22 December 2023: Articles 
Successful Pediatric Penile Replantation Following Amputation During Ritual Circumcision: A Case Report and Literature Review
Management of emergency care
Niti Tawaranurak1ABCDEF*, Worapat Attawettayanon2ABE, Sarayuth Boonchai2ABCDE, Virote Chalieopanyarwong3A, Wanchalerm Chungsiriwattana1AE, Laliphat Kongpanichakul1AEDOI: 10.12659/AJCR.942448
Am J Case Rep 2023; 24:e942448






Abstract
BACKGROUND: Circumcision is commonly performed in males, especially in Jewish and Muslim cultures, and is considered a safe surgical procedure with a low complication rate. Major complications, such as partial and total penile amputation, can occur, but those are rare complications. However, high replantation success rates have been reported and reviewed.
CASE REPORT: We describe the case of an 8-year-old boy who experienced total penile amputation during ritual circumcision performed by a layperson outside the hospital setting. Microsurgical penile replantation was performed after an ischemic period of 16 hours 43 minutes, with successful outcomes and without any major complications. In our technique, we repaired both dorsal and deep cavernosal vessels. At 1-year postoperative period, the results of two-point discrimination test were 4 mm, 7 mm, and 7 mm on the dorsal part, ventral part, and glans, respectively. After a follow-up period of 4 years, there were no late complications such as penile deformity, urethral fistula, urethral stenosis, absence of penile sensation, or erectile dysfunction. The results of two-point discrimination test were 3 mm, 5 mm, and 5 mm on the dorsal part, ventral part, and glans, respectively. The patient also experienced good penile sensation, morning erection, satisfaction with the cosmetic outcome, and a peak urine flow rate of 21 mL/s with a consistently strong void stream and a low postvoid residual urine volume of 20 mL.
CONCLUSIONS: Our experience suggests that a short ischemic time, prompt surgical correction, microscopic technique of replantation, and intensive postoperative care can result in good functional outcomes.
Keywords: Circumcision, Male, Replantation, Amputation, Penis, Pediatrics, Reconstructive Surgical Procedures, Humans, Male, Child, Ceremonial Behavior, Amputation, Traumatic, Ischemia
Background
Ritual circumcision without therapeutic indications is a common surgical procedure, particularly in Jewish and Muslim populations. Circumcision is performed by healthcare providers or laypeople, which may account for the variability of the reported complication rates, from 0.2% to 15% [1,2]. Traumatic penile amputation is a rare but serious complication of this procedure.
Penile replantation in children is typically performed as soon as possible after the injury, and has a high success rate owing to the greater flexibility and elasticity of the blood vessels and skin in these patients [3]. Most patients experience a return of function and satisfactory cosmetic appearance following the procedure. However, potential complications associated with penile replantation include infection, tissue necrosis, and loss of function. It is therefore important that patients and their families work closely with a team of healthcare professionals, including urologists and plastic surgeons, to ensure the best possible outcome.
The surgical technique of pediatric penile replantation involves several steps. First, the surgeon carefully cleans the amputated penis and any remaining tissues to remove dirt and debris. Next, the surgeon carefully reattaches the penis using micro-surgical techniques. This must involve the reattachment of blood vessels, nerves, and other structures to restore blood flow and nerve function to the penis.
