28 July 2023: Articles 
Enhancing Body Balance and Performance in Elite Archery Athletes: The Impact of Atlasprofilax Intervention on Suboccipital Myofascia
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment
Lluis ManentDOI: 10.12659/AJCR.939824
Am J Case Rep 2023; 24:e939824






Abstract
BACKGROUND: High-performance athletes, such as archers, require optimal proprioception and balance. Subclinical or underestimated metabolic and pathomechanic alterations in the suboccipital myofascia could lead to loss of performance in balance and proprioception. Therapeutic optimization of myofascia and its complex structures through noninvasive stimulation by mechanotransductive vibropressure could be a preliminary key factor in high-performance athletes for high-performance sport.
CASE REPORT: This study was conducted with 6 athletes from the Brazilian Olympic archery team to evaluate the impact of the Atlasprofilax intervention on body balance. The results were measured using a standardized medical stabilometric platform, which assessed static balance and proprioception capacity. One athlete underwent the intervention before the entire team was tested for balance and reflexes in their archery performance. The study found that the intervened athlete showed improved balance and reflexes, as indicated by superior scores in the risk of fall assessment and fall index. The results suggest the potential for the Atlasprofilax intervention to improve body balance and proprioception in high-performance athletes.
CONCLUSIONS: A single intervention using the Atlasprofilax method in 1 of 6 Olympic archers resulted in significant improvement in balance and proprioception when compared with that of the non-intervened athletes. This preliminary evidence suggests that the Atlasprofilax intervention on the suboccipital myofascia may have a positive impact on enhancing balance and performance in elite athletes by improving proprioception.
Keywords: Atlanto-Occipital Joint, Fascia, postural balance, Humans, athletic performance, athletes, Proprioception, Brazil
Background
Balance in humans is complex and is dependent on biomechanics, especially in upright posture during physical activity. The suboccipital hinge, including the suboccipital myofascia, plays a crucial role in balance control owing to its high concentration of mechanoreceptors and proprioceptors, which allow for precise detection of changes in head angular posture. Imbalances in cervical alignment, particularly suboccipital (C0-C2) hyperextension, can lead to neck pain and other postural consequences [1]. Asymptomatic subclinical cervical sagittal imbalance related to C0-C2 underestimated abnormalities could potentially reduce the body’s proprioception and balance, thereby impacting sports performance. Head movements are essential in affecting cerebrospinal fluid pressure, and the myodural bridge and the suboccipital muscles play a key role in this process [2]. Suboccipital muscles are involved in sensorimotor control and stabilization of the spinal cord. Several soft tissue structures that cross over the cervical epidural space connect suboccipital myofascia and dura [3]. Proprioceptive inputs from suboccipital muscles are relevant in head-eye coordination and postural performance, and those muscles have a high spindle content [4].The high density, type of distribution, and morphology of muscle spindles found in the rectus capitis posterior minor indicate their important role of “proprioceptive monitors” of the cervical spine and head, in addition their motor function [5]. Suboccipital muscle atrophy is negatively correlated with proper standing balance, reducing proprioceptive output from atrophied muscles. Loss of control in standing balance can be due to the lack of proprioceptive inhibition of nociceptors at the dorsal horn of the spinal cord [6]. Multiple studies have shown that myodural connections bridge the epidural spaces between 3 of the 4 suboccipital muscles and the dura mater [7–10]. Other studies established correlations between the suboccipital myofascia and cervical dura mater, with implications in postural control, sensorimotor function, and cervicocephalic pain syndromes [3,11,12] and other disorders, such as Arnold-Chiari malformation [13], a problem that is highly correlated with body imbalance. Alterations in cervical proprioception, sympathetic tone, balance, and dural enfolding due to cervical spine trauma have also been studied [14–16]. Fascia and its interconnections play a very important role in body alignment and myofascial tissue integrity. Changes induced in certain areas or parts of the myofascial tissues can affect others remotely [17–20].
