26 April 2023: Articles 
Rare Case of Remitting Seronegative Symmetrical Synovitis with Pitting Edema Syndrome with Monoclonal Gammopathy of Undetermined Significance
Challenging differential diagnosis, Rare disease
Alpana GargDOI: 10.12659/AJCR.939650
Am J Case Rep 2023; 24:e939650






Abstract
BACKGROUND: Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is a rare condition with underlying polyarthritis, pitting edema, and negative rheumatoid factor. It can be associated with an underlying rheumatological condition or can present as a paraneoplastic syndrome with malignancy. We present a rare case of RS3PE associated with monoclonal gammopathy of undermined significance (MGUS).
CASE REPORT: A 62-year-old man presented in ambulatory medicine clinic with 3-month swelling of distal lower extremities that progressed to distal upper extremities. He had pain and morning stiffness in hands, left elbow, and left shoulder. Examination revealed 3+ pitting edema in bilateral hands, feet, legs, and thighs. Laboratory studies revealed normal blood counts and renal and liver functions. Erythrocyte sedimentation rate was normal; C-reactive protein was mildly elevated (0.7 mg/dL). Echocardiogram and computed tomography of chest, abdomen, and pelvis revealed mild splenomegaly (14.5 cm). Serum protein electrophoresis revealed IgG kappa monoclonal peak of 0.1 g/dL. Beta-2 microglobulin was elevated (7.4 mg/L); LDH was elevated (264 U/L). No lytic lesions were present in bones. RS3PE was diagnosed based on established diagnostic criteria. Prednisone produced significant improvement in swelling within 72 h of start; however, he required a longer duration of steroid treatment due to relapse and continued periodic MGUS surveillance.
CONCLUSIONS: Our case highlights the importance of awareness of this condition in general practice to help with timely diagnosis and intervention, as this condition is steroid responsive. Also, it is important to screen for underlying autoimmune condition, hematological, and solid organ malignancies with appropriate workup.
Keywords: Edema, monoclonal gammopathy of undetermined significance, Paraproteinemias, Male, Humans, Middle Aged, synovitis, Arthritis, Prednisone, Antibodies, Monoclonal
Background
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is a rare condition with underlying polyarthritis, pitting edema, and negative rheumatoid factor [1–4]. It can be associated with an underlying rheumatological condition or can present as a paraneoplastic syndrome with malignancy [4]. It is a heterogeneous condition that affects the elderly and is twice as common in men than women [4]. RS3PE has been associated with solid organ malignancies; however, it is rare to find it associated with an underlying monoclonal gammopathy of undetermined significance (MGUS). Here, we present a rare case of RS3PE with underlying MGUS.
Case Report
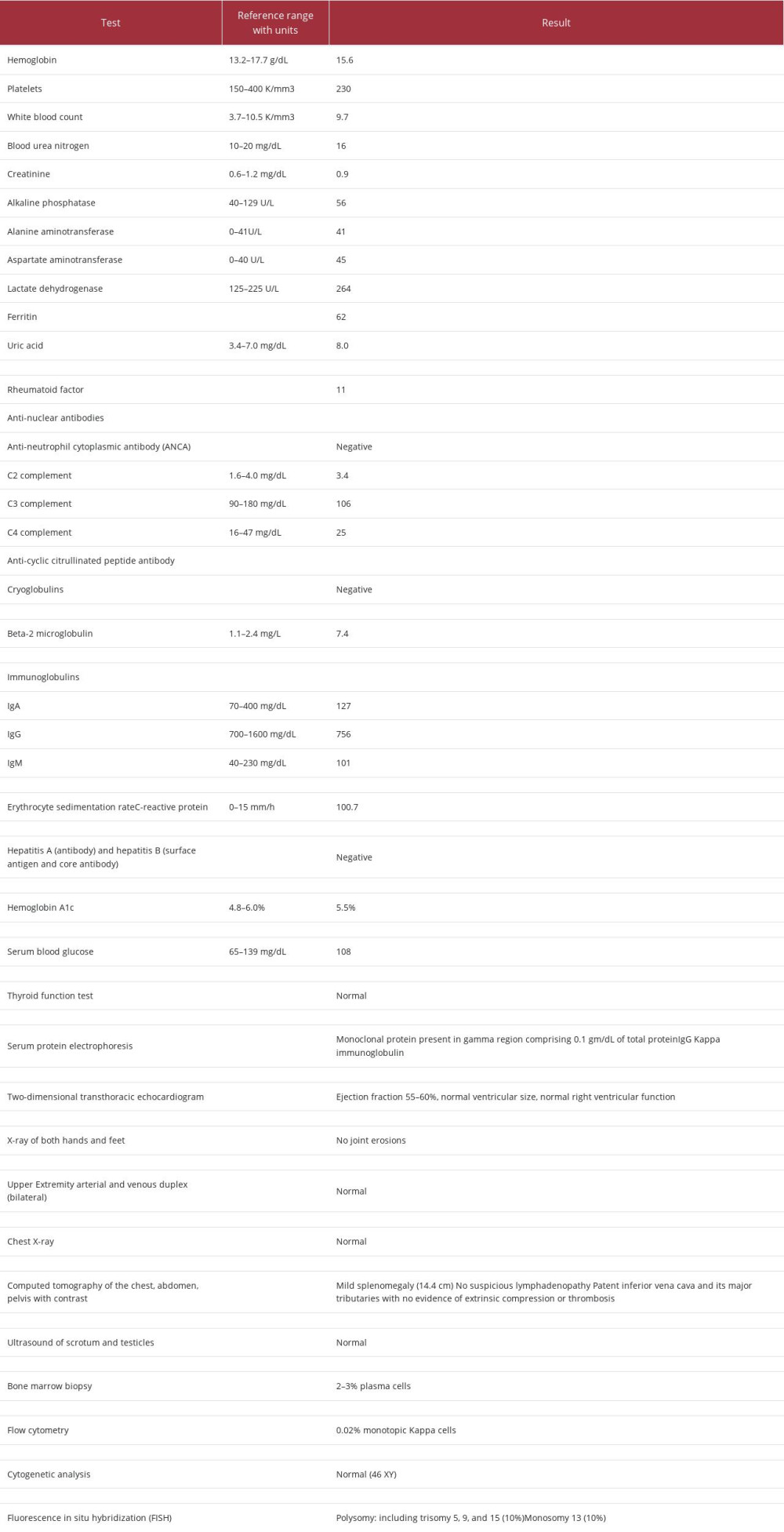
