06 May 2024: Articles 
Medial Hoffa Fracture: A Case Report and Literature Review of Approach and Management
Challenging differential diagnosis, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Alaa Akel1ABCDEFG, Mohammed Yahia Sarhan2ABCDEFG, Mohammad Abu-JeyyabDOI: 10.12659/AJCR.943136
Am J Case Rep 2024; 25:e943136






Abstract
BACKGROUND: Hoffa fractures are an uncommon form of coronal fracture that impact the femoral condyle. As a result, they are not very prevalent. It is necessary to perform anatomical reduction and rigorous fixation on these fractures; however, there is no consensus among medical professionals on the surgical procedure and implant that would be the most successful in treating these fractures.
CASE REPORT: A 50-year-old woman who had poliomyelitis in her right lower limb presented with a displaced medial Hoffa fracture of her left knee. She had fallen and was suffering from poliomyelitis. The trauma that caused this fracture had a modest energy level. Open reduction and internal fixation with 2 retrograde cannulated screws were included in her surgical procedure. An approach known as the medial parapatellar route was used for this treatment. As part of her postoperative rehabilitation, she participated in physiotherapy, exercises that did not require weight bearing, exercises that used passive and active assistance, activities that involved partial and full weight bearing, and exercises that involved complete weight bearing. At the 2-year follow-up, the patient’s left knee continued to be painless and stable, and it had unrestricted range of motion across the whole extremity. It was determined via radiographs that the fracture had healed without any problems or arthritic changes developing. She was able to walk without help and carry out her daily tasks since she was able to walk with the use of a cane.
CONCLUSIONS: Retrograde cannulated screws can be a reliable and successful choice for treatment of medial Hoffa fractures, with positive results according to both clinical and radiographic characteristics. Further research is needed to analyze the outcomes over a longer period of time and make comparisons between this technique and others.
Keywords: Accidental Falls, Classification, Femoral Fractures, fracture dislocation, Female, Humans, Middle Aged, Bone Screws, Fracture Fixation, Internal, Hoffa Fracture, Open Fracture Reduction, Poliomyelitis
Introduction
Hoffa fractures are an uncommon kind of distal femoral fracture that affects the joint surface of the knee and occurs in the coronal plane of the femoral condyle. They account for around 40% of intercondylar fractures and are most commonly encountered in adults following high-energy trauma [1]. The lateral femoral condyle is involved in most Hoffa fractures, but medial Hoffa fractures can also occur [2,3]. Because there is no consensus on the best therapy for these fractures, the purpose of this case study is to evaluate the literature on medial Hoffa fracture patients, as well as surgical procedures and fixation methods for their care. Although anatomical reduction and rigid fixation are typically suggested, the choice of implants and procedures may vary according on the fracture pattern and the comorbidities affecting bone condition, as in the discussed case [3].
Case Report
Following a left-sided accident with a low-energy direct trauma, a 50-year-old female patient presented to the Emergency Department with acute pain and edema in her left knee. Since her infancy, she had been diagnosed with poliomyelitis of the right lower limb, which caused muscle paralysis, limb atrophy, and gait disruption. She was also obese, as measured by a body mass index (BMI) of 32 kg/m2. She presented with severe tenderness and edema of the left knee upon physical examination. Her right side was rendered immobile by poliomyelitis, and she was incapable of locomotion or weight bearing on her left side. Her range of motion at the left knee joint was restricted (15 degrees of extension and 30 degrees of flexion). In that area, there were no open lesions, neurovascular deficits, or indications of infection.
Anterior-posterior (AP) and lateral plain radiographs of the left knee identified a displaced Hoffa fracture (coronal unicondylar medial femoral fracture) (Figure 1A, 1B). No indications of peripheral nerve damage, vascular injury, or additional fractures were present. In addition to confirming the diagnosis, a computed tomography (CT) scan of the left knee was performed to assess the fracture pattern, displacement, and comminution. A displaced Hoffa fracture was detected by a CT scan; no other injuries were observed (Figure 2A, 2B).
