08 August 2025: Articles 
Deep-Brain Stimulation and Intensive Rehabilitation in a Patient with Parkinson Disease: A Case Report
Unusual setting of medical care
Giorgio FerrieroDOI: 10.12659/AJCR.946308
Am J Case Rep 2025; 26:e946308






Abstract
BACKGROUND: Parkinson disease (PD) is a common neurodegenerative disease. Intensive rehabilitation programs improve motor and non-motor symptoms in people with PD. Quite recently, deep-brain stimulation (DBS) has become an established therapeutic tool for treating patients with a disease who have troublesome motor fluctuations and dyskinesias refractory to best medical therapy.
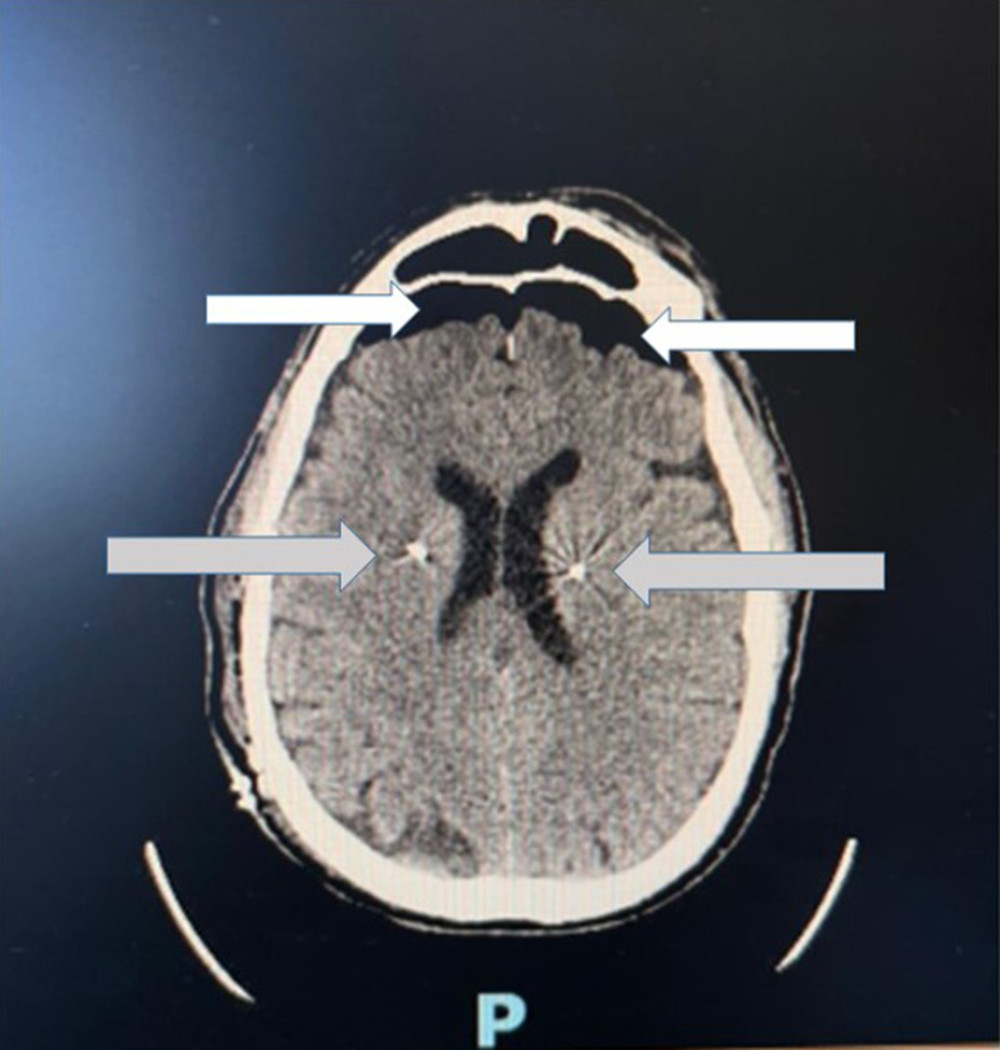
CASE REPORT: A 56-year-old man affected by PD with motor complications was admitted to undergo deep-brain stimulation. After the operation, he was transferred to the Intensive Rehabilitation Department and received multidrug therapy. First, we tried to optimize the pharmacological therapy. To achieve this goal, we performed a physiatric evaluation with the device turned off. We set up an Individual Rehabilitation Project with active kinesitherapy for maintaining the strength and muscular resistance of the shoulder and pelvic girdle, upper limbs, and lower limbs, exercises to improve trunk stability and balance reactions, exercises to improve motor coordination and static and dynamic balance, gait training with gait pattern, training for climbing and descending stairs, and functional re-education. For the headache, we requested a magnetic resonance imaging (MRI) of the brain, that showed the correct positioning of the electrodes bilaterally, with the identification of a moderate amount of air (pneumocephalus). At the same time, adjustment/switching on of the stimulator was carried out, which was well tolerated, adjusting the stimulation parameters of the sensors both on the right and left during hospitalization and gradually modifying the pharmacological therapy.