A 62-year-old man presented with 3 months of generalized swelling. He first noticed feet swelling at the onset, with progression to knee and leg swelling 1 month later. He further developed hand swelling, which progressively worsened and was associated with pain. The pain and swelling, particularly in the hands, was severe enough to interfere with sleep and affected quality of life. Other associated symptoms included left arm soreness and left shoulder stiffness. He endorsed morning stiffness in the ankles and knees, which improved with activity after 30 min and completely resolved after 2 h. He also reported stiffness with prolonged sitting, which improved with walking. He denied any fevers, chills, night sweats, fatigue, decreased appetite, hair loss, rash, photosensitivity, Raynaud’s phenomenon, headache, dry eye, vision changes, diplopia, nasal ulcers, epistaxis, dry mouth, oral ulcers, cough, shortness of breath, hemoptysis, chest pain, difficulty swallowing, nausea, vomiting, diarrhea, constipation, urinary symptoms, hematuria, easy bruising, or bleeding. The patient’s history was significant for a 30-pack-year smoking history, with smoking cessation at age 40 years. On presentation, he was afebrile, with a pulse of 73 beats per min, blood pressure of 117/72 mmHg, and body mass index of 28.95 kg/m2. Physical examination was notable for 3+ pitting edema in the bilateral hands, feet, and legs, extending past the knees (Figure 1A–1C). Evaluation for synovitis in the small joints of the hands was limited by extensive edema. His metacarpophalangeal joints were boggy, and he was unable to make a fist owing to swelling. Investigations and diagnostic tests (Table 1), including renal function, hepatic function, electrolytes, complete blood count with differential, thyroid stimulating hormone, thyroxine, N-terminal pro-brain natriuretic peptide, urinalysis with microscopic analysis, and urine random protein, were all within normal limits. The erythrocyte sedimentation rate was within normal limits, and the C-reactive protein level was mildly elevated at 0.7 mg/dL. The total serum protein level was slightly elevated at 5.7 g/dL, and the albumin level was normal (3.2 g/dL). Serum protein electrophoresis revealed a monoclonal protein present in the gamma region, comprising 0.1 g/dL of the total protein. Because the presence of bilateral symmetric edema in the upper and lower extremities with associated pain in the hands was concerning for active synovitis, rheumatologic and autoimmune testing was performed. The rheumatologic workup was notable for a negative rheumatoid factor; the full workup is shown in Table 1. The uric acid level was elevated at 8.0 mg/dL; however, a diagnosis of gout was felt to be unlikely given the polyarticular presentation and the absence of severe pain and redness. Repeat uric acid levels at follow-up were normal. Transthoracic echocardio-gram revealed normal left ventricular systolic