12 July 2023: Articles 
Parvovirus B19 Infection: A Vasculitis Masquerade in an Elderly Patient
Unusual clinical course, Mistake in diagnosis, Diagnostic / therapeutic accidents, Unusual setting of medical care, Educational Purpose (only if useful for a systematic review or synthesis)
Morika Suzuki1ABCDEFG, Takashi WatariDOI: 10.12659/AJCR.939696
Am J Case Rep 2023; 24:e939696






Abstract
BACKGROUND: The profound ability of viral infections to convincingly mimic vasculitis, thereby pathologically influencing vessels of any caliber, is undeniably significant. Notably, adult patients with B19V infection frequently experience joint pain and cutaneous eruptions, which are ostensibly immune responses to the infection and necessitate careful differentiation from autoimmunity. Conversely, vasculitis syndromes represent an amalgamation of diseases characterized by vascular inflammation, predominantly classified based on the impacted vessels’ size and location. Although the expedited diagnosis and therapeutic management of vasculitis are paramount, many conditions, including infectious diseases, can potentially masquerade as vasculitis, necessitating rigorous differential diagnosis.
CASE REPORT: A 78-year-old male patient presented with fever, bilateral leg edema, skin rash, and foot numbness to the outpatient department. Blood investigations showed elevated inflammatory parameters, and urinalysis showed proteinuria and occult blood presence. We considered SVV, particularly microscopic polyangiitis, which causes acute renal injury, as the provisional diagnosis. Blood investigations, including auto-antibodies and a skin biopsy, were performed. However, his clinical symptoms resolved spontaneously before these investigation results were reported. Subsequently, the patient was diagnosed with B19V infection based on B19V immunoglobulin M antibody positivity.
CONCLUSIONS: B19V infection mimics vasculitis. Even in geriatric patients, particularly during B19V infection outbreaks, clinicians should conduct thorough interviews and examinations while contemplating the likelihood of B19V infection as a potential vasculitis mimic.
Keywords: Aged, livedo reticularis, Microscopic polyangiitis, Parvovirus B19, Human, Adult, Male, Humans, Erythema Infectiosum, Exanthema, Vasculitis, Acute Kidney Injury, Immunoglobulin M
Background
Human parvovirus B19 (B19V) infection causes erythema infectiosum in children. However, the virus triggers many systemic manifestations, including cutaneous eruptions and arthralgia in adults; although these symptoms are somewhat atypical of erythema infectiosum, they are frequently superseded by predominant arthropathy, particularly in women [1]. The detailed mechanism responsible for this phenomenon is unknown [2]; however, the manifestation of erythema infectiosum and arthropathy are conjectured to result from the formation and subsequent deposition of immune complexes [1]. The characteristic B19V facial rash observed in children is rarely found in adults [3,4]. Additionally, B19V-induced post-infection acute glomerulonephritis can cause renal damage, albeit this consequence is relatively uncommon [5]. From a diagnostic perspective, B19V-associated arthralgia, skin rash, and nephropathy with fever in adults should be differentiated from autoimmune conditions. However, the immune response elicited by B19V infection could produce false-positive auto-antibodies, creating potential misidentification of B19V infection as an auto-inflammatory disorder [6,7]. Therefore, it is crucial to diagnose vasculitis promptly. Moreover, since various diseases can mimic the condition, differentiation from other entities is required. Infection can mimic vasculitis and affect vessels of any size. Viral infections, such as those caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), hepatitis B and C viruses, and HIV are known to mimic vasculitis [7]. However, the clinical manifestations of small vessel vasculitis (SVV) vary and can include systemic symptoms, such as fever and malaise, skin rashes, peripheral neuropathic symptoms due to tissue hemorrhage, and ischemia. Therefore, a differential examination is critical. Microscopic polyangiitis (MPA) is hypothesized to be SVV that is caused by an autoimmune abnormality involving antineutrophil cytoplasmic antibody (ANCA), although its definitive cause is unknown [8–10]. Renal involvement is the most common manifestation of severe MPA, and an early diagnosis is crucial because of the possibility of rapid progression and transition to end-stage renal failure [9].
Therefore, we report a case of B19V infection in an older adult patient who presented with typical SVV-like symptoms (fever, bilateral leg edema, skin rash, and numbness in the feet) but whose symptoms eventually resolved spontaneously.
