15 May 2023: Articles 
IgG4-Related Disease of Temporal Bone Presenting as Unilateral Mastoiditis and Cerebral Thrombosis in a 22-Year-Old Man
Unusual setting of medical care, Rare disease
Natália Carasek12ABF*, Aline Motta Bitencourt1CDF, Juliana Guedes Amorim Mendonça1BC, Fayez Bahmad Jr.12ADDOI: 10.12659/AJCR.939013
Am J Case Rep 2023; 24:e939013






Abstract
BACKGROUND: Immunoglobulin G4-related disease (IgG4-RD) is a rare autoimmune disease that can affect multiple organs and manifest itself as a mass at any region of the body. Due to its several differential diagnoses, investigation and treatment are still challenging. Therefore, imaging, serology, and histopathology are required to confirm the diagnosis. The involvement of the temporal bone is an uncommon presentation, often mistaken for malignancy, with vague symptoms. Therefore, we present a 22-year-old Brazilian man, diagnosed with IgG4-related disease, manifesting with unilateral mastoiditis, sensorineural hearing loss, cerebral venous sinus thrombosis, and a mass in the left temporal bone.
CASE REPORT: A 22-year-old Brazilian male patient first presented with coughing and precordialgia. Chest scans showed pleural effusion and diffuse areas of ground-glass opacity. A year later, the patient developed severe headache, along with aural fullness, facial pressure, and otorrhea. Imaging detected cerebral thrombosis with failure in the filling of the transverse and left sigmoid sinuses and pachymeningeal thickening in the right cerebral hemisphere, with contrast enhancement. Pure tone audiometry showed thresholds consistent with severe sensorineural hearing loss in the left ear. The patient underwent mastoidectomy with removal of large amounts of inflammatory tissue that were sent to histopathological analysis with compatible signs of IgG4-RD. Corticosteroids and rituximab completed the treatment.
CONCLUSIONS: Early recognition and appropriate treatment of IgG4-RD are imperative to avoid complications and serious irreversible organ damage. This report has presented an atypical case of IgG4-RD of the left temporal bone that was diagnosed and managed according to current guidelines.
Keywords: Immunoglobulin G4-Related Disease, Intracranial Thrombosis, Mastoiditis, Humans, Male, young adult, Adult, Temporal Bone, Hearing Loss, Sensorineural
Background
Immunoglobulin G4-related disease (IgG4-RD) is a polymorphic autoimmune disease that can affect multiple systems in the form of fibroinflammatory disorders. First reported in 2003 in Japan, it still remains poorly understood [1,2]. It has an insidious presentation and can affect many different body organs such as pancreas, lung, and lacrimal and salivary glands, with a broad spectrum of clinical manifestations. Due to its several differential diagnoses, investigation and treatment are still challenging. Clinical data, imaging, serologies and biopsies are in the arsenal for this investigation [3]. Laboratory findings suggestive of IgG4-RD, including low levels of total hemolytic complement, CH50, and the individual components, C3 and C4, have been described [4,5]. Although found in 60–70% of the cases, high levels of serum IgG4 are no longer considered essential for the recognition of IgG4-RD [6].
In the otolaryngology field, multiple presentations are possible, since this autoimmune condition can affect virtually every tissue in the body. The involvement of parotid, salivary, submandibular, and lacrimal glands, when present in combination, are referred to as Mikulicz disease [7]. Known as Küttner’s tumor, the presentation of chronic sclerosing sialadenitis is in the list of reported signs, as well as inflammatory orbital pseudotumors, thyroiditis, and nasopharynx manifestations associated with lymphadenopathies [7]. Another possible presentation is laryngeal stenosis, a rare condition with first symptoms manifesting as swelling, dyspnea, and dysphonia [8].
IgG4-RD involving the temporal bone is an uncommon and underrecognized pathology often mistaken for malignancy. Clinically, it presents with vague otological symptoms. The most common are progressive hearing loss, otalgia, and headache [9]. Ear fullness, pressure, and otorrhea are other possible symptoms [10]. Previous case studies also reported destructive mastoid bone lesions, in addition to pachymeningitis and cranial nerve paresis [11].