function, without any significant valvular abnormalities. Given the concern for underlying malignancy, computed tomography of the chest, abdomen, and pelvis with contrast was obtained, revealing a patent inferior vena cava, without evidence of extrinsic compression or thrombosis, and mild splenomegaly (14.5 cm). No suspicious lesions, lymphadenopathy, or skeletal lesions were present. He was referred to the Hematology and Oncology Department, owing to the paraproteinemia and elevated beta-2 microglobulin. He was evaluated further with bone marrow biopsy, which was suggestive of normocellular bone marrow (40–50%) and plasma cells (2–3%) and was negative for Congo red staining. Other test results, including flow cytometry of peripheral blood and fluorescent in situ hybridization (FISH), are shown in Table 1. Due to worsening joint pains and edema, with minimal improvement with diuretic furosemide, the patient was referred to the Rheumatology Department for evaluation of an underlying inflammatory condition.
Based on a 3-month history of slowly progressive pitting edema initially in the distal lower extremities and subsequently in the hands and distal upper extremities that was combined with morning stiffness and gelling phenomenon, which is consistent with inflammatory arthritis, a diagnosis of RS3PE was made. MGUS was diagnosed because the level of paraprotein was low at <30 g/L, bone marrow plasma cells were <10%, and there was an absence of myeloma-related organ or tissue damage (renal, skeletal, or bone marrow impairment) [5]. The patient was started on prednisone 60 mg daily and had an excellent response (Figure 1D). There was dramatic improvement in swelling within 72 h. The patient reported 50% improvement with the first dose of steroid and 90% improvement with the second dose. His weight decreased from 219 pounds to 207 pounds. Prednisone 60 mg daily was given for 2 weeks, followed by 40 mg daily for 2 weeks, followed by 30 mg daily for 2 weeks, and 20 mg daily for 2 weeks. After completing this regimen for 2 months, the patient endorsed the return of symptoms, with worsening of joint pains and swelling, and another course of prednisone with a slower taper was given. He was also referred for age-appropriate cancer screening, which included colonoscopy and the checking of prostate cancer antigen levels (which were normal). Further, it was recommended by Oncology that he follow up annually for MGUS surveillance, but further fat pad biopsy for amyloid was deemed to be low yield (which would not change management of patient care) and was not performed.
Discussion
We report a rare case of RS3PE with underlying MGUS. To the best of our knowledge, only 1 other case has been reported, which was in a retrospective study by Tezcan et al [6]. The authors reported 15 cases of RS3PE with different comorbidities, of which 1 patient, an 86-year-old man, had MGUS and pitting edema of the ankles [6].