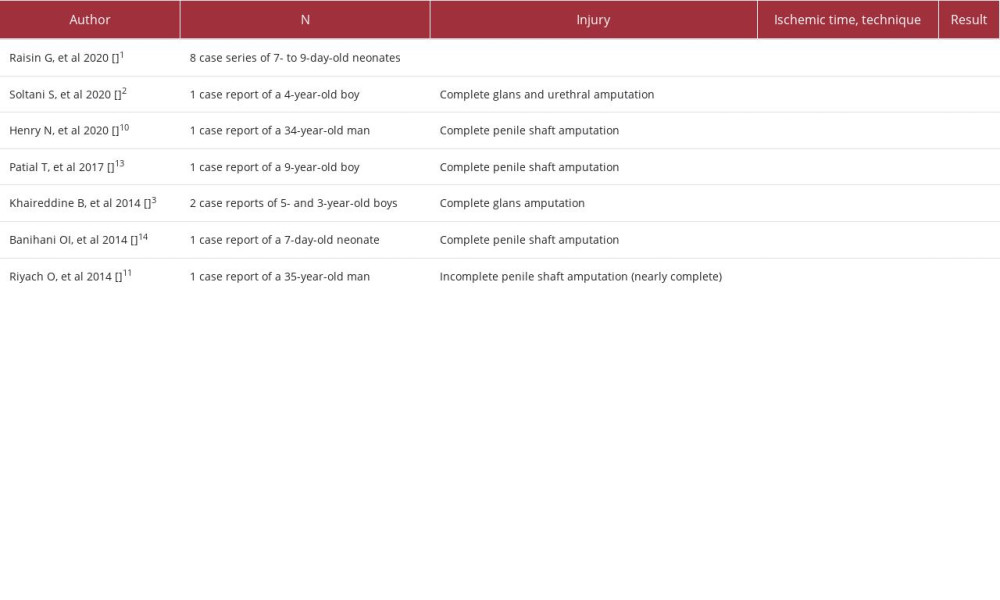
In this article, we report the case of an 8-year-old boy who underwent total penile amputation as a result of a ritual circumcision performed by an imam. We describe our experience related to the management and long-term follow-up of this patient, along with a literature review (Table 1).
Case Report
An 8-year-old boy was referred from a rural hospital after total penile amputation incurred during ritual circumcision by an imam (a Muslim religious leader). The degree of injury was equivalent to that of a total penectomy (Figure 1). The amputated tissue was soaked in cool moist gauze and placed in a plastic bag, which was then closed. This bag was placed inside a second plastic bag containing ice, which was also closed. A wet dressing was applied to the penile stump. Pressure dressing with elastic bandage was applied on the waist. The patient underwent emergency penile replantation under general anesthesia.
The patient was placed in a supine position with the legs spread apart and a suprapubic cystostomy was placed. The blood vessels, nerves, and urethra were carefully identified and repaired using microsurgical techniques. The corpus spongiosum and urethra were identified using a small 8-Fr urethral catheter and the railroading technique. The urethra and corpus spongiosum were repaired using 6-0 Vicryl® suture material. Bilateral cavernous arteries, which carry blood into the corpus cavernosum, were repaired using 11-0 Ethilon® suture. The autonomic nerve supply was re-approximated at maximum microscopic magnification. Then, the tunica albuginea was closed using a 6-0 round polydioxanone running suture. The deep dorsal arteries, veins, and 2 dorsal nerves were repaired using 10-0 and 9-0 Ethilon® sutures, respectively. Then, Buck’s fascia was closed using a 6-0 round polydioxanone with interrupted suture to prevent the tightening of deep dorsal vessels, and the superficial dorsal veins were repaired with an 11-0 Ethilon® suture. The skin was closed with interrupted 6-0 Vicryl Rapide® sutures. The penis was covered with an antibiotic-loaded petroleum tulle dressing and a loose gauze bandage and maintained in an upright position with an 8-Fr Foley catheter inserted for 3 weeks following the surgery. Intravenous antibiotic was given for 14 days and the patient did not receive any heparinization.