Case Report
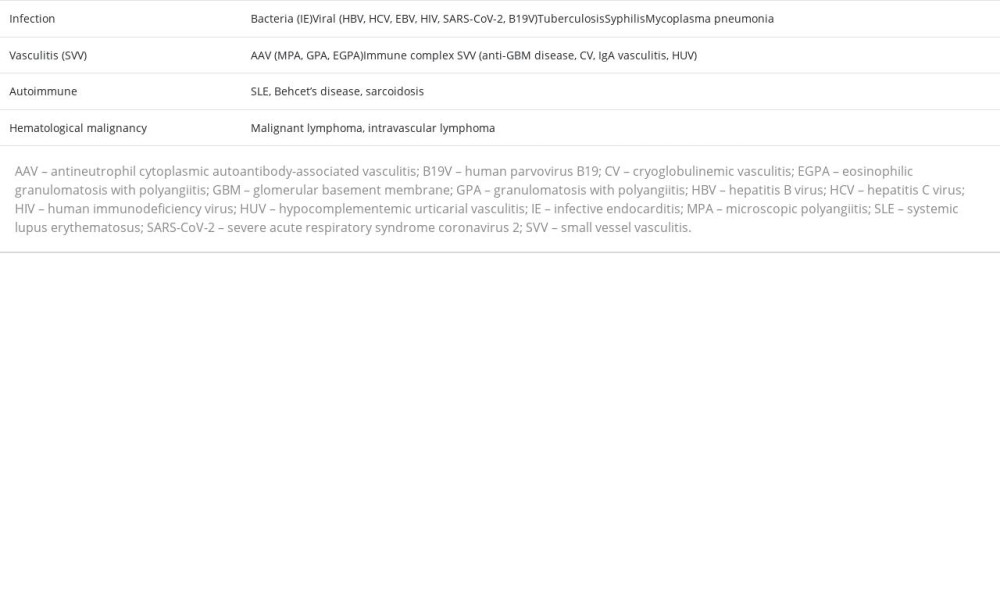
DIFFERENTIAL DIAGNOSES:
We considered the following differential diagnoses based on the patient’s key clinical complaints: severe bacterial infection (infective endocarditis), viral infections (HIV, hepatitis B, hepatitis C, Epstein-Barr virus, SARS-CoV-2, and B19V), tuberculosis, syphilis, mycoplasma pneumonia, autoimmune diseases (systemic lupus erythematosus, Behcet’s disease, and sarcoidosis), and hematologic malignancies (malignant and intravascular lymphomas) (Table 1).
INVESTIGATIONS:
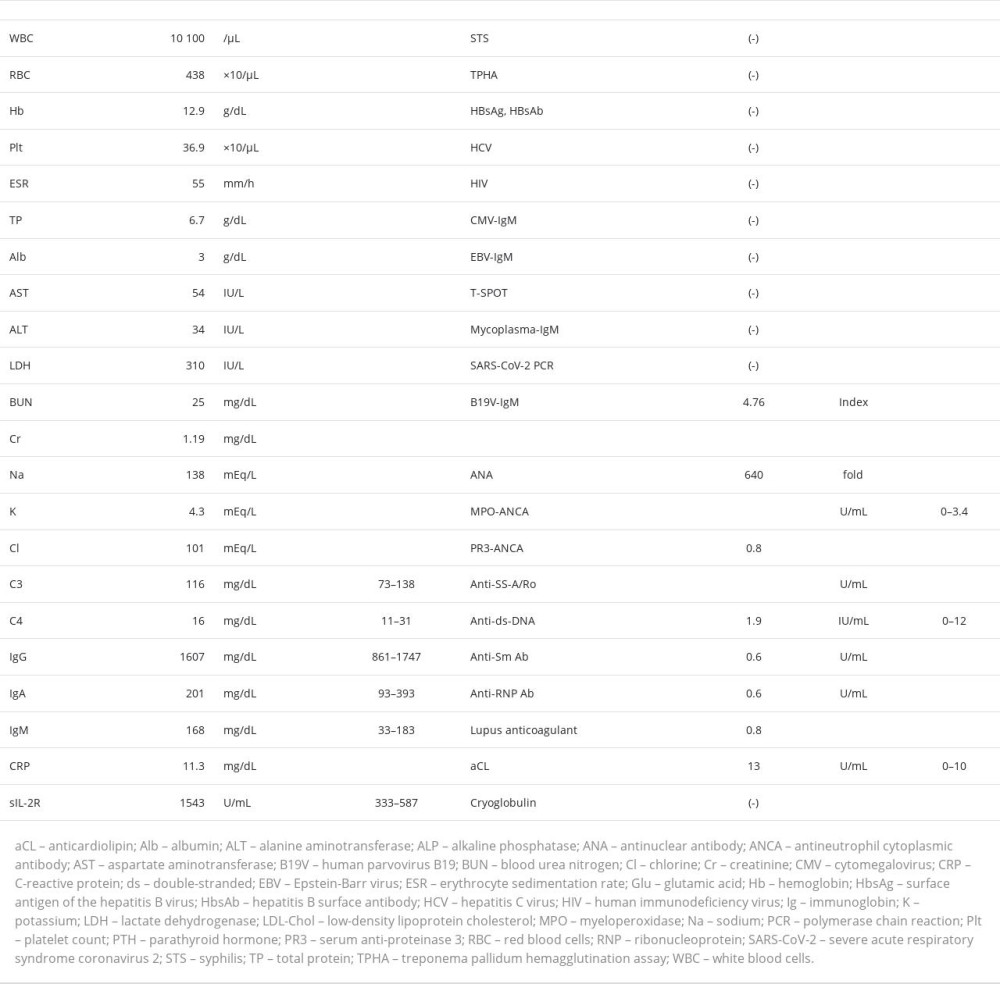
Blood tests showed an elevated inflammatory response (white blood cell count, 10 100/μL; C-reactive protein level, 11.3 mg/dL; and erythrocyte sedimentation rate, 55 mm/h), mild anemia (red blood cell count, 483×103 cells/μL and hemoglobin, 12.9 mg/dL), and renal dysfunction (blood urea nitrogen, 25 mg/dL and creatinine, 1.19 mg/dL). We examined the patient for viral infections, and all test results except B19V-immunoglobulin M (IgM) were negative. Furthermore, cryoglobulin tested negative. His antinuclear antibody titer was 640-fold; however, test results for myeloperoxidase-ANCA and proteinase 3-ANCA were negative (Table 2).
The urinalysis results were positive for protein (2+) and occult blood (2+). Microscopic examination revealed 5 to 9 erythrocytes per field of view and no obvious morphological abnormalities. The protein/creatinine ratio was 0.43 g/g.Cr (reference value, <0.15), indicating mild proteinuria.
Urine and blood cultures were negative for any microbial growth. Imaging studies showed no lymphadenopathy, hepatosplenomegaly, or possible focus of infection that could have caused the fever. Skin biopsies performed at the site of the livedo reticularis showed no sign of vasculitis or malignancy.
Three weeks after the onset of fever (hospitalization day 11), B19V-IgM by enzyme immunoassay was positive at 4.76 (negative, <0.8), and the diagnosis of acute B19V infection was confirmed.
TREATMENT:
The patient was treated with oral acetaminophen (400 mg) during febrile episodes, and no other treatment was administered. Furthermore, the patient fully recovered without complications.