The Atlasprofilax method is a device-mediated intervention on the suboccipital myofascia that uses mechanotransductive vibropercussion, aiming an amelioration of clinical or subclinical metabolic and structural alterations, which are often underestimated, of the soft tissues and bony structures of the occipito-cervical hinge [21]. Clinical experience with the Atlasprofilax method supports that this intervention helps in recovering or ameliorating the orthogonal cephalopodalic axis, which brings improvements in spinal curves, center of gravity, and body balance. The Atlasprofilax method has already showed benefits in jaw and temporomandibular joint disorders [22], fibromyalgia [23], and radiologic improvements in the orthogonality of the C0-C1-C2 segment [24,25]. The pathologies in which the Atlasprofilax intervention showed therapeutic gains have a correlation with postural control deficits and imbalance [26–28]. Body balance is an important health-related component of physical activity, as it can influence training and competition results in sports. Any potential physiologically induced enhancement in postural control and balance can translate into improved performance and sporting outcomes. The main characteristic of archery is that the archer adopts the most static posture possible. Its principle is stability and repetition of movements in order to obtain a consistent shot. This is key when the body is stationary (state of static equilibrium). Archery efficiency is measured by scoring arrows on a target. Research aimed at enhancing athletes’ performance also examines factors such as balance, which is the capacity to maintain coordination and control in counteracting forces that can disrupt optimal performance. Athletes increase their stability when they increase the size of their base of support.
The stability of the body is closely tied to the center of gravity’s projection on the base of support. A lower center of gravity leads to a more stable body. Archers require exceptional balance and postural control under static conditions. To maintain balance, the body’s line of gravity within the base of support must be kept steady, with minimal postural oscillation. Multiple systems and inputs coordinate to maintain balance, including the visual, vestibular, and somatosensory systems. The proprioceptive system is essential in providing information about body positioning and movement. For archers, the base of support is a square polygonal surface that encompasses the tips of the feet and heels. Archers begin by holding the bow low in front of them and then raising it with an extended arm. This movement raises the center of gravity and shifts it to the foot closest to the target, leading to a more unstable balance. The neck joint receptors provide critical proprioceptive information to the nervous system, enabling the archer to maintain proper orientation of the head in relation to the body (Figure 1).
Case Reports
CLINICAL INTERVENTION AND BALANCE TESTING:
The intervention was performed only on athlete 5, on November 13, 2014, at the Primeira Vértebra Clinic in Belo Horizonte, Brazil. The balance tests were performed on November 25, of 2014, at Pakaesejong Clinic Sports Rehabilitation Center in South Korea. The intervention was blinded to the balance test examiners and to the other 5 athletes participating in the pilot test. The Atlasprofilax method uses intermittent percussive mechanical vibropressure mediated by a noninvasive device (Figure 2). The intervention was applied once during 8 min on multiple specific points of the suboccipital region to stimulate certain receptors involved in proprioception and muscle reflex. By intervening in the suboccipital region, a domino effect was pursued, aiming at an improvement in the antero-posterior and lateral symmetry of muscle chains as well as in the body’s fascial tensegrity. The intervention targets a profound mechanotransduction effect on the suboccipital muscles and their multiple receptors, especially in their proprioceptors, as well as on other upper neck muscles and the cervical deep fascia. Suboccipital muscles are located within a dense fibro-fatty tissue region, which is beneath the semispinalis capitis. Multiple neck muscles act as skeletal muscles transferring downward biomechanical and elastic energy to all myofascial chains. To maintain horizontal gaze and proper balance, the craniocervical structures can counteract the loss of lordosis by modifying the physiological Cobb angle, affecting proprioception and body balance. It is very likely that subclinical alterations in suboccipital myofascia can negatively affect the myofascial chains in their symmetry, as well as the posture of the body, by altering proprioception and postural balance.