The total ischemic time was 16 hours 43 minutes. Restorative blood supply to the glans was achieved (Figure 2). The patient was placed on bed rest for the first 48 hours postoperatively. Analgesia was administered as required and the patient was monitored closely for signs of vascular ischemia or congestion. The patient was discharged without any major complications and was scheduled for biannual clinical follow-up appointments with uroflowmetry. At the 1-year postoperative follow-up, the results of the two-point discrimination test were 4 mm, 7 mm, and 7 mm on the dorsal part, ventral part, and glans, respectively. During 4 years of follow-up, the patient experienced good cosmetic outcomes, better penile sensation, and functional outcomes (Figure 3). The results of the two-point discrimination test were 3 mm, 5 mm, and 5 mm on the dorsal part, ventral part, and glans, respectively. His peak urine flow rate improved continuously, reaching 21 mL/s (Figure 4), with a consistently strong void stream and a low postvoid residual urine volume of 20 mL. Furthermore, the patient reported morning erections and satisfaction with the cosmetic outcome of the surgery.
Discussion
Penile amputation during circumcision is rare and challenging. Currently, there is no standard classification system for external genital injuries. Most penile injuries in pediatric patients are caused by circumcision, animal bites, or zippers [4]. Initial management of penile amputation involves resuscitation and proper specimen collection. Moreover, replantation requires good cooperation between urologists and plastic surgeons.
Pediatric penile replantation involves the reattachment of a penis following partial or complete amputation, typically due to an accident or injury. The goal of the procedure is to restore the normal function and appearance of the penis. Surgical success often depends on the availability and quality of the amputated tissue, as well as the skill and experience of the surgeon.
In general, arterial anastomosis primarily involves the dorsal arteries beneath Buck’s fascia. Previous studies have demonstrated that a single set of approximated arteries was adequate to maintain adequate collateral blood flow between the deep and superficial systems [5,6]. In our experience, dorsal arterial anastomosis alone can lead to distal prepuce necrosis. In the present patient, we intended to repair the deep cavernous arteries because we believed that they would supercharge arterial blood supply and even help in erectile function.
If microsurgery cannot be performed at the presenting hospital and the transfer time to a hospital offering this procedure is more than 24 hours, macrosurgery can be performed. Macroscopic penile replantation was first reported by Ehrich in 1929, and his technique depended on corporal sinusoidal blood flow with the distal amputated part, as a composite graft [7]. Macroscopic replantation can be successful in some cases, and its advantages may include shorter operative times and the use of less specialized equipment. However, the disadvantages are significant, and can lead to higher rates of complications such as skin necrosis, urethral stricture, or pe-nile loss. In contrast, in 1977 Cohen reported the microsurgical technique of replantation, which provided early restoration of blood flow with better graft survival [8]. Microscopic techniques are more time-consuming and require specialized microsurgical skills. They have been associated with reduced complications and improved functional results due to meticulous anastomosis of small nerves and blood vessels. The microsurgical penile replantation has been shown to improve the cosmetic appearance, urination, sensation, and erectile function [1–3,8–10].
Ischemic time is a strong prognostic factor of operative outcome [11]. Shukla et al reported that replantation can be attempted up to 24 hours after injury [12], with cutoff points for warm and cold ischemic times of 4 and 16 hours, respectively. Cooling the amputated tissue in ice is a valuable method that can extend the ischemic time. When the replantation procedure was started beyond 24 hours postamputation, the success rate was very low. In our patient, the ischemic time was 16 hours 43 minutes, allowing a good functional outcome to be achieved.
After surgery, the child is typically closely monitored in the hospital for several days to ensure proper healing of the reattached penis. Physical therapy may be recommended to help improve blood flow and function, and children may also be prescribed medication to alleviate pain and inflammation. In some cases, additional surgery may be necessary to address complications or improve the appearance or function of the penis. Cautious postoperative care can help prevent delayed complications, such as infection, vessel thrombosis, penile curvature, and urethral stricture. Erectile dysfunction can be prevented by vigorous autonomic nerve re-approximation in the corpus cavernosum. Furthermore, patients undergoing this type of surgery require broad-spectrum antibiotic therapy [12]. Thrombosis of the microvascular anastomosis is also an important issue. The interrupted suture technique was used to avoid the compression of deep dorsal vessels, to prevent necrosis on the skin of the penis. Recent reports have recommended the use of low-molecular-weight heparin and the opioid alkaloid papaverine to prevent thrombosis and vasospasms [12,13]. In addition, the use of postoperative leech therapy has been reported for the treatment of venous congestion [14].
