24 April 2023: Articles 
An Easily Missed But Life-Threatening Diagnosis: A Case Report of Gorlin Syndrome
Rare disease
Christoforos S. Kosmidis12AE, Christina Michael3ABCDEF*, Chrysi Maria Mystakidou3DF, Vasiliki Theodorou3CD, Evanthia Papadopoulou4BE, Konstantina Papadopoulou5F, Charilaos Koulouris12BC, Nikolaos Varsamis1DF, Georgios KoimtzisDOI: 10.12659/AJCR.939117
Am J Case Rep 2023; 24:e939117






Abstract
BACKGROUND: Gorlin syndrome, also known as basal cell nevus syndrome (BCNS), nevoid basal cell carcinoma syndrome (NBCCS), and Jaw cyst-Basal cell nevus-Bifid rib syndrome, is a rare multisystemic syndrome that can affect a remarkable number of tissues and organs in the human body. Patients with this syndrome are in jeopardy of developing basal cell skin cancer during puberty or early adulthood.
CASE REPORT: Herein, we report a case of a 58-year-old woman who had multiple pigmented skin lesions and a palpable tumor of the left scapula. The patient underwent surgical excision of the above-mentioned lesions. The histopathological examination revealed that 10 of them were basal cell skin carcinomas (BCCs); therefore, the patient was proven to have the syndrome. She had a history of similar skin lesions, which were removed before the age of 20.
CONCLUSIONS: This case highlights that rare phenomena, such as the presence of multiple BCCs, require additional investigations and a multidisciplinary approach since a rare and potentially life-threating condition might be the underlying cause. Early diagnosis of Gorlin syndrome is of paramount importance to facilitate the appropriate therapeutic approach, as directed by a multidisciplinary team. Patients with multiple skin lesions need to have regular assessments by their general practitioner or dermatologist, with dermoscopy serving as an important preventive measure. Furthermore, because pathogenesis of the syndrome is characterized by development of basal cell carcinomas, consecutive follow-up is of a great significance.
Keywords: Basal Cell Carcinoma, Multiple, case reports, Rare Diseases, Female, Humans, Adult, Middle Aged, Basal Cell Nevus Syndrome, Early Detection of Cancer, Carcinoma, Basal Cell, Skin Neoplasms, Pigmentation Disorders
Background
Gorlin syndrome was mentioned several times in the medical literature, but it was not until 1960 that Drs. Robert Gorlin and Robert Goltz outlined the disorder in detail [1]. The syndrome is characterized by a multiplicity of symptoms, including various basal cell carcinomas, accompanied by skeletal, ophthalmologic, neurologic symptoms, and neoplasms. Gorlin syndrome affects 1 in 40 000–60 000 people [2]. Due to the syndrome’s tendency to become aggressive and lead to development of malignant neoplasms, prompt diagnosis is the cornerstone of maximizing survival of affected patients.
Herein, we report a case of a woman with multiple skin lesions in more than 18 different sites. Following surgical excision, most of them were revealed to be basal cell carcinomas, and ultimately the patient was diagnosed with Gorlin syndrome.
Case Report
A 58-year-old patient visited our clinic due to multiple pigmented skin lesions and a palpable tumor of the left scapula (Figure 1).
Her medical history included hypertension treated with 150 mg of irbesartan, 5 mg of nebivolol, 5 mg of amlodipine, and 100 mg of acetylsalicylic acid, hypothyroidism treated with 125 μg of levothyroxine sodium, high LDL levels treated with 10 mg of rosuvastatin, poorly controlled and untreated type II diabetes mellitus, a 12-year history of rheumatoid arthritis treated with titrated dose of corticosteroids, and stage II neck and mediastinal nodular sclerosis Hodgkin’s lymphoma treated with 6 cycles of chemotherapy with adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD). The ABVD regimen is given on Day 1 and Day 15 and patients undergo 6 courses in total; each of them lasts 28 days [3]. Advantages of chemotherapy with ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) include low risk of late toxicity, absence of causing sterility, and induction of secondary neoplasms being low [4]. Moreover, the patient underwent excision of similar skin lesions before the age of 20 and had knee arthroplasty 8 years ago.