The 6 athletes underwent physical and balance tests at the Sports Rehabilitation Training Center in Wonju, Korea, lasting 2 h, under the same training conditions, with the same equipment, and on the same day. For balance testing, an Advance Mechanical Technology Inc (AMTI) board was used, which has features specifically produced for balance testing, with 6-board sensors, comprising dynamic and computerized platforms (Figure 3). This platform has a standard of excellence known worldwide for its durability and reliability of the measured data. It meets ISO 13485 standards, with medical qualification, and it has been widely used for measuring balance and proprioception in other conditions [29,30].
METHODS, MEASUREMENTS, AND ENDPOINTS:
Primary and secondary endpoints were measured according to the output scores using an AMTI balance testing board that includes 6-board sensors and dynamic and computerized platforms (Figure 3). The primary endpoint was the risk of fall assessment (Figure 4). The secondary endpoint was the score of the fall index (Figure 5, Table 2). For measuring the primary endpoint, risk of fall assessment, the AMTI software gives a score based on an abscissa and ordinate axis. The closer the score is to the origin point of the axis, the higher the proprioceptive and balance ability and the lower the risk of fall (Figure 4). To measure the secondary endpoint, several factors were measured, such as the stability index and the weight distribution index (WDI), in relation to various values depending on the position of the head, eyes closed open, among others, giving a final value of fall index. The lower the value of the fall index, the higher the stability and proprioceptive performance of the evaluated participant (Figure 5).
Results
The results of the primary endpoint, risk of fall assessment, are shown in Figure 4. Athlete number 5, the only one who underwent the Atlasprofilax procedure, 12 days before the balance testing, obtained the best score among the 6 athletes, reaching the most proximal position to the origin of the abscissa and ordinate axis (Figure 4). For the secondary endpoint, fall index, athlete 5 obtained the best performance, compared with the other athletes, managing to maintain the minimum value in all the evaluated positions, obtaining the lowest total score, and achieving the best placement among all the evaluated athletes in all tests and values (Figures 5, 6, Table 2). No adverse effects related to the intervention were observed.
Table 2 shows that athlete 5, who received the Atlasprofilax intervention, obtained a fall index score of zero, while the other athletes, who did not undergo the intervention, obtained values between 8 and 12.
Discussion
The relevance and relationship of the atlantooccipital hinge and its soft structures to proprioception is well studied [2,31,32]. The proprioceptive role of the posterior rectus muscles of the head is important in posture and balance [33]. Dural infolding through tension in the myodural bridge impacts negatively in proprioception and balance [34]. Although possible subclinical abnormalities in the metabolism of the suboccipital myofascia are not usually examined, they could underlie a decrease in body balance and human proprioceptive ability. Atlasprofilax is a noninvasive device-mediated intervention that uses mechanotransductive vibropercussion, aiming an improvement of underestimated alterations in the suboccipital myofascial [21]. The mechanotransductive mechanism of the Atlasprofilax device could potentially ameliorate not only subclinical metabolic alterations of the suboccipital miofascia but also of the myodural bridge function and its performance. This would biomechanically contribute to improving posture and balance downwardly through the myofascial chains continuum. It is relevant to note that athlete 5, the only one intervened among the 6 members of the Brazilian Olympic archery team, obtained far better scores and performance in proprioceptive and balance skills than the others. Even if we cannot establish a direct correlation between results and intervention, it is possible to suggest a tendency that should be evaluated with a 2-arm study, with pre- and post-intervention measurements and a control group.
A limitation of this study was the small sample size. With a larger number of participants, the statistical significance could determine what this case series can only suggest. A larger study with pre- and post-intervention testing in a larger group of participants and a control group is recommended.
Conclusions
This case series report suggests that the Atlasprofilax intervention could produce positive effects on proprioception, balance, and sport performance in archers. Further studies with a larger sample size could eventually corroborate the trend shown in this case series.