Discussion
B19V infection is a globally recognized infectious disease [1,2,11]. The prevalence of B19V antibodies in adults increases with age, from 40% to 60% in young adults to approximately 85% to 90% in older people [1,3]. More than half of B19V cases in adults are acquired from children because of the infection of a household member [1,6,12]. The skin rash of a B19V infection is characterized by the typical “slapped cheek” in children but is less and more common on the face and lower legs, respectively, in adults [1,3,11]. Various cutaneous manifestations, including erythematous skin rash, purpura, and livedo reticularis, have been reported in adults with B19V infection [3,4]. However, the incidence of these skin rashes has not been reported. Additionally, edema due to B19V infection varies from mild to generalized [13,14]. Furthermore, B19V infection causes renal disorders, such as acute glomerulonephritis and nephrotic syndrome, which frequently resolve spontaneously [5,11]. However, B19V blood tests can show false-positive results for auto-antibodies, such as antinuclear antibodies, ANCA antibodies, and rheumatoid factor [6,7]. These diverse clinical and laboratory outcomes are believed to be due to direct damage from the viral infection and immune complexes created because of induced auto-antibody production; however, the exact causative mechanism remains unknown [5,12] and could be similar to that of an autoimmune disease.
Generally, IgM in response to B19 appears 7 to 10 days after infection and remains positive for 2 to 4 months. B19V-IgM antibody detected via enzyme immunoassay can be used to diagnose acute or recent infection and is the mainstay of diagnosis in healthy hosts [1].
However, when clinical and general examination outcomes suggest SVV during provisional diagnosis, appropriate diagnostic tests should be performed expeditiously while considering the differential diagnoses. In the present case, we considered MPA to be a disease that could not be overlooked owing to its potential to cause rapid deterioration of renal function.