Following clinical assessment of her skin lesions and negative result of an examination for palpable lymph nodes, the patient was scheduled for surgical excision of the lesions under general anesthesia.
The patient’s preoperative chest X-ray revealed nodular opacification in the lower lung lobes and intensification of the interstitial pulmonary network. Her laboratory test results were largely unremarkable expect for a high glucose level of 163 mg/dl, mild neutrophilia of 80% (normal value: 40–75%), and lymphopenia of 14% (normal values: 20–40%).
The procedure was carried out with no intraoperative complications and the patient had an uneventful postoperative period and was discharged home on the first postoperative day. In total, more than 18 specimens were sent for histopathological examination. No chemotherapy or actinotherapy were given.
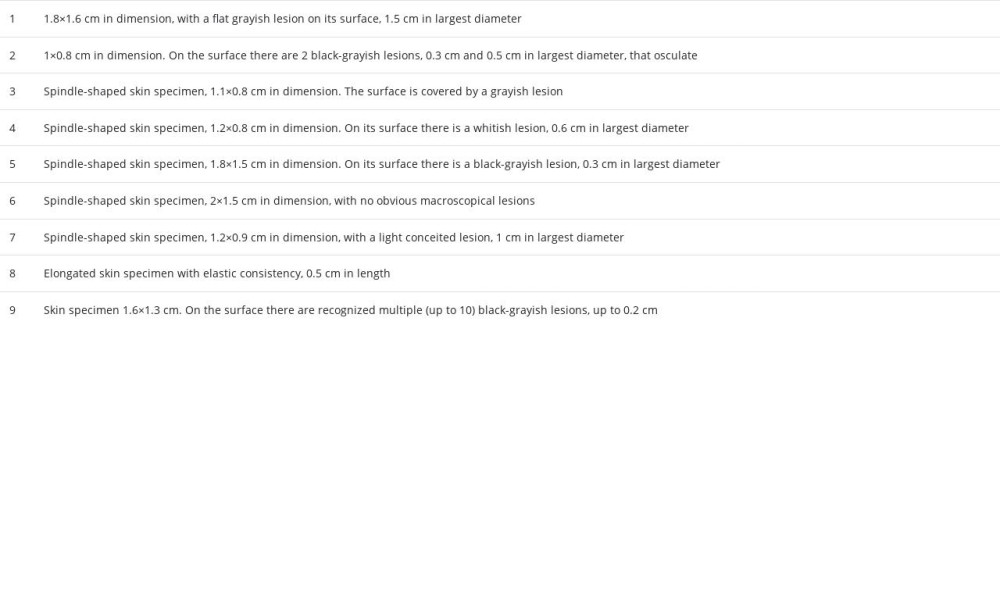
Histopathological examination confirmed that all specimens were excised with negative margins and revealed multiple basal cell skin carcinomas (BCCs) (Figure 2), seborrheic keratosis, dermal naevus, fibrous histiocytoma, and fibroma. Ten of them were compatible with BCCs. The lesion of the left scapula was confirmed to be a fibroma, with a maximum diameter of 9.5 cm, along with superficial BCCs measuring 5×2 cm. The specific characteristics of each BCC are portrayed in Table 1.
Following the histopathology report, the patient was referred to a multidisciplinary team (MDT) that recommended a sentinel lymph node biopsy, which revealed no evidence of metastasis. Moreover, following the MDT’s recommendations, a computed tomography (CT) scan of the thorax, abdomen, and retroperitoneal space and a bone nuclear scan were performed, which were also negative for any metastatic disease. Hence, no further treatment with chemotherapy or radiotherapy was advised. Based on the histopathological findings, paraclinical tests, and the patient’s history, the diagnosis of Gorlin syndrome was made.
Discussion
Gorlin syndrome is an infrequent genetic disorder that is inherited in an autosomal dominant pattern. The gene responsible for it is the tumor-suppressor gene PTCH, located in chromosome 9q, which encodes the patched-1 protein, a receptor whose ligand is a protein called Sonic Hedgehog [5]. Therefore, mutations of this gene can cause rampant and abnormal cell growth.