Figures
References:
1.. Patwardhan AG, Havey RM, Khayatzadeh S, Postural consequences of cervical sagittal imbalance: A novel laboratory model: Spine (Phila Pa 1976), 2015; 40(11); 783-92
2.. Ma Y, Tang W, Gong D-Z, The morphology, biomechanics, and physiological function of the suboccipital myodural connections: Sci Rep, 2021; 11(1); 8064
3.. Enix DE, Scali F, Pontell ME, The cervical myodural bridge, a review of literature and clinical implications: J Can Chiropr Assoc, 2014; 58(2); 184-92
4.. Kulkarni V, Chandy MJ, Babu KS, Quantitative study of muscle spindles in suboccipital muscles of human foetuses: Neurol India, 2001; 49(4); 355-59
5.. McPartland JM, Brodeur RR, Rectus capitis posterior minor: A small but important suboccipital muscle: J Bodyw Mov, 1999; 3(1); 30-35
6.. McPartland JM, Brodeur RR, Hallgren RC, Chronic neck pain, standing balance, and suboccipital muscle atrophy – a pilot study: J Manipulative Physiol Ther, 1997; 20(1); 24-29
7.. Hack GD, Koritzer RT, Robinson WL, Anatomic relation between the rectus capitis posterior minor muscle and the dura mater: Spine (Phila Pa 1976), 1995; 20(23); 2484-86
8.. Scali F, Marsili ES, Pontell ME, Anatomical connection between the rectus capitis posterior major and the dura mater: Spine (Phila Pa 1976), 2011; 36(25); E1612-14
9.. Scali F, Pontell ME, Enix DE, Marshall E, Histological analysis of the rectus capitis posterior major’s myodural bridge: Spine J, 2013; 13(5); 558-63
10.. Zumpano MP, Hartwell S, Jagos CS, Soft tissue connection between rectus capitus posterior minor and the posterior atlanto-occipital membrane: A cadaveric study: Clin Anat, 2006; 19(6); 522-27
11.. Bogduk N, Cervicogenic headache: Anatomic basis and pathophysiologic mechanisms: Curr Pain Headache Rep, 2001; 5(4); 382-86
12.. Haldeman S, Dagenais S, Cervicogenic headaches: A critical review: Spine J, 2001; 1(1); 31-46
13.. Labuda R, Nwotchouang BST, Ibrahimy A, A new hypothesis for the pathophysiology of symptomatic adult Chiari malformation type I.: Med Hypotheses., 2022; 158; 110740
14.. Palmgren PJ, Andreasson D, Eriksson M, Hägglund A, Cervicocephalic kinesthetic sensibility and postural balance in patients with nontraumatic chronic neck pain – a pilot study.: Chiropr Osteopat, 2009; 17; 6
15.. Rix GD, Bagust J, Cervicocephalic kinesthetic sensibility in patients with chronic, nontraumatic cervical spine pain: Arch Phys Med Rehabil, 2001; 82(7); 911-19
16.. Uhlig Y, Weber BR, Grob D, Müntener M, Fiber composition and fiber transformations in neck muscles of patients with dysfunction of the cervical spine: J Orthop Res, 1995; 13(2); 240-49
17.. Burk C, Perry J, Lis S, Can myofascial interventions have a remote effect on ROM? A systematic review and meta-analysis: J Sport Rehabil, 2020; 29(5); 650-56
18.. Wilke J, Niederer D, Vogt L, Banzer W, Remote effects of lower limb stretching: Preliminary evidence for myofascial connectivity?: J Sports Sci, 2016; 34(22); 2145-48