IgG4-RD is more common in middle-aged and elderly men, but can also be seen in women and has been reported in children as well. Patients often feel well at the time of diagnosis, resulting in the disease being frequently an incidental finding based upon a radiological aspect or histopathologic examination of a tissue specimen [12]. The present report describes a 22-year-old Brazilian man presenting with unilateral mastoiditis, sensorineural hearing loss, cerebral venous sinus thrombosis, and a mass in the left temporal bone, diagnosed as IgG4-related disease and treated with surgical excision, corticosteroids, and rituximab.
Case Report
A 22-year-old Brazilian man was asymptomatic until 12 years of age, when he started presenting with cough and precordialgia. Due to the severity of the case, a detailed investigation was performed and a chest computed tomography (CT) scan showed pleural effusion and diffuse areas of ground-glass opacity. Adjacent symptoms of allergic rhinitis were described. A year later, the patient presented with a severe headache, along with aural fullness, facial pressure, and otorrhea. He underwent clinical and imaging investigations. No symptoms related to the pharynx, salivary or lacrimal glands, or other locations were reported.
Magnetic resonance angiography detected cerebral thrombosis with filling failures in the transverse and left sigmoid sinuses (Figure 1) and pachymeningeal thickening in the right cerebral hemisphere (Figure 2), with contrast impregnation. Prior pure tone audiometry showed thresholds of 6 dB in the right ear and 71 dB in the left ear, consistent with severe sensorineural hearing loss on the left, with a ramp configuration (Figure 3).
Surgical treatment was indicated, with a retro-auricular approach. We performed a wide mastoidectomy with removal of large amounts of inflammatory tissue involving the entire mastoid cavity, and encountered significant meningeal thickening and mucosal edema involving the sigmoid sinus. A meningeal fragment was collected for anatomopathological study.
According to the most recent systematic review, diagnosis of this condition involves painstaking work, and histopathological analysis is crucial in establishing a definitive diagnosis [9]. The 2020 revised comprehensive diagnostic criteria for IgG4-RD [13] recommend the inclusion of clinical and radiological features (one or more organs show diffuse or localized swelling or a mass or nodule characteristic of IgG4-RD), serum IgG4 levels greater than 135 mg/dL, and pathological diagnosis.
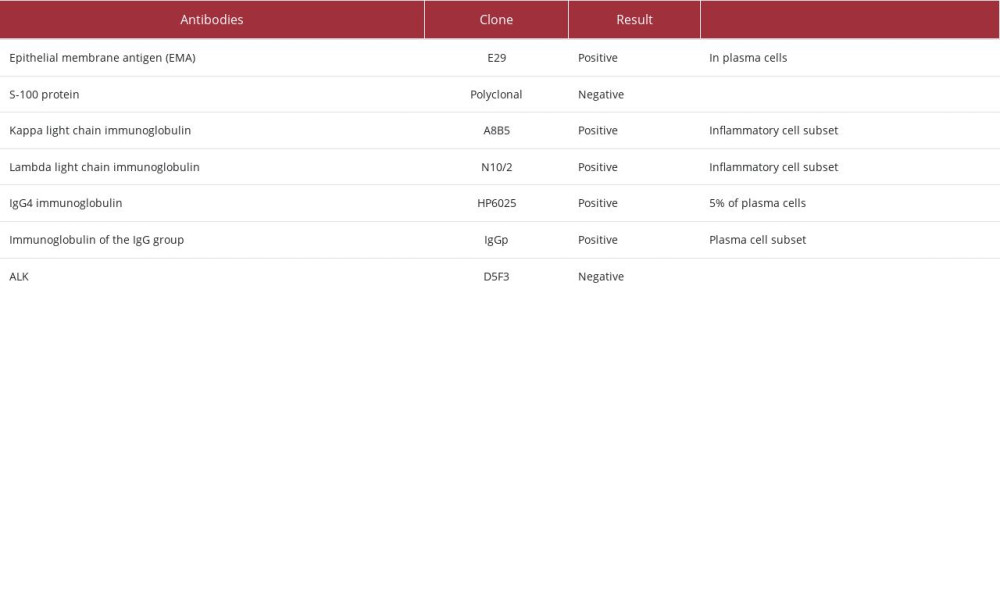
The diagnosis of IgG4 deposition disease was made based on the radiological findings, the elevated serum levels of IgG4, and the results of anatomopathological and immunohisto-chemical studies of the meningeal biopsy acquired intraoperatively (Figure 4). The immunohistochemical study revealed, in the infiltrate, polyclonal expression of light chains of kappa and lambda immunoglobulins. The IgG/IgG4 ratio was 5%; normal reference range is below 5%. The set of findings was consistent with inflammatory pseudotumor.