These mutations and therefore NBCCS can be inherited, new mutations account for approximately 50% of total cases. According to clinical testing done for the syndrome, to specify the clinical manifestations which are going to prognosticate positive test outcome, among 143 patients representing 106 unrelated pedigrees, 42 individuals were categorized as sporadic cases because either parents’ test results were negative or no family history was reported. Among those patients, more than half (54.8%) carry PTCH mutations. Results agree with other published estimations. Overall, the same source concludes that those pedigrees with multiple manifestations of the syndrome present greater possibility of having PTCH mutations. On the contrary, pedigrees who developed BCCs without any other features were less likely to test positive for PTCH mutations [6]. It is worth mentioning that “the two-hit hypothesis”, also known as “the Knudson hypothesis” was suggested as the genetic mechanism of the disease. Since PTCH is a tumor-suppressor gene, inactivation of both alleles is required for development of the syndrome.
Gorlin syndrome affects 1 in 40 000–60 000 people [1], distributed almost equally among men and women [7].
Clinical presentation of the syndrome involves a wide spectrum of cutaneous and extracutaneous symptoms and signs. Gorlin and Goltz came up with the classical triad of symptoms that characterizes this disorder: multiple basal cell carcinomas and keratocysts in the jaw and bifid ribs [8]. Other symptoms reported include epidermal cysts, the pathognomonic [9] calcified falx cerebri, hamartomas, pectus excavatum or carinatum, short 4th metacarpal, kyphoscoliosis, lumbarization of the sacrum, enlarged occipitofrontal circumference, which presents as macrocephaly and prominent forehead, spina bifida occulta, syndactyly, strabismus, medulloblastoma, meningioma, cardiac fibromas, and ocular hypertelorism [10,11].
BCCs are one of the most frequently encountered features of the syndrome, especially in the head and neck area [12]. Diagnosis of BCCs usually occurs at ages 40–79 [13], whereas BCCs in BCNS occur between adolescence and age 35 [7]. Exposure to sunlight is considered to be a risk factor for development of BCCs while it also affects their number [14], thus people need to avoid unnecessary ultraviolet (UV) radiation. Our patient developed multiple basal cell carcinomas principally in the dorsal part of the body; the subtypes of BCC which were encountered in this case were superficial, pigmented, and nodular.
In a study by Bartoš et al that collected data from 3 studies from the USA, Japan, and Australia, the presence of BCCs was associated with nationality and genetic background. BCCs were present in 78.9% of American people with light skin and 75% of the Australian people. On the other hand, BCCs were presented in only 38.4% of American people with dark skin and 37.8% of the Japanese people. The authors concluded that the phenotypic diversity presented can be explained by mutations of the PTCH gene and impact of the environment of each ethnic group [15].
Diagnosis of Gorlin syndrome requires, the presence of 2 major criteria or 1 major and 2 minor criteria or 1 major criterion and molecular confirmation [16]. Major criteria include >2 BCCs or 1 BCC before the age of 20, any odontogenic keratocyst proven by histology, at least 3 palmar or plantar cysts, calcified falx cerebri, and family history of the syndrome. Minor criteria include macrocephaly and protruding forehead, medulloblastoma, cardiac or ovarian fibroma, cleft lip or palate, polydactyly, skeletal abnormalities such as pectus deformity, anomalies of the eye such as cataract, coloboma, or microphthalmia, anomalies of the vertebral column, bridging of the sella turcica, and PTCH mutation [17]. In this article, we present a case that met the criteria of the syndrome: the patient has a history of BCCs before the age of 20, and had a first-degree relative (mother) with nevoid basal cell carcinomas. Genetic testing was advised by the oncology consult, but the patient was unable to proceed with it due to the cost of such a procedure. Although genetic testing is the criterion standard method for diagnosis of the syndrome [16], PTCH1 genetic testing is not a routine test, and it is only used in particular circumstances. Specifically, it is performed when confirmation of the diagnosis is needed in patients who do not meet the diagnostic criteria, in patients at risk who have family history but do not meet the criteria, and for prenatal testing when a mutation in the family is known [18]. Due to the patient’s medical history of NSHL and the treatment she received, there is a high probability of them being related. Nevertheless, according to the guidelines, the present case met the criteria and therefore it was a case of Gorlin syndrome.