According to the Knee Injury and Osteoarthritis Outcome Score (KOOS-PS) [4] and upon patient survey on daily life activity, the patient score was 75.1% preoperatively. It was also Pires category 2 and Orthobullets 33b3.
On the day of admission, she underwent surgical intervention while under general anesthesia. The fracture site was exposed via a limited midline incision made through the medial parapatellar approach. Anatomical reduction was successfully completed, and fixation was executed retrogradely using two 6.5-mm cannulated screws into the posterior femoral condyle articular cartilage (Figure 3, 4) under direct vision. The screw tips were sunk into the cartilage. Utilizing fluoroscopy, reduction and fastener position were validated. Following a multilayered closure of the incision, a sterile dressing was applied. Following the operation, a hinged knee brace was utilized to safeguard the fixation and facilitate prompt mobilization.
After surgery, the patient commenced physical rehabilitation in an effort to regain complete muscle strength and range of motion. A physical rehabilitation program was started after surgery to allow her to regain full range of movement with the hinged knee brace initially locked at 15 degrees of flexion with a non-weight bearing rehabilitation protocol. Range of motion knee exercise started at 2 weeks after the surgery, with the hinged knee brace still on, from 0 extension to 120 degrees of flexion until 6 weeks postoperatively, then discontinuing the hinged knee brace, with active home-based range of motion knee exercises. She had regained full knee range of motion about 8 weeks after surgery, and gradual weight bearing as tolerated started at 4 weeks postoperatively. She regained of full weight bearing with a protective crutch at 8 weeks, and was walking independently and was totally pain free without any concerns at 12–14 weeks. Serial follow-up was performed every 3 months until the last visit 2 years after the operation, when she was pain free without any knee symptoms and still able to achieve a normal full range of movement. In addition, she underwent physiotherapy for the poliomyelitis-affected right lower limb.
Two years after surgery, the patient reported no pain and a normal, full range of motion (0–130 degrees) in her left knee during the final follow-up appointment. She presented with no hardware-related issues or indications of infection. Her follow-up KOOS-PS score was 72.5%. X-ray examination of the fracture revealed no arthritic alterations (Figure 5A, 5B). With the aid of a cane, she was capable of independently walking and carrying out her routine tasks and was satisfied with the results and the rehabilitation program, without any noticeable effect on her daily life activities.
Discussion
A Hoffa fracture is an uncommon form of fracture that occurs within the joint, specifically affecting the back part of the femoral condyles in a horizontal plane. Typically, it is a result of a forceful impact, such as collisions involving motor vehicles or falls from significant heights. The damage occurs either from a direct impact to the bent knee or from an indirect axial load with either inward or outward tension. The diagnosis of Hoffa fracture may go unnoticed or be postponed due to the inconspicuous radiographic signs and the occurrence of other related injuries. Consequently, it is crucial to maintain a heightened level of suspicion and conduct a thorough review of the radiographs. The CT scan is considered the most reliable method for verifying the diagnosis and assessing the fracture pattern, displacement, and comminution [1,3].
Treating a Hoffa fracture can be challenging due to the intricate anatomy involved, as well as the potential risks of mal-union, nonunion, and post-traumatic arthritis. The primary goal of the therapy is to attain anatomical alignment and secure fixation to restore the alignment of the joints and enable prompt mobility. Therapeutic options include conservative management, closed reduction with percutaneous fixation, open reduction with internal fixation (ORIF), and external fixation [5]. The treatment plan is established based on several factors, such as the extent of displacement, comminution, the state of the soft tissues, and the patient’s general health [3,6].