CONCLUSIONS: The combination of internal-geriatric expertise together with the collaboration between neurologist and physiatrist are fundamental for management of these patients. Intensive rehabilitation is ideal for these subjects before discharge and subsequent post-procedural follow-up.
Keywords: Drug Combinations, Geriatricians, Parkinson Disease, Physiatrists, Pneumocephalus, Rehabilitation, Humans, Male, Deep Brain Stimulation, Middle Aged, Exercise Therapy
Introduction
Parkinson disease (PD) is a common neurodegenerative disease with incidence ranging from 5/100 000 to over 35/100 000 new cases yearly, which increases 5- to 10-fold from the sixth to the ninth decades of life [1]. Advances in the medical management of PD have led to longer lives. This has resulted in increased disability secondary to the presence of motor and non-motor symptoms, leading to progressive handicap and a reduction in the quality of life (QoL) of patients [2,3]. Progression of the disease, as well as the daily levodopa dose, were reported to be associated with so-called ‘levodopa-induced’ motor complications, with a modification of levodopa responsiveness with disease progression [4]. Intensive rehabilitation programs can improve motor and non-motor symptoms in people with PD. Quite recently, deep-brain stimulation (DBS) has become an established therapeutic tool for treating patients with PD who have motor fluctuation problems and dyskinesias refractory to best medical therapy, as demonstrated by data from the EARLYSTIM trial [5]. The implantation of the deep-brain stimulator is performed at our center according to a validated protocol. We present with this clinical case report an emblematic example of our daily experience with these patients.
