns. A blood test led to the diagnosis of iron-deficiency anemia (Hb: 8.9 g/dL, MCV: 69.8 fL, MCHC: 30.4%, Fe: 23 μg/dL, ferritin: 3ng/dL, TIBC: 460 μg/dL) and thrombocytosis (platelets: 416×109 count/L). Liver dysfunction was not demonstrated on the blood test. The tests for anti-hepatitis C antibody and hepatitis B surface antigen were negative (Table 1). Esophagogastroduodenoscopy (EGD) was performed for anemia screening. Esophageal varices (Modified Paquet classification grade I) were noted in the investigation (Figure 1).
In addition, since the fecal occult blood test was negative, lower gastrointestinal bleeding was considered to be unlikely. Contrast-enhanced computed tomography (CT) was performed as portal hypertension was considered as a possible diagnosis. The CT scan revealed that the patient’s portal vein was expanded and meandering with collateral circulations. It also demonstrated an extrahepatic portal vein thrombus (Figure 2) that was the suspected cause of the portal hyper-tension. Chronic hepatitis and liver cirrhosis were ruled out based on the liver function status; moreover, a malignant tumor was not identified. The CT and blood test results were also negative for abdominal infection. Protein C or S deficiency, anti-thrombin III (AT III) deficiency, anti-phospholipid antibody syndrome, and autoimmune disease were ruled out based on the blood test results.
A positive JAK2 mutation (34.7%) was identified during the blood tests, leading to a suspicion of MPN. A bone marrow biopsy was, thus, performed, and it demonstrated many local mature megakaryocytes without dysplasia, immature cells, or fibrosis. These megakaryocytes had large and irregular nuclei, and platelet aggregation was observed in the field of view (Figure 3). This led to the diagnosis of ET. The patient was prescribed low-dose aspirin (100 mg/day) and hydroxycarbamide (500 mg×3 times/week) for ET and warfarin (2 mg/day) for EHPVT. She continued to visit the hematology department regularly and at her most recent follow-up appointment (24 weeks after treatment initiation), she was in stable clinical condition.
Discussion
ET is a MPN variant related to other types of MPNs, such as polycythemia vera, primary myelofibrosis, and chronic myeloid leukemia. ET leads to excessive production of platelets in the bone marrow; hence, it may be responsible for causing PVT. Thromboembolism occurs in 13% of all cases of ET, with a recurrence rate of 5.6% per year [3]. In our case, ET-induced EHPVT was suspected of causing the observed portal hypertension and esophageal varices [4]. The subsequently performed bone marrow biopsy demonstrated many mature megakaryocytes with large and irregular nuclei and platelet aggregation. Despite the bone marrow cell morphology, the platelet count of our patient was 416×109/L, which is less than that included in the diagnostic criteria for ET. Generally, hypersplenism owing to portal hypertension results in pancytopenia. Therefore, the blood cell count of patients with MPN tends to be closer to the normal range [5]. Judging from the information mentioned earlier, the platelet count in our case was less than the actual level. In addition, the patient was positive for the JAK2 mutation; thus, ET could still be diagnosed.
The JAK2 (V617F) mutation involves a change of valine to phenylalanine at position 617. This mutation is considered a crucial factor in the clinical course of MPNs, such as polycythemia vera and ET. The risk of thrombosis almost doubles with the presence of this mutation. JAK2 mutations are also considered to be an independent risk factor for splanchnic vein thrombosis (SVT) from MPN [6]. The mechanism of thrombosis in a case with JAK2 mutation was reported to be due to an increase of P secretin as an adhesion factor on the surface of platelets, decreased activity of protein C and protein S as anticoagulant factors, and vascular endothelial dysfunction caused by reactive oxygen due to neutrophil activation [7]. Since PVT is highly predominant among cases of liver cirrhosis, abdominal infection, and cancer, checking for JAK2 mutation in such cases is often unnecessary. Therefore, only cases with uncertain causes are subjected to a JAK2 mutation check. The blood test results in our patient revealed iron-deficiency anemia and thrombocytosis. She had a negative medical and alcohol consumption history as well as normal liver function test results. Her hepatitis virus and anti-nuclear antibody tests were negative. The surface of the patient’s liver was smooth, with a sharp edge; the inside of the liver was diffuse, without tumors. Consequently, chronic hepatitis and liver cirrhosis were ruled out. In addition, protein C or S deficiency, ATIII deficiency, anti-phospholipid antibody syndrome, and autoimmune disease were ruled out based on the blood test results.