19.. Tamartash H, Bahrpeyma F, Dizaji MM, Effect of remote myofascial release on lumbar elasticity and pain in patients with chronic nonspecific low back pain: A randomized clinical trial: J Chiropr Med, 2023; 22(1); 52-59
20.. Kang HS, Kwon HW, Kim DG, Effects of the suboccipital muscle inhibition technique on the range of motion of the ankle joint and balance according to its application duration: A randomized controlled trial: Healthcare (Basel), 2021; 9(6); 646
21.. Angulo O, The mystery around suboccipital myofascial alterations and their correlated ailments. Could the Atlasprofilax method be a therapeutic option?: EC Orthopaedics, 2023; 14(3); 1-5
22.. Navas V, [Effect of Atlasprofilax® therapy on symptoms related to temporomandibular dysfunction, bruxism and the relationship of dental midlines.]: UstaSalud, 2013; 12; 124
23.. Malagón J, Villaveces M, Manent L, A Therapeutic alternative in the management of fibromyalgia: Revista Cuarzo, 2017; 23; 30
24.. León JG, Laguna N, Manent L, Radiological improvements in symmetry of the lateral atlantodental interval and in atlas tilt after the application of the Atlasprofilax method: A case series. CPQ Orthopaedics, 2022; 6(3); 1-13
25.. León JG, Manent L, Lewis K, Angulo O, Clinical and imaging improvement after the Atlasprofilax method in a patient with cervicobrachial syndrome and temporomandibular joint disorders. A case report.: Acta Sci Orthop, 2021; 4(10); 92-102
26.. Bracco P, Deregibus A, Piscetta R, Effects of different jaw relations on postural stability in human subjects: Neurosci Lett, 2004; 356(3); 228-30
27.. Jones KD, King LA, Mist SD, Postural control deficits in people with fibromyalgia: A pilot study.: Arthritis Res Ther., 2011; 13(4); R127
28.. Larsen K, Atlas joint instability: Causes, consequences and solutions. [Online] Published Sept. 10, 2017. . Available from: MSKNeurology.com
29.. Labanca L, Ciardulli F, Bonsanto F, Balance and proprioception impairment, assessment tools, and rehabilitation training in patients with total hip arthroplasty: A systematic review.: BMC Musculoskelet Disord, 2021; 22(1); 1055
30.. Chung PH, Lin GL, Liu C, The effects of tai chi chuan combined with vibration training on balance control and lower extremity muscle power: J Sports Sci Med, 2013; 12(1); 19-26
31.. Scali F, Ohno A, Enix D, Hassan S, The posterior atlantooccipital membrane: The anchor for the myodural bridge and meningovertebral structures: Cureus, 2022; 14(5); e25484
32.. Song X, Gong J, Yu SB, The relationship between compensatory hyperplasia of the myodural bridge complex and reduced compliance of the various structures within the cranio-cervical junction: Anat Rec (Hoboken), 2023; 306(2); 401-8
33.. Hallgren RC, Rowan JJ, Implied evidence of the functional role of the rectus capitis posterior muscles: J Am Osteopath Assoc, 2020; 120(6); 395-403
34.. Pontell ME, Scali F, Marshall E, Enix D, The obliquus capitis inferior myodural bridge: Clin Anat, 2013; 26(4); 450-54
Figures
Tables
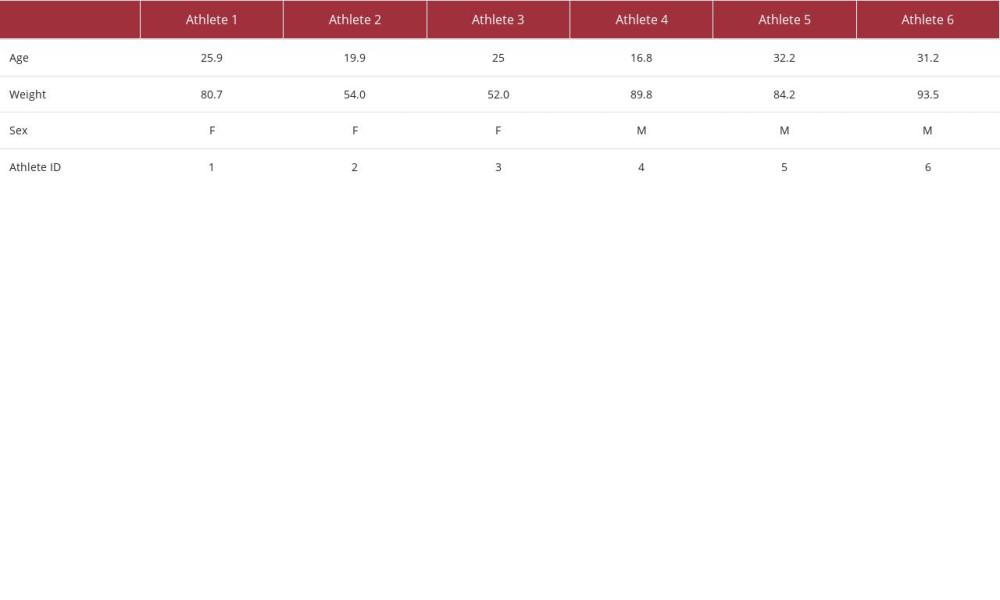 Table 1.. Characteristics of the 6 Brazilian athletes.