Case Report
Our patient was a 56-year-old man with PD, living with his wife in a house without internal stairs or other physical obstacles. His PD symptoms began in 2016 with akinesia and rigidity in the right side of the body, and he had motor complications (disabling dyskinesias in the right hemilate, mostly at the level of the upper limbs). He had a medical history of ischemic heart disease and underwent angioplasty and drug-eluting stent placement in 2019. In 2014 he underwent surgery for carpal tunnel syndrome and Dupuytren’s disease on the right, and in 2024 was admitted to undergo DBS. After the operation, he was transferred to the Intensive Rehabilitation Department (this type of rehabilitation setting in Italy has a numeric code of 56) with the following drug therapy: rasagiline 1 mg, triesifenidile 4 mg, levodopa/benserazide 200/50 mg 1 tablet in the early morning (5: 30), 3/4 tablet at 10: 00, 1 tablet at 13: 00, 1 tablet at 16: 00, half a tablet at 19: 00, levodopa/benserazide 100/25 mg prolonged release 2 tablets at bedtime, rosuvastatine 10 mg, valsartan 160 mg, macrogol 3350 mg, pantoprazole 20 mg, and ASA 100 mg. The psychiatric evaluation showed (with the DBS device turned off, in the off phase, in the process of optimizing the pharmacological therapy) a hematoma in the right subclavicular region, which was not painful or tender to palpation at the stimulator implant site. He was in good general condition, oriented in the 3 axes, cooperative, and reported having headache. He exhibited spontaneous, hypophonic, congruous, and informative speech, with dyskinesias at the level of the perioral and mimic muscles. The subject reported decreased salivation in the absence of swallowing disorders. He correctly performed the index-nose and heel-knee test. He remained autonomy in common life activities, and was able to independently perform postural transitions and transfers with adaptations. Standing static was possible independently with multidirectional oscillations, which were major on the left. Independently walking was possible with a slightly widened base and slight forward position of the trunk, with pendulum synkinesis of the limbs. There were diffuse dystonias in the face, head, neck, and upper limbs bilaterally. He had free and painful cervical range of motions during rotations. The upper limbs were normally positioned, and he was able to reach and maintain the anti-gravity position bilaterally without leveling. There were major distal fine tremors on the right side. The articulation of the main joint fulcrums was normal, except for plastic hypertonicity at the level of elbow flexion and extension bilaterally, especially on the right side. Then, we evaluated muscle strength and from the evaluation of the individual muscle groups, which was 4/5 according to the Medical Research Council (MRC) system. There was no bilateral manual dexterity deficit. We evaluated the patients’ manual grasp and it was normal. The grasp of the digito-palmar forceps was also good. Bradykinesia and dyskinesia were present on finger tapping, with rapid and symmetrical alternating movements. The bicipital reflexes were normal and symmetrical. The lower limbs were in normal position; they reached and maintained the anti-gravity position bilaterally without leveling. Articulation of the main joint fulcrums was normal. Strength globally evaluable at 4/5 according to the MRC system. There was no bradykinesia. The reflexes of the patella were normal and symmetrical. The plantar cutaneous reflex was present in extension on the right side, and not evocable on the left. The protopathic and epicritic tactile sensitivities were preserved on all explored dermatomes. Cortical functions were apparently normal (Mini-Mental State Examination in the normal range values). Sphincter control was preserved. The main disability was difficulty in mobility, balance, walking, and fine manual motor skills. We set up an Individual Rehabilitation Project (PRI) with active kinesitherapy for maintaining the strength and muscular resistance of the shoulder and pelvic girdle, and upper limbs and lower limbs, as well as exercises to improve trunk stability and balance reactions, exercises to improve motor coordination and static and dynamic balance, gait training with gait pattern, training for climbing and descending stairs, and functional re-education. For the headache, we requested an MRI scan of the brain, which showed correct positioning of the electrodes bilaterally, with the identification of a moderate amount of air (pneumocephalus) bilaterally at the frontal level, with a probable iatrogenic etiology (surgical intervention for the positioning of the electrodes themselves) (Figure 1), so ibuprofen 40 mg was administered, with clinical efficacy. A logopedic rehabilitation program was started, and he also had occupational therapy sessions in which he performed fine manual skills and hand-eye coordination exercises. All the various phases took place under physiotherapy and nursing supervision to ensure safe transfer training. At the same time, adjustment/switching on of the stimulator was carried out, which was well tolerated. We adjusted the stimulation parameters of the sensors on the right and left during hospitalization and gradually modified the pharmacological therapy (suspension of rasagiline; start of quetiapine 12.5 mg bedtime, down-titration of levodopa/benserazide), with good compensation of motor symptoms, persistence of slight akinesia in the right side of the body, improvement of autonomy in activities of daily living and in mobility activities (increase in the distance covered in the 6-minute walking test), better control of dyskinesias, bradykinesia, and better symptomatic control during periods when motor and non-motor symptoms of the disease reappear or worsen, due to the decreased effect of levodopa (periods called OFF phases). He had improvement of muscle tone and trophism and trunk control (maximal trunk control test).