Dermoscopy is considered to be an essential method for the differential diagnosis of skin lesions and is also helpful when selecting the area to be biopsied (Figure 3). This is important because NBCCS affects young people; therefore, dermoscopy not only restricts the number of biopsies but also prevents unnecessary surgical procedures [16].
No particular diagnostic laboratory test for NBCCs exists, but patients may present elevated levels of cyclic adenosine monophosphate and impaired phosphate diuresis during the parathormone test [19].
A multidisciplinary approach is essential for the treatment of the Gorlin syndrome due to the multiple tissues and organs affected. A multiplicity of treatments was suggested, yet no ideal approach has been found. Regarding treatment, basal cell carcinomas and keratocysts agree with the guidelines set for patients with these manifestations but not the syndrome. Invariably, therapy of BCCs using radiation should be eschewed since the development of BCCs is closely related to radiation.
Treatment options for BCCs include standard surgical excision, Mohs surgery, electrocoagulation, cryotherapy, laser ablation, photodynamic therapy, and topical chemotherapy [16,20]. Surgical excision – the criterion standard method of treatment [21] – is the most common method used for the removal of BCCs, especially when the lesions are restricted in number or are characterized by rapid growth [22]. It is worth mentioning that, according to the medical literature, removal of BCCs is advised to be performed with a margin of 3–4 mm [23]. Mohs surgery is selected as the best alternative in cases of tumors either located in high-risk zones or with regionally aggressive behavior [22]. Other treatment options mentioned above are useful when superficial or small-sized tumors occur [22]. In the present case, all lesions were removed by standard surgical excision within negative surgical margins.
In 2012, the United States Food and Drug Administration (FDA or USFDA) approved Vismodegib. This pharmacological agent is the first approved inhibitor of the Sonic Hedgehog (SHH) pathway. Vismodegib is suggested for locally advanced or metastatic BCC and for patients who cannot be treated surgically or with radiation [24].
Other frequently encountered skin abnormalities such as palmoplantar pits, basaloid follicular hamartomas, facial milia, and epidermoid cysts are considered to be benign and, although treatment is not needed, they have a crucial role in diagnosis of the syndrome [21].
It is advised that patients must be under close lifelong follow-up. Occasional dermatological examinations are vital for the early recognition of any recurrence [7]. It is recommended that follow-up for the BCCs should take place at least 3 or 4 times a year [19]. Neurological examination is needed twice a year, especially in younger children who are at high risk of developing medulloblastoma [19,25]. MRI of the brain is indicated in children aged 1 to 7 years old. Given that this is an inherited syndrome, genetic counselling should also be suggested [19]. In addition, depending on the signs or symptoms the patients may present, examination of the cardiac system can take place [25].
It is mandatory that these patients are closely monitored by an MDT due to the high risk of recurrence. Moreover, it is necessary to emphasize the importance of prevention. For those at high risk of the syndrome, apart from frequent assessments, simple preventive measures, such as avoidance of sun exposure, is crucial. Use of sunscreen should be discussed with the patient, since the development or recurrence of BCCs can be prevented in patients with Gorlin syndrome [21]. A high level of clinical suspicion is required, and expert assistance should be sought as soon as a suspicious lesion is noted by the patient or the responsible clinician.
Conclusions
In the present article, we describe the case of a rare syndrome that involves pathology of several tissues of the human body. Early diagnosis is vital for the treatment to be successful. Presence of multiple basal cell carcinomas suggests further investigation of the cause, while the diagnosis of Gorlin syndrome requires certain criteria to be met. Patients that might have the syndrome need to meet certain criteria. Existence of a first-degree relative is essential as well, but sporadic events can also occur.