Lateral Hoffa fractures are mainly classified using the Letenneur system, which relies on the position and alignment of the fracture line. However, it is not sufficient for medial Hoffa fractures due to its failure to consider the biomechanical and surgical consequences of these fractures. Consequently, several categorization methods have been suggested for medial Hoffa fractures. The Pires approach categorizes medial Hoffa into types 1 and 2 – type 1 is a horizontal fracture line, and type 2 is an oblique fracture line of the medial condyle – and comminution indicates inclusion of subtypes 1c or 2c, respectively. The Orthobullets system categorizes medial Hoffa fractures as 33B3 fractures, indicating partial articular fractures in the coronal plane. This approach relies on the OTA categorization of distal femur fractures, which takes into account the extent of extra-articular, partial, or total articular involvement of the fracture. Both systems have advantages and disadvantages, necessitating more research to authenticate their dependability and replicability [7].
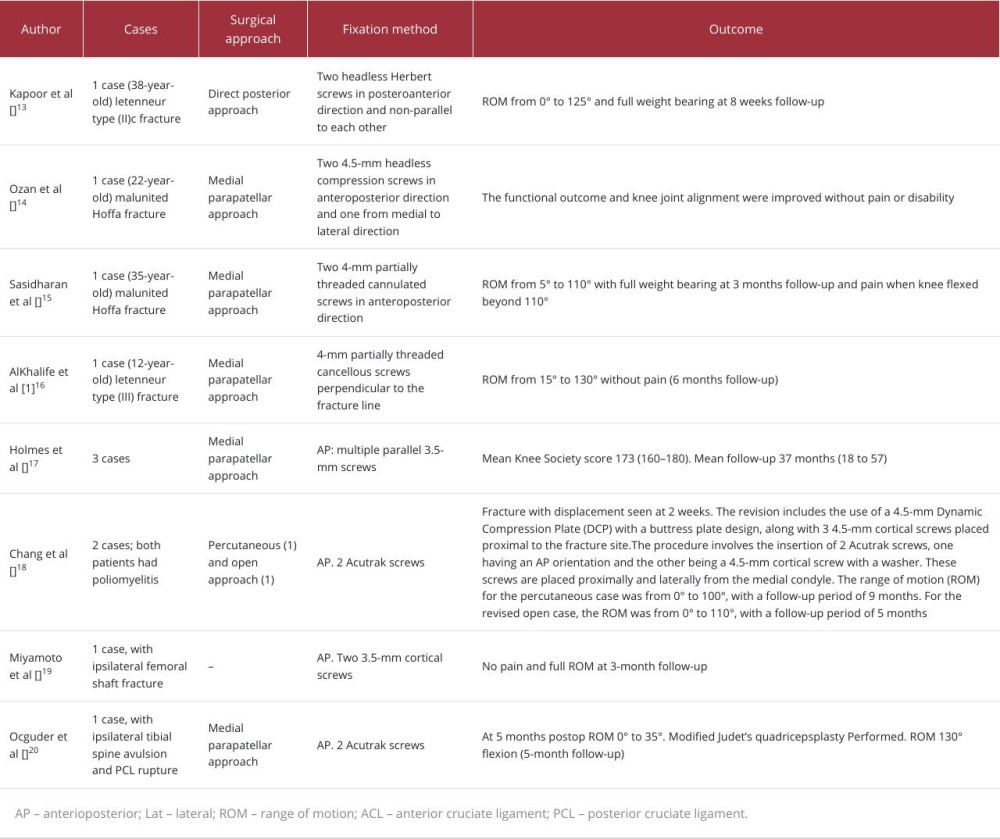
The literature discusses several surgical methods and treatment alternatives for medial Hoffa fractures, which have been evaluated in a study including 100 patients (Table 1).
The choice of surgical technique for a medial Hoffa fracture is determined based on the specific fracture pattern and the surgeon’s personal preference. The medial parapatellar technique is commonly utilized due to its non-interference with prospective future arthroplasty. Nevertheless, it lacks the ability to provide sufficient vision and control over the posterior comminution [2]. To address this constraint, several authors have proposed other methods, such as the extended medial subvastus approach, the modified posteromedial approach, and the direct posterior approach with a sluggish S-shaped incision [3,6]. These methods can help in reducing and stabilizing tiny or rotated fragments, particularly the Letenneur II fragment, which is essential for preserving proper alignment of the joint at a 90° angle of knee flexion. Bagaria et al introduced a novel categorization scheme for medial Hoffa fractures, utilizing CT scan data to determine the most effective treatment approach for each specific kind [8].