MPA has been hypothesized to be an autoimmune abnormality-induced SVV involving ANCA, although its definitive cause remains unknown [8–10,15]. It is reported to have an incidence rate and a prevalence of 0.5 to 24.0 and 9 to 94 per million, respectively, occurring predominantly in middle-aged and older adults, without sex differences [16]. In addition to systemic symptoms, such as fever, fatigue, and weight loss, MPA is associated with arthralgia, skin rashes (palpable purpura and livedo reticularis), and peripheral neuropathy [8]. Renal involvement is the most common manifestation of severe MPA, and an early diagnosis is crucial due to the possibility of rapid progression and transition to end-stage renal failure [9]. Furthermore, neuropathy is present in 50% of patients with MPA [17]. We assumed SVV, particularly MPA, and performed the tests necessary to evaluate the MPA categorization criteria to enable a rapid diagnosis [10]. However, the results did not indicate MPA and were as follows: Computed tomography showed no lung abnormalities, skin biopsy showed no abnormal findings, and the ANCA result was negative.
In this case, there was no history of contact with children; however, B19V infection was prevalent in the community at that time [18].
Moreover, spontaneous improvement in skin rash, livedo reticularis, and bilateral edema of the limbs was observed. Although joint pain is common in adults with B19V infection, it was not present in this case. The clinical manifestations of B19V in adults vary widely, making diagnosis based on the physical examination outcomes alone an arduous task. Peripheral neuropathy is an uncommon symptom of B19V infection; however, in this case, the patient had numbness localized to the plantar region that was exacerbated by ankle joint movement and resolved with the improvement of the lower leg edema. Therefore, his symptoms were probably due to tarsal tunnel syndrome. The clinical manifestations and course of the disease, combined with the positive B19V-IgM antibody test results, led to a definitive diagnosis of B19V infection.
Conclusions
B19V infection in adults can mimic vasculitis. In the present case, the initial clinical presentation and laboratory results strongly suggested SVV; therefore, the patient was examined, while we considered MPA, particularly because of the potential for rapid progression of renal dysfunction. Vasculitis requires rapid diagnosis; however, mimics should be ruled out. Therefore, even in older patients, it is critical to consider the possibility of B19V infection, particularly during epidemic periods of the viral infection, and conduct interviews and tests for differentiation.
References:
1.. Landry ML, Parvovirus B19: Microbiol Spectr, 2016; 4 DMIH2-0008-2015
2.. Servey JT, Reamy BV, Hodge J, Clinical presentations of parvovirus B19 infection: Am Fam Physician, 2007; 75; 373-76
3.. Mage V, Lipsker D, Barbarot S, Different patterns of skin manifestations associated with parvovirus B19 primary infection in adults: J Am Acad Dermatol, 2014; 71; 62-69
4.. Sajjan VV, Lunge S, Swamy MB, Pandit AM, Livedo reticularis: A review of the literature: Indian Dermatol Online J, 2015; 6; 315-21
5.. Waldman M, Kopp JB, Parvovirus B19 and the kidney: Clin J Am Soc Nephrol, 2007; 2; S47-56
6.. Vassilopoulos D, Calabrese LH, Virally associated arthritis 2008: Clinical, epidemiologic, and pathophysiologic considerations: Arthritis Res Ther, 2008; 10; 215
7.. Maningding E, Kermani TA, Mimics of vasculitis: Rheumatology (Oxford), 2021; 60; 34-47
8.. Kallenberg CG, The diagnosis and classification of microscopic polyangiitis.: J Autoimmun, 2014; 48–49; 90-93
9.. Wallace ZS, Miloslavsky EM, Management of ANCA associated vasculitis.: Br Med J., 2020; 368 m421
10.. Suppiah R, Robson JC, Grayson PC, 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis.: Arthritis Rheumatol, 2022; 74; 400-6
11.. Young NS, Brown KE, Parvovirus B19: N Engl J Med, 2004; 350; 586-97
12.. Broliden K, Tolfvenstam T, Norbeck O, Clinical aspects of parvovirus B19 infection: J Intern Med, 2006; 260; 285-304
13.. Wiggli B, Imhof E, Meier CA, Laifer G, Water, water, everywhere. Acute parvovirus B19 infection.: Lancet, 2013; 381; 776
14.. Katta R, Parvovirus B19: A review: Dermatol Clin, 2002; 20; 333-42
15.. Jennette JC, Falk RJ, Bacon PA, 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides: Arthritis Rheum, 2013; 65; 1-11
16.. Kitching AR, Anders HJ, Basu N, ANCA-associated vasculitis: Nat Rev Dis Primers, 2020; 6; 71
17.. Collins MP, Periquet MI, Isolated vasculitis of the peripheral nervous system: Clin Exp Rheumatol, 2008; 26(Suppl. 49); S118-30
18.. Infectious Disease Outbreak Surveillance Weekly Report. Miyagi Prefectural Government Homepage (Japanese). URL: , accessed on May 29, 2023https://www.pref.miyagi.jp/site/hokans/surveypdf-shuho.html
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133