In this case, mild prolongation of prothrombin time and mildly decreased protein C and protein S activity were revealed in the blood test results. JAK2 mutation can result in decreased protein C and S activity [8]. Therefore, abnormal coagulation factor activity could have also occurred. As mentioned earlier, the PVT in our case had an uncertain origin; hence, we investigated the patient for JAK2 mutation.
ET prognosis is considered to be better than that of other MPNs. However, this is dependent on any associated arterial thrombosis, such as myocardial infarction or stroke [9]. The risk of thrombosis is estimated based on a history of thrombosis, presence of JAK2 mutation, more than 60 years of age, and cardiovascular risk factors. Patients are classified into 4 risk categories: very low, low, intermediate, and high [1,10]. In high-risk groups for thrombosis, low-dose aspirin as anti-thrombotic therapy and hydroxycarbamide as myelosuppressive therapy are recommended [1,11]. Both drugs are reported to efficiently reduce the risk of thrombosis in cases of ET [12]. Although the thrombosis in our case was a venous thrombosis, low-dose aspirin and hydroxycarbamide were prescribed to our patient prophylactically, as was warfarin, which was prescribed specifically for PVT. To date, arterial thrombosis has not occurred.
Conclusions
This case study describes a patient with ET-induced EHPVT who presented without any concerns. This case emphasizes that physicians should consider MPNs as part of their differential diagnosis in patients with EHPVT.
Figures
References:
1.. Ayalew T, Animesh P, Essential thrombocythemia: N Engl J Med, 2019; 381; 2135-44
2.. Kentaro I, Yoshihide U, Masako M, Portal vein thrombosis due to essential thrombocythemia with limited cutaneous systemic sclerosis: Clin J Gastroenterol, 2021; 14; 293-96
3.. De Stefano V, Za T, Rossi E, Recurrent thrombosis in patients with polycythemia vera and essential thrombocythemia: Incidence, risk factors, and effect of treatments: Haematologica, 2008; 93; 372-80
4.. Jian-Bo W, Yang G, Jun-Wei L, Gastroesophageal varices in a patient presenting with essential thrombocythemia: A case report: World J Clin Cases, 2021; 9; 1871-76
5.. Smallberg JH, Arends LR, Valla DC, Myeloproliferative neoplasms in Budd-Chiari syndrome and portal vein thrombosis: A meta-analysis: Blood, 2012; 120; 4921-28
6.. Yonal I, Pinarbasi B, Hindilerden F, The clinical significance of JAK2V617F mutation for Philadelphia-negative chronic myeloproliferative neoplasms in patients with splanchnic vein thrombosis: J Thromb Thrombolysis, 2012; 34; 388-96
7.. Pardanani A, Lasho TL, Hussein K, JAK2V617F mutation screening as part of the hypercoagulable work-up in the absence of splanchnic venous thrombosis or overt myeloproliferative neoplasm: Assessment of value in a series of 664 consecutive patients: Mayo Clin Proc, 2008; 83; 457-59
8.. Marchetti M, Castoldi E, Spronk HM, Thrombin generation and activated protein C resistance in patients with essential thrombocythemia and polycythemia vera: Blood, 2008; 112; 4061-68
9.. Palandri F, Catani L, Testoni N, Long-term follow-up of 386 consecutive patients with essential thrombocythemia: Safety of cytoreductive therapy: Am J Hematol, 2009; 84; 215-20
10.. Paola G, Naseema G, Giacomo C, Mutation and thrombosis in essential thrombocythemia: Blood Cancer J, 2021; 11; 77
11.. Ayalew T, Alessandro M, Vannucchi , Essential thrombocythemia treatment algorithm 2018: Blood Cancer J, 2018; 8; 2
12.. Squizzato A, Romualdi E, Passamonti F, Middledorp S, Antiplatelet drugs for polycythemia vera and essential thrombocythemia: Cochrane Database Syst Rev, 2013; 4; CD006503
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133