Various methods of fixation are also documented in the literature and are shown in Table 1. According to Gao et al [5], using a locking plate with cannulated or lag screws for medial Hoffa fracture fixation appears to be a reliable and effective method for attaining proper alignment and producing outstanding functional outcomes when paired with intensive rehabilitation. Based on biomechanical study [9], the lateral plate fixation offers superior stiffness and load capacity before failure, as well as little displacement for the posterior condylar fragments. The posterior plate fixation comes next in terms of these factors.
The screws put in the AP direction had the lowest levels of stiffness and ultimate load, while exhibiting the highest level of vertical displacement. Xu et al [10] documented a group of 11 patients who had type III coronal plane fractures of the femoral condyle, with 3 of them also having medial Hoffa fractures. These patients were treated with 3-screw fixation. A single screw was introduced via the femoral intercondylar notch, while the remaining 2 screws were placed through the nonarticular surface of either the lateral or medial condylar fragment. Somford et al [11] showed that the stability of absorbable screws was weak, and that the application of significant shear stress due to knee joint movement raised the likelihood of screw fracture. We used medial parapatellar approach lag screw fixation because we believed it would decrease and align the fracture anatomically, minimize blood loss and soft-tissue injury, and preserve the patient’s functional activity. However, lag screws alone may not stabilize osteoporotic bone, and reinforcing plates may be superior biomechanically [5].
Additionally, the arthroscopic treatment of medial femoral condylar coronal fractures is also discussed in the literature [12,13]. We utilized a surgical technique called medial parapatellar approach to access the fracture site. We employed non-parallel lag screws in a retrograde manner to accomplish precise alignment and compression of the medial Hoffa fracture, ensuring proper anatomical restoration. To enable early movement of the knee joint, we positioned the screws in the back and inner part of the femoral condyle, away from the joint itself. The patient had poliomyelitis and had a weakened limb on the opposite side, but demonstrated complete mobility in the operated limb throughout both short-term and long-term evaluations.
Conclusions
Medial Hoffa fracture is a frequently overlooked injury that requires a systematic approach and an appropriate fixation method based on the new classification system. We treated a patient with post-polio syndrome who sustained a medial Hoffa fracture, due to osteoporosis associated with post-polio syndrome, this fracture could be considered as a fragility fracture. We performed open reduction and internal fixation using lag screws through a medial parapatellar approach, which is a common technique for Hoffa fractures. However, we acknowledge that lag screws alone may not provide sufficient stability for osteoporotic bone, and that other fixation methods, such as reinforcement plates, may offer better biomechanical outcomes. We chose lag screws fixation via the me-dial parapatellar approach only because we believed it would achieve anatomical reduction and alignment of the fracture and would minimize the soft-tissue damage and blood loss taking into consideration the patient’s functional level of activity. We also followed the patient closely and monitored the postoperative period, fracture healing, and stepwise rehabilitation program. We did not encounter any surgical-site or any hardware-related complications. We agree that the choice of fixation method for Hoffa fractures depends on several factors, such as the fracture type, the bone quality, the surgical approach, and the patient’s condition and pre-injury functional level. We suggest that future studies should compare the different fixation options and evaluate their long-term results.
Our patient had with a severe form of polio, experiencing difficulties in early weight bearing owing to weakness on the opposite side caused by polio. We performed a basic anatomical fixation without substantial plating in this patient because of the lower demand and the requirement for slow rehabilitation. Despite the challenges, we achieved a complete functional result, which is remarkable in this particular instance. The combination of medial Hoffa and polio in a patient is a challenging and unusual situation that requires careful and astute judgment.