Histological analysis showed fragments with proliferation of elongated cells without atypia, with the appearance of reactive myofibroblasts, forming fascicles and with areas in a storiform pattern. In between, we observed an intense lymphoplasmacytic infiltrate without atypia, sometimes forming aggregates. Collections of xanthomatous histiocytes were also seen. Immunohistochemical analysis revealed polyclonal expression for kappa and lambda immunoglobulin chains. Individual results for each marker are summarized in Table 1.
Image staging was performed to estimate the extent of the disease involvement. Furthermore, our patient received oral treatment with corticosteroids for approximately 3 months with significant improvement. Currently, his care consists of rituximab every 6 months and regular followup with the otolaryngologist. Routine imaging did not reveal significant changes and the patient is currently maintaining a good quality of life.
The patient’s left hearing was rehabilitated with the adoption of a hearing aid, which provides normal hearing thresholds in its functional gain. He has been using the device systematically and shows satisfaction with the results.
Discussion
IgG4-RD is still a complex and unfamiliar disease, as the clinical features may involve multiple medical fields and some of the symptoms are indeed very common, like cough and dry mouth. It is fundamental that multidisciplinary teams are able to understand, recognize, and treat this disorder accordingly.
The exact prevalence of IgG4-RD is unknown, partly because it remains unfamiliar to many physicians and partly for its multiple differential diagnoses, as it can affect virtually every tissue in the body, resulting in multiple clinical presentations. Sjögren’s syndrome, for example, is a differential diagnosis, due to the involvement of salivary and lacrimal glands [7].
The most frequently reported symptoms are vague, such as hearing loss, otalgia, and headache [9], similar to the current case. Symptoms of asthma or allergies are present in approximately 40% of patients whereas vascular involvement has 15–25% rates and the aorta is the vessel most commonly affected [12]. Our patient, aside from cerebral thrombosis in the transverse and left sigmoid sinuses, also presented with respiratory allergies and developed pulmonary symptoms.
The serum IgG4 concentration is considered to have low specificity. Many disorders may also show high serum IgG4 concentrations, while some patients with IgG4-RD can have low levels of this antibody as well. Therefore, the histopathological study is the basis for the diagnosis, along with immunohistochemical features [14]. Obliterative phlebitis, bands of storiform fibrosis, and inflammatory infiltrate can be seen in the histological analysis and corroborate the diagnosis [15]. Our patient confirmed his diagnosis through meningeal biopsy and immunohistochemical analysis.
IgG4-RD has demonstrated a favorable responsiveness to glucocorticoids, although the iatrogenic toxicity associated with prolonged steroid therapy and relapses represent relevant long-term clinical concerns. As an effective alternative strategy to induce remission, rituximab is increasing in use [16]. In more recent studies, mizoribine, an immunosuppressive drug, showed reduced exacerbation in patients with multiple organ involvement, and may therefore be a potential treatment alternative for the future [17].
Once the diagnosis is confirmed, it is important to evaluate the extent of the disease with imaging, such as CT scans of the chest, abdomen, and pelvis due to the frequency of subclinical disease in these areas [18]. The infiltration of IgG4 plasma cells into the involved organs, one of the pathological features of IgG4-RD, causes enlargement of the affected organs [19]. Early recognition and treatment are fundamental to avoid progression to an inflammatory stage of poorly responsive fibrotic disease. A good initial therapeutic response to corticosteroids is expected [12], and the steroids can be accompanied by other drugs like monoclonal antibodies, as was instituted in this case. The baseline systematic review reported 22 cases with temporal bone involvement. Most patients were treated with corticosteroids±surgical intervention or an association of corticosteroids and immunosuppressors. The rate of symptom control and remission was 95.5% [9].
Considering the higher risk of malignancy in patients with the condition, especially in pancreatic and lymphoma forms, the treatment of choice in the case of early recognition is removal of the foci. Followup is essential to avoid complications, treat irresponsive stages, and prevent severe irreversible organ damage [20]. MRI has been shown to be preferential to CT scan in cases of bone destruction. This superiority is due to the greater enhancement of the lesion due to substantial lymphoplasmacytic infiltration [19]. As demonstrated in other cases with temporal bone involvement, imaging and systemic investigations can be insufficient to support a diagnosis [20]. To obtain samples for immunohistochemical investigation, surgery is also necessary for diagnostic purposes [9].