Table 1.. Characteristics of the 6 Brazilian athletes.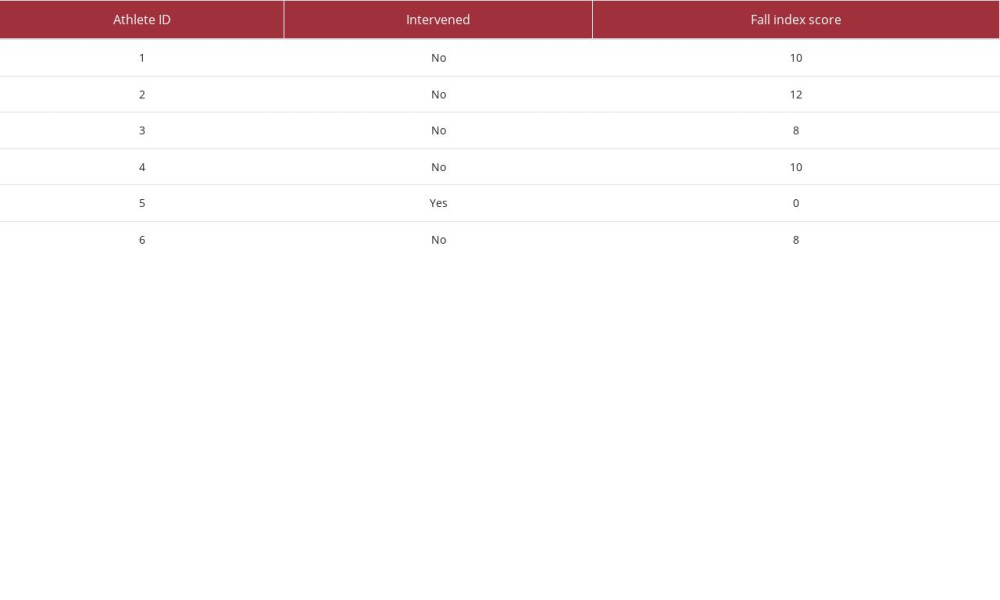 Table 2.. Fall index results. Final score obtained for the 6 athletes (see also Figure 4). The lower the score, the lower the fall index and the better the balance and proprioception ability.Table 1.. Characteristics of the 6 Brazilian athletes.Table 2.. Fall index results. Final score obtained for the 6 athletes (see also Figure 4). The lower the score, the lower the fall index and the better the balance and proprioception ability.
Table 2.. Fall index results. Final score obtained for the 6 athletes (see also Figure 4). The lower the score, the lower the fall index and the better the balance and proprioception ability.Table 1.. Characteristics of the 6 Brazilian athletes.Table 2.. Fall index results. Final score obtained for the 6 athletes (see also Figure 4). The lower the score, the lower the fall index and the better the balance and proprioception ability. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133