Figures
References:
1.. Arastu MH, Kokke MC, Duffy PJ, Coronal plane partial articular fractures of the distal femoral condyle: Current concepts in management: Bone Joint J, 2013; 95(9); 1165-71
2.. Zhou Y, Pan Y, Wang Q, Hoffa fracture of the femoral condyle: Injury mechanism, classification, diagnosis, and treatment: Medicine (Baltimore), 2019; 98(49); e14633
3.. Viskontas DG, Nork SE, Barei DP, Technique of reduction and fixation of unicondylar medial Hoffa fracture: Am J Orthop (Belle Mead NJ), 2010; 39(9); 424-28
4.. Roos EM, Lohmander LS, The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis: Health Qual Life Outcomes, 2003; 1; 64
5.. Gao M, Tao J, Zhou Z, Surgical treatment and rehabilitation of medial Hoffa fracture fixed by locking plate and additional screws: A retrospective cohort study: Int J Surg, 2015; 19; 95-102
6.. Patel PB, Tejwani NC, The Hoffa fracture: Coronal fracture of the femoral condyle a review of literature: J Orthop, 2018; 15(3); 726-31
7.. Pires RE, Bidolegui F, Pereira S, Medial Hoffa fracture: Description of a novel classification system and rationale for treatment based on fragment-specific fixation strategy: Z Orthop Unfall, 2020; 160(3); 269-77
8.. Bagaria V, Sharma G, Waghchoure C, A proposed radiological classification system of Hoffa’s fracture based on fracture configuration and consequent optimal treatment strategy along with the review of literature: SICOT J, 2019; 5; 18
9.. Ercin E, Bilgili MG, Basaran SH, Arthroscopic treatment of medial femoral condylar coronal fractures and nonunions [published correction appears in Arthrosc Tech. 2014;3(1): e103]: Arthrosc Tech, 2013; 2(4); e413-e15
10.. Lal H, Bansal P, Khare R, Conjoint bicondylar Hoffa fracture in a child: A rare variant treated by minimally invasive approach [published correction appears in J Orthop Traumatol. 2011;12(4): 237]: J Orthop Traumatol, 2011; 12(2); 111-14
11.. Sun H, He QF, Huang YG, Plate fixation for Letenneur type I Hoffa fracture: A biomechanical study [published correction appears in Injury. 2017;48(10): 2365]: Injury, 2017; 48(8); 1492-98
12.. Xu Y, Li H, Yang HH, A comparison of the clinical effect of two fixation methods on Hoffa fractures [published correction appears in Springerplus. 2016;5(1) 2032]: Springerplus, 2016; 5(1); 2023
13.. Kapoor C, Merh A, Shah M, A case of distal femur medial condyle Hoffa Type II© fracture treated with headless screws: Cureus, 2016; 8(11); e802
14.. Ozan F, Okur KT, Ünlü ÖC, Corrective osteotomy for coronal plane mal-union of the medial femoral condyle: Cureus, 2018; 10(12); e3222
15.. Sasidharan B, Shetty S, Philip S, Reconstructive osteotomy for a malunited medial Hoffa fracture – a feasible salvage option: J Orthop, 2016; 13(2); 132-35
16.. AlKhalife YI, Alshammari AN, Abouelnaga MA, Hoffa’s fracture of the medial femoral condyle in a child treated with open reduction and internal fixation: A case report: Trauma Case Rep, 2018; 18; 20-26
17.. Holmes SM, Bomback D, Baumgaertner MR, Coronal fractures of the femoral condyle: A brief report of five cases: J Orthop Trauma, 2004; 18(5); 316-19
18.. Chang JJ, Fan JC, Lam HY, Treatment of an osteoporotic hoffa fracture: Knee Surg Sports Traumatol Arthrosc, 2010; 18(6); 784-86
19.. Miyamoto R, Fornari E, Tejwani NC, Hoffa fragment associated with a femoral shaft fracture: a case report: J Bone Joint Surg Am, 2006; 88(10); 2270-74
20.. Ocguder A, Bozkurt M, Kalkan T, Hoffa fracture, eminentia fracture and posterior cruciate ligament damage: An unusual knee injury: Injury Extra, 2008; 39(10); 344-47
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133