RS3PE is a rare elderly-onset disease that was initially described by McCarty et al in 1985; it can be associated with neoplasia and considered a paraneoplastic rheumatic disease [3]. Although its underlying pathophysiology is not very well understood, it has been increasingly associated with elevations in vascular endothelial growth factor (VEGF) and matrix metalloproteinase 3 [7,8]. The level of VEGF was found to be higher in patients with RS3PE than in patients with rheumatoid arthritis or even healthy adults [9,10]. It is also associated with immune checkpoint inhibitor use and certain infections, like parvovirus B19 [11,12]. Cases of RS3PE have also been reported after the administration of medications and vaccination [13–15].
For diagnosis of RS3PE, the following diagnostic criteria were proposed by Olivo et al: (1) painful edema of the distal extremities, (2) acute onset, (3) negative rheumatoid factor and nonerosive arthritis, and (4) age >50 years [2]. In addition to performing a workup to look for other rheumatological conditions, such as rheumatoid arthritis and polymyalgia rheumatica, it is important to look for any evidence of an occult tumor, as it can be a first presentation of underlying malignancy [16,17].
It is important to highlight that RS3PE is extremely steroid-responsive, especially when there is no concomitant malignancy. Small doses of glucocorticoids have been shown to rapidly improve the clinical symptoms. However, a slow taper is required in many cases, as there is risk of frequent relapses, as happened in the present case. Long courses of steroids, at 1-year follow-up, were shown to be associated with higher risk of infections when patients with R3SPE were compared with patients with rheumatoid arthritis [18]. In addition to steroids, tocilizumab has been used for treatment, especially in steroid-resistant cases [19].
Our case of RS3PE is unique since an underlying MGUS was found; the importance of both together is unknown, as it is a rare entity. Overall, MGUS requires no therapy, and the risk of progression to myeloma is 1% per year [5]. The clinical course of RS3PE is highly variable, and follow-up data is limited in the published literature. In a retrospective study that included 13 elderly patients and followed the patients for 3 to 172 months, 6 patients were later found to have another connective tissue or inflammatory rheumatic disease, such as polymyalgia rheumatic or spondyloarthropathy [20]. It is also important to screen for cancers, as underlying associations with malignancies have been described, including hematological, solid organ, and genitourinary cancers. A study investigated the outcomes of 41 patients with RS3PE; at 1-year follow-up, 82.9% were receiving prednisone and 34.1% were diagnosed with neoplasm [21]. Of the neoplasms, 3 had gastric cancer, 5 had colon cancer, 4 had lung cancer, 1 had breast cancer, and 1 had prostate cancer. Most of these cancers occurred within 2 years of diagnosis of RSPE, with 1 patient dying from lung cancer at 1 year after diagnosis. Remission of RS3PE was induced in all 41 patients, with 7 of these patients developing relapsing disease during their first year [21]. We plan to follow our patient in the Primary Care Clinic for age-appropriate cancer screening and in the Hematology-Oncology Clinic annually for routine surveillance for MGUS.
Conclusions
MGUS in the setting of RS3PE is a rare entity. Our case highlights the importance of awareness of this condition in general practice to help with timely diagnosis and intervention, as RS3PE is responsive to steroid treatment. Also, it is important to screen for underlying autoimmune conditions and hemato-logical and solid organ malignancies with appropriate workup.