Discussion
This case report shows value of cooperation of the various professionals involved in patient care: neurologists, physiatrists, geriatricians, physiotherapists, speech therapists, occupational therapists, and nurses. Among motor disturbances, postural instability is particularly important because it is associated with increased risk of falls and loss of self-sufficiency, especially in older patients [6]. DBS may improve postural control and can even aggravate this imbalance, depending on the improvement or worsening of the location of the electrodes at the level of different brain areas [7]. However, there is also evidence that exercise in patients with PD can improve postural balance and non-motor symptoms (eg, autonomic dysfunction, cognitive decline, and sleep and mood disorders), and can improve quality of life [8]. A retrospective study by Chevrier et al confirmed the beneficial effects of physiotherapy in this group of PD patients [9]. A recent case-control study suggests that rhythmic auditory stimulation (RAS)-program-assisted gait training plus conventional physiotherapy is a useful strategy to improve gait performance in PD patients with and without DBS [10]. Several studies have investigated the impact of DBS on movement and quality of life. A randomized controlled trial by Deuschl et al involving 150 patients with severe motor deficits showed that just 6 months of this treatment improved motor symptoms and quality of life compared to use of drugs alone [11]. This positive experience was replicated for an even longer period (up to 4 years) in a multicenter study conducted on a much smaller cohort of patients, approximately half the size of the previous study [12]. The EARLY-STIM trial showed the superiority of DBS for treating PD patients with early motor complications compared to use of the best oral medications [13]. However, the results are not always optimal or long-lasting, especially when intervention is performed too late, too long after diagnosis of the disease, or in elderly patients [14]. Causes of suboptimal or decidedly unsatisfactory results include: patients having suboptimally placed electrodes, infection or a fractured lead, and an inadequately programmed device, and some patients were given the wrong diagnosis in the first place [15]. A study involving the major Italian centers that use this technique, including ours, has evaluated the “poor stimulation responders” among late-stage PD patients for elaborating an algorithm to decide whether and when DBS discontinuation may be considered [16]. Finally, many centers in Italy have a well-established DBS program for patients with PD and several surveys were conducted, in which our center also participated, to compare different parameters such as the different techniques, the characteristics of the patients treated, and the short and long-term results [17]. The discussed single clinical case report is a good example of the care of patients at our center. A study on data from the center’s activity on all patients who have been treated with DBS and then referred to our intensive rehabilitation service is certainly a commitment to be undertaken [18–20].
Conclusions
Geriatric internal assessment is fundamental in the evaluation of these patients, both in clinical surveillance and in decisions regarding the appropriate dose of anti-Parkinsonian drug therapy and in the evaluation of the results achieved, as well as in the management of the patient’s other comorbidities (ischemic heart disease, hypertension) and in the critical evaluation of symptoms (such as for example headaches, identifiable only as a tension-type headache rather than with the co-presence of a pneumocephalus) potentially subject to misinterpretation and therefore poorly managed and treated. Although further studies are necessary to validate a rational protocol that combines neurological interventional procedures with targeted physiotherapy programs, the combination of internal medicine and geriatrics expertise, together with collaboration between neurologists and physiatrists, are fundamental for the management of these patients and that intensive rehabilitation of for this reason represents the ideal setting for these subjects before discharge and subsequent post-procedural follow-up. Finally, the DBI was well tolerated by our patient, who showed satisfaction with the results achieved, both through the procedure and with the physiotherapy treatments carried out in our center (studies are underway to verify the overall level of satisfaction of patients treated at our polyclinic), confirming the validity and effectiveness of the process.