Common late complications of penile replantation include pe-nile deformity, urethral fistula, urethral stenosis, the absence of penile sensation, and erectile dysfunction [13], although improved microsurgical techniques have decreased the incidence of these complications. The postoperative peak urine flow rate in our patient increased with age and was comparable to that of the general pediatric population [15,16]. Uroflowmetry may be a valuable noninvasive method of assessing void stream characteristics, which helps confirm the patency of urethral anastomosis and long-term outcomes.
Conclusions
Circumcision-related complications vary from minor to serious. Penile amputation is a serious condition requiring prompt microsurgery. Penile replantation in children is a complex and delicate surgical procedure that requires a high level of skill and experience. With proper care and follow-up, the procedure can be highly successful in restoring normal penile function and appearance. Our experience suggests that a short ischemic time, prompt surgical correction, microscopic technique of replantation, and intensive postoperative care can result in good functional outcomes.
Figures
References:
1.. Raisin G, Kocherov S, Jaber J, Glans injury during ritual circumcision: J Pediatr Urol, 2020; 16; 471.e1-e5
2.. Soltani S, Mottaghi M, Jafarpisheh A, Tavakkoli M, Penile glans amputation following circumcision: A case report of a rare complication: Case Rep Urol, 2020; 2020; 5806987
3.. Khaireddine B, Adnen H, Khaled BM, Adel S, Surgical reimplantation of penile glans amputation in children during circumcision: Urol Ann, 2014; 6; 85-87
4.. Kim JH, Park JY, Song YS, Traumatic penile injury: From circumcision injury to penile amputation: Biomed Res Int, 2014; 2014; 375285
5.. Jezior JR, Brady JD, Schlossberg SM, Management of penile amputation injuries: World J Surg, 2001; 25; 1602-9
6.. Reiss HF, Newman HF, Zorgniotti A, Artificial erection by perfusion of pe-nile arteries: Urology, 1982; 20; 284-88
7.. Ehrich WS, Two unusual penile injuries: J Urol, 1929; 21; 239-41
8.. Cohen BE, May JW, Daly JS, Young HH, Successful clinical replantation of an amputated penis by microneurovascular repair. Case report: Plast Reconstr Surg, 1977; 59; 276-80
9.. Babaei AR, Safarinejad MR, Penile replantation, science or myth? A systematic review: Urol J, 2007; 4; 62-65
10.. Henry N, Bergman H, Foong D, Filobbos G, Successful penile replantation after complete amputation and 23 hours ischaemia time: The first in reported literature: BMJ Case Rep, 2020; 13; e234964
11.. Riyach O, El Majdoub A, Tazi MF, Successful replantation of an amputated penis: A case report and review of the literature: J Med Case Rep, 2014; 8; 125
12.. Shukla CJ, Brown G, Dorkin T, British Association of Urological Surgeons (BAUS) consensus document for the management of male genital emergencies – penile amputation: BJU Int, 2018; 121; 699-702
13.. Patial T, Sharma G, Raina P, Traumatic penile amputation: A case report: BMC Urol, 2017; 17; 93
14.. Banihani OI, Fox JA, Gander BH, Complete penile amputation during ritual neonatal circumcision and successful replantation using postoperative leech therapy: Urology, 2014; 84; 472-74
15.. Kumar V, Dhabalia JV, Nelivigi GG, Age, gender, and voided volume dependency of peak urinary flow rate and uroflowmetry nomogram in the Indian population: Indian J Urol, 2009; 25; 461-66
16.. Singla D, Malik P, Sangwan M, Age, gender, and voided volume dependency of peak urinary flow rate and uroflowmetry nomogram in a tertiary care centre: Asian Pac J Health Sci, 2018; 5; 13-16
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133