References:
1.. Lakhmalla M, Dahiya DS, Kichloo A, Remitting seronegative symmetrical synovitis with pitting edema: A review: J Investig Med, 2021; 69(1); 86-90
2.. Olivo D, D’Amore M, Lacava R, Benign edematous polysynovitis in the elderly (RS3PE syndrome): Clin Exp Rheumatol, 1994; 12(6); 669-73
3.. McCarty DJ, O’Duffy JD, Pearson L, Hunter JB, Remitting seronegative symmetrical synovitis with pitting edema. RS3PE syndrome: JAMA, 1985; 254(19); 2763-67
4.. Karmacharya P, Donato AA, Aryal MR, RS3PE revisited: A systematic review and meta-analysis of 331 cases: Clin Exp Rheumatol, 2016; 34(3); 404-15
5.. Cook L, Macdonald DH, Management of paraproteinaemia: Postgrad Med J, 2007; 83(978); 217-23
6.. Tezcan D, Gülcemal S, Limon M, Yilmaz S, Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome: A single-center experience: J Contemp Med, 2021; 11; 804-10
7.. Arima K, Origuchi T, Tamai M, RS3PE syndrome presenting as vascular endothelial growth factor associated disorder: Ann Rheum Dis, 2005; 64(11); 1653-55
8.. Origuchi T, Arima K, Kawashiri SY, High serum matrix metalloproteinase 3 is characteristic of patients with paraneoplastic remitting seronegative symmetrical synovitis with pitting edema syndrome: Mod Rheumatol, 2012; 22(4); 584-88
9.. Kenzaka T, The Relationship between remitting seronegative symmetrical synovitis with pitting edema and vascular endothelial growth factor and matrix metalloproteinase 3: Intern Med, 2020; 59(8); 1021-22
10.. Kenzaka T, Goda K, Serum matrix metalloproteinase 3 in detecting remitting seronegative symmetrical synovitis with pitting edema syndrome: A case report: World J Clin Cases, 2018; 6(5); 84-87
11.. Yamamoto S, Fujita S, Mukai T, Paraneoplastic remitting seronegative symmetrical synovitis with pitting edema syndrome should be treated with low-dose prednisolone during pembrolizumab therapy: Intern Med, 2020; 59(4); 597-98
12.. Wada N, Uchi H, Furue M, Case of remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome induced by nivolumab in a patient with advanced malignant melanoma: J Dermatol, 2017; 44(8); e196-e97
13.. Law J, Nauka PC, Nguyen A, LeFrancois D, Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) associated with DPP-4 inhibitor: Am J Med, 2021; 134(7); e412-e14
14.. Sawamura T, Karashima S, Ohmori A, Remitting seronegative symmetrical synovitis with pitting edema syndrome worsen after the administration of dulaglutide: Medicina (Kaunas), 2022; 58(2); 289
15.. Parperis K, Constantinou M, Remitting seronegative symmetrical synovitis with pitting oedema following BNT162b2 mRNA COVID-19 vaccination: BMJ Case Rep, 2021; 14(8); bcr-2021-244479
16.. Ferrao C, Faria RM, Farrajota P, Vasconcelos C, Lucky to meet RS3PE: BMJ Case Rep, 2013; 2013; bcr-2013-010363
17.. Matsuoka H, Matsubara H, Sugimura A, Remitting seronegative symmetrical synovitis with pitting edema syndrome complicated with primary lung cancer: Int Cancer Conf J, 2017; 6(1); 16-21
18.. Origuchi T, Umeda M, Koga T, Comparison of complications during 1-year follow-up between remitting seronegative symmetrical synovitis with pitting edema syndrome and elderly-onset rheumatoid arthritis: Immunol Med, 2022; 45(3); 168-74
19.. Sato H, Yamada S, Muraoka S, Masuoka S, Treatment of refractory RS3PE syndrome with tocilizumab: J Clin Rheumatol, 2021; 27(8S); S814
20.. Berthier S, Toussirot E, Wendling D, [Acute benign edematous polyarthritis in the elderly (or RA3PE syndrome). Clinical course apropos of 13 cases.]: Presse Med, 1998; 27(34); 1718-22 [in French]
21.. Origuchi T, Arima K, Umeda M, Clinical outcomes in the first year of remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome: Mod Rheumatol, 2017; 27(1); 150-54
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133