Conclusions
IgG4-RD remains a complex disease in its diagnosis and management. When there is temporal bone involvement, a surgical approach will be needed. Early recognition and surgical treatment are imperative to avoid complications and serious irreversible organ damage. The present report has presented a case of IgG4-RD of the left temporal bone, and highlights the approach to diagnosis and management, according to current guidelines.
Figures
References:
1.. Kamisawa T, Funata N, Hayashi Y, A new clinicopathological entity of IgG4-related autoimmune disease.: J Gastroenterol, 2003; 38(10); 982-84
2.. Hamano H, Kawa S, Horiuchi A, High serum IgG4 concentrations in patients with sclerosing pancreatitis: N Engl J Med, 2001; 344(10); 732-38
3.. Wallace ZS, Naden RP, Chari S, The 2019 American College of Rheumatology/European League Against Rheumatism classification criteria for IgG4-related disease: Ann Rheum Dis, 2020; 79(1); 77-87
4.. Masaki Y, Dong L, Kurose N, Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: Analysis of 64 cases of IgG4-related disorders: Ann Rheum Dis, 2009; 68(8); 1310-15
5.. Muraki T, Hamano H, Ochi Y, Autoimmune pancreatitis and complement activation system: Pancreas, 2006; 32(1); 16-21
6.. Wallace ZS, Deshpande V, Mattoo H, IgG4-related disease: Clinical and laboratory features in one hundred twenty-five patients: Arthritis Rheumatol, 2015; 67(9); 2466-75
7.. Hofauer B, Chaker A, Thürmel K, Knopf A, [Manifestations of autoimmune disorders in otorhinolaryngology: Classical symptoms and diagnostic approach.]: HNO, 2017; 65(8); 695-708 [in German]
8.. Barańska M, Makowska J, Wągrowska-Danilewicz M, Pietruszewska W, Supraglottic localization of IgG4-related disease-rare and challenging equity: J Pers Med, 2022; 12(8); 1223
9.. Oochit KK, Wong YY, Mihuna A, IgG4-related sclerosing disease of the temporal bone: A systematic review.: Otol Neurotol, 2022; 43(8); 856-63
10.. Barnado AL, Cunningham MA, IgG4-related disease presenting as recurrent mastoiditis with central nervous system involvement: J Investig Med High Impact Case Rep, 2014; 2(3) 2324709614553670
11.. Nilles C, Poillon G, Deschamps L, IgG4-related pachymeningitis and mastoiditis, associated with cerebral venous thrombosis: A case report: J Neuroimmunol, 2021; 360; 577717
12.. Moutsopoulos H, Fragoulis G, Stone J, Pathogenesis and clinical manifestations of IgG4-related disease, Waltham, Mass. UpToDate
13.. Umehara H, Okazaki K, Kawa S, The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD: Mod Rheumatol, 2021; 31(3); 529-33
14.. Carruthers MN, Khosroshahi A, Augustin T, The diagnostic utility of serum IgG4 concentrations in IgG4-related disease: Ann Rheum Dis, 2015; 74(1); 14-18
15.. Lanzillotta M, Della-Torre E, Wallace ZS, Efficacy and safety of rituximab for IgG4-related pancreato-biliary disease: A systematic review and meta-analysis: Pancreatology, 2021; 21(7); 1395-401
16.. Fukui S, Kawaai S, Nakai T, Effectiveness and safety of mizoribine for the treatment of IgG4-related disease: a retrospective cohort study: Rheumatology (Oxford), 2021; 60(12); 5697-704
17.. Moutsopoulos H, Fragoulis G, Stone J, Treatment and prognosis of IgG4-related disease., Waltham, Mass. UpToDate
18.. Yu T, Wu Y, Liu J, The risk of malignancy in patients with IgG4-related disease: A systematic review and meta-analysis: Arthritis Res Ther, 2022; 24(1); 14
19.. Hofmeyr L, Herbst G, Pretorius E, Case report: Diagnosis of petrous apex IgG4-related disease by middle cranial fossa craniotomy and temporal bone biopsy: Front Neurol, 2022; 13; 874451
20.. Chowsilpa S, Chowsilpa S, Teeranoraseth T, Roongrotwattanasiri K, Temporal bone involvement of IgG4-related disease: A rare condition misleading to petrous apicitis causing lateral rectus palsy: BMJ Case Rep, 2019; 12(2); e228550
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133