References
1. Simon DK, Tanner CM, Brundin P, Parkinson disease epidemiology, pathology, genetics, and pathophysiology: Clin Geriatr Med, 2020; 36(1); 1-12
2. Ellis TD, Colón-Semenza C, DeAngelis TR, Evidence for early and regular physical therapy and exercise in Parkinson’s disease: Semin Neurol, 2021; 41(2); 189-205
3. GBD 2016 Parkinson’s Disease Collaborators, Global, regional, and national burden of Parkinson’s disease, 1990–2016. A systematic analysis for the Global Burden of Disease Study 2016: Lancet Neurol, 2018; 17(11); 939-53
4. Cilia R, Cereda E, Akpalu A, Natural history of motor symptoms in Parkinson’s disease and the long-duration response to levodopa: Brain, 2020; 143(8); 2490-501
5. Pinto S, Nebel A, Rau JEARLYSTIM Study Group, Results of a randomized clinical trial of speech after early neurostimulation in Parkinson’s disease: Mov Disord, 2023; 38(2); 212-22
6. Pickering RM, Grimbergen YA, Rigney U, A meta-analysis of six prospective studies of falling in Parkinson’s disease: Mov Disord, 2007; 22(13); 1892-900
7. Collomb-Clerc A, Welter ML, Effects of deep brain stimulation on balance and gait in patients with Parkinson’s disease: A systematic neurophysiological review: Neurophysiol Clin, 2015; 45(4–5); 371-88
8. Ernst M, Folkerts AK, Gollan R, Physical exercise for people with Parkinson’s disease: A systematic review and network meta-analysis: Cochrane Database Syst Rev, 2023; 1(1); CD013856
9. Chevrier E, Fraix V, Krack P, Is there a role for physiotherapy during deep brain stimulation surgery in patients with Parkinson’s disease?: Eur J Neurol, 2006; 13(5); 496-98
10. Naro A, Pignolo L, Sorbera C, A case-controlled pilot study on rhythmic auditory stimulation-assisted gait training and conventional physiotherapy in patients with Parkinson’s disease submitted to deep brain stimulation: Front Neurol, 2020; 11; 794
11. Deuschl G, Schade-Brittinger C, Krack PGerman Parkinson Study Group, Neurostimulation Section, A randomized trial of deep-brain stimulation for Parkinson’s disease: N Engl J Med, 2006; 355(9); 896-908
12. Rodriguez-Oroz MC, Obeso JA, Lang AE, Bilateral deep brain stimulation in Parkinson’s disease: A multicentre study with 4 years follow-up: Brain, 2005; 128(Pt 10); 2240-49
13. Hacker ML, Turchan M, Heusinkveld LE, Deep brain stimulation in early-stage Parkinson disease: Five-year outcomes: Neurology, 2020; 95(4); e393-e401
14. Zheng Y, Wei L, Ang SYL, Outcomes after deep brain stimulation for elderly versus non-elderly patients with Parkinson’s disease: Clin Neurol Neurosurg, 2024; 242; 108319
15. Hariz MI, What is deep brain stimulation “failure” and how do we manage our own failures?: Arch Neurol, 2005; 62(12); 1938 author reply 1938–39
16. Fabbri M, Zibetti M, Rizzone MG, Should we consider deep brain stimulation discontinuation in late-stage Parkinson’s disease?: Mov Disord, 2020; 35(8); 1379-87
17. Mancini F, Guzzi G, Castrioto CF, Deep brain stimulation for Parkinson’s disease in practice: Results of the survey by the Italian Neurosurgery Society: J Neurosurg Sci, 2022; 66(6); 526-34
18. Bertolini C, Nigito C, Ronconi GPThe role of occupational therapy in rehabilitating injured at work: G Ital Med Lav Ergon, 2010; 32(4 Suppl); 172 [in Italian]
19. Genovese D, Bove F, Rigon L, Long-term safety and efficacy of frameless subthalamic deep brain stimulation in Parkinson’s disease: Neurol Sci, 2024; 45(2); 565-72
20. Izzo A, Piano C, D’Ercole M, Intraoperative microelectrode recording during asleep deep brain stimulation of subthalamic nucleus for Parkinson Disease. A case series with systematic review of the literature: Neurosurg Rev, 2024; 47(1); 342
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133