Figures
References:
1.. Dodda VK, Taneeru S, Guttikonda VR, Gaddipati R, Nevoid basal cell carcinoma syndrome: A case report: J NTR Univ Health Sci, 2018; 3; 200-3
2.. Sanghera R, Grewal PS, Gorlin syndrome presentation and the importance of differential diagnosis of skin cancer: A case report: J Pharm Pharm Sci, 2018; 21; 222s-24s
3.. Collins G, ABVD, 2021 Available at: https://nssg.oxford-haematology.org.uk/lymphoma/documents/lymphoma-chemo-protocols/L-8%20-%20abvd.pdf
4.. Domínguez AR, Márquez A, Gumá J, Treatment of stage I and II Hodgkin’s lymphoma with ABVD chemotherapy: Results after 7 years of a prospective study: Ann Oncol, 2004; 12; 1798-804
5.. , Gorlin syndrome: MedlinePlus Genetics [online] Medlineplus.gov. Available at: [Accessed 26 August 2022].https://medlineplus.gov/genetics/condition/gorlin-syndrome
6.. Klein RD, Dykas DJ, Bale AE, Clinical testing for the nevoid basal cell carcinoma syndrome in a DNA diagnostic laboratory: Genet. Med, 2005; 9; 611-19
7.. Kim CS, Na YC, Basal cell nevus syndrome with excessive basal cell carcinomas: Arch Craniofac Surg, 2021; 22; 122-25
8.. Pandeshwar P, Jayanthi K, Mahesh D, Gorlin-Goltz syndrome: Case Rep Dent, 2012; 2012; 247239
9.. Shrivastava S, Nayak S, Nayak P, Sahu S, Gorlin syndrome: A rare case report: J Oral Maxillofac Pathol, 2020; 24; 591
10.. Scully C, Langdon J, Evans J, Marathon of eponyms: 7 Gorlin-Goltz syndrome (Naevoid basal-cell carcinoma syndrome): Oral Dis, 2010; 16; 117-18
11.. Kiwilsza M, Sporniak-Tutak K, Gorlin-Goltz syndrome – a medical condition requiring a multidisciplinary approach: Med Sci Monit, 2012; 18(9); 145-53
12.. Casaroto AR, Ferraz DRL, Moreschi E, Early diagnosis of Gorlin-Goltz syndrome: case report: Head Face Med, 2011; 7; 2
13.. Ciążyńska M, Narbutt J, Woźniacka A, Lesiak A, Trends in basal cell carcinoma incidence rates: A 16-year retrospective study of a population in central Poland: Postepy Dermatol Alergol, 2018; 35(1); 47-52
14.. Jones AE, Sajid MI, Shenton A, Evans DG, Basal cell carcinomas in gorlin syndrome: A review of 202 patients: J Skin Cancer, 2011; 2011; 217378
15.. Bartoš V, Kullová M, Adamicová K, Paučinová I, Gorlin-Goltz syndrome: Klin Onkol, 2019; 32(2); 124-28
16.. Binsheikhan S, Mittal S, Al Abadie M, Nevoid basal cell carcinoma syndrome (Gorlin syndrome) in Children: Eur J Med Sci, 2021; 5; 15-17
17.. Veenstra-Knol HE, Diagnostic criteria for Gorlin syndrome (or nevoid basal cell carcinoma syndrome, NBCCS): Eur J Pediatr, 2005; 164; 126-30
18.. Spiker AM, Troxell T, Ramsey ML: Gorlin syndrome, 2022, Treasure Island (FL), StatPearls Publishing
19.. Manzi G, Magli A, Pignalosa B, Liguori G, The Gorlin-Goltz syndrome: Case report: Ophthalmologica, 1990; 200; 104-46
20.. Palakkal S, Celine MI, Vineetha M, Sobhanakumari K, Gorlin syndrome – a case report: J Skin Sex Transmitted Dis, 2019; 1; 104-6
21.. Verkouteren BJA, Cosgun B, Reinders MGHC, A guideline for the clinical management of basal cell naevus syndrome (Gorlin-Goltz syndrome): Br J Dermatol, 2022; 186(2); 215-26
22.. Barankin B, Lam JMC, Nevoid basal cell carcinoma syndrome (Gorlin syndrome) 2022 Retrieved from Up To Date: https://www.uptodate.com/
23.. Smith V, Walton S, Treatment of facial basal cell carcinoma: A review: J. Skin Cancer, 2011; 2011; 7
24.. Zito PM, Nassereddin A, Scharf R, 2022, Treasure Island (FL), StatPearls Publishing
25.. Rao A, Taksande A, A case of Gorlin-Goltz syndrome presented with multiple odontogenic keratocysts in the jaw without skin manifestation: Cureus, 2022; 14; e24666
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133