29 April 2025: Articles 
Secukinumab as a Novel Treatment for Chronic Netherton Syndrome in a Young Adult
Challenging differential diagnosis, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Irma BuchukuriDOI: 10.12659/AJCR.946411
Am J Case Rep 2025; 26:e946411






Abstract
BACKGROUND: Netherton syndrome is an autosomal recessive skin disorder usually diagnosed in infancy and is characterized by ichthyosis, erythroderma, atopy, and characteristic beading of the hair shaft (trichorrhexis invaginata). Secukinumab, a monoclonal antibody that inhibits interleukin-17, has recently been reported to be effective in patients with refractory Netherton syndrome. The present report describes a 20-year-old man with a chronic history of refractory Netherton syndrome who responded to treatment with secukinumab.
CASE REPORT: A 20-year-old male patient presented with generalized pruritus, erythema, and scaling. The patient was previously diagnosed with atopic dermatitis and had been treated with systemic corticosteroids and omalizumab, without improvement. Later, the patient was referred to us. Physical examination showed generalized erythroderma and polycyclic and serpiginous erythematous plaques with double-edged scales at the margins. Trichoscopy of the scalp revealed a hair shaft abnormality, specifically trichorrhexis invaginata. The blood tests demonstrated elevated IgE levels. Initially, the patient was started on topical corticosteroids, which caused the condition to deteriorate. As the patient did not respond to the treatment, a decision was made to start secukinumab monotherapy. After 2 injections, the patient’s condition markedly improved and the effect after the last injection was maintained for 4-5 months.
CONCLUSIONS: Netherton syndrome is a rare and often misdiagnosed hereditary diseases in dermatology. For this reason, the management strategies of the disease are variable and without consensus. In our case, considering the pathogenesis of the disease, we used secukinumab, which has shown promising results and good tolerability. Further studies are required to establish the efficacy of the drug.
Keywords: Hair Diseases, Immunotherapy, Netherton Syndrome, Humans, Male, Antibodies, Monoclonal, Humanized, young adult, Antibodies, Monoclonal, Chronic Disease
Introduction
Netherton syndrome is a rare form of autosomal recessive disease of the skin, which is classically characterized by a triad of symptoms: hair shaft abnormalities (trichorrhexis invaginata); ichthyosiform erythroderma, later evolving into ichthyosis linearis circumflexa; and elevated serum immunoglobulin E (IgE) levels [1]. The exact pathogenesis of the disease still remains unknown, but it is thought to be an interplay between inflammatory and genetic factors; specifically, a loss-of-function mutation of the SPINK5 gene, responsible for the production of enzymes that control the activity of kallikreins in the skin, which, in turn, control the epidermal cell turnover. The incidence is approximately 1 in 200 000 births and the prevalence is between 1 and 9 per million births [2]. Usually, the disease is misdiagnosed as atopic dermatitis, treated by standard therapy, which often struggles to alleviate the symptoms. The evaluation of severity of the disease is done clinically; however, it can be aided by assessment by the Ichthyosis Area and Severity Index (IASI) [3] and the Netherton Area and Severity Assessment (NASA) [4]. The former is done by evaluating the areas of erythema and scaling on different parts of the body, while the latter assesses erythema, infiltration, scaling, and lichenification of different parts of the body. Each finding is given a score that ranges from 0 to 48 for IASI and 0 to 72 for NASA. A higher number of points correlates with greater severity of the disease.
Recent discoveries [5,6] link the disease pathogenesis to interleukin 17 (IL-17)-mediated inflammation. These reports suggest that the inflammation and scaling that are characteristic of the disease are caused by upregulation and infiltration of Th17 helper T cells in the skin. The present report describes the case of a 20-year-old man with a history of chronic erythroderma, ichthyosis, trichorrhexis invaginata, and atopy, consistent with Netherton syndrome, who responded to treatment with secukinumab, a therapeutic monoclonal antibody inhibitor of IL-17.
Case Report
A 20-year-old man was referred to our clinic complaining of scaling, erythema, and pruritus manifesting itself since infancy and early childhood. The patient was diagnosed with atopic dermatitis and had been treated for it with various treatment regimens without any notable improvement. The exact timeline of symptom development and treatment is unknown. A skin biopsy that the patient had done prior to our consultation showed histologic features of atopic dermatitis, and was inconclusive. Also, the patient reported several bouts of recurrent secondary bacterial infections of the skin, which were treated accordingly.
Prior to our consultation, based on his atopic dermatitis, elevated eosinophil count (880 U/μL; reference range: 30–350 U/μL), and IgE levels (45 000 kU/L; reference range: 100–200 kU/L), the patient had been treated with antihistamines, cyclosporine, and systemic corticosteroids. As the response to treatment was poor, the patient was started on subcutaneous omalizumab, starting at a dose of 600 mg once every 4 weeks for 3 months; later, once every 2 weeks for 5 months. Following the treatment, the degree of pruritus decreased; however, overall symptoms remained unchanged. Approximately 7 months after the last dose of omalizumab injection, which yielded unsatisfying results, the patient was referred to our clinic.
The physical examination showed generalized erythroderma with polycyclic and serpiginous erythematous plaques with double-edged scales at the margins on the face, trunk, and on both upper and lower extremities (Figure 1). Serum IgE levels were also increased (38 550 kU/L). Assessment by IASI and NASA yielded a baseline IASItotal of 34.8 and a baseline NASAtotal of 27.2.
The patient’s history and the clinical presentation were strongly suggestive of severe atopic dermatitis. However, since the persistent erythroderma and its presence since infancy could not be explained solely by atopic dermatitis, we considered another diagnosis as a differential. Another finding during the physical examination was brittle and damaged hair on the patient’s scalp. Thus, we preformed trichoscopy of the scalp that revealed a hair shaft abnormality, specifically invagination of the distal end of the hair shaft into its proximal part, or trichorrhexis invaginata, a highly characteristic trichoscopic feature of Netherton syndrome (Figure 2). DNA sequencing for detection of the SPINK5 gene mutation confirmed the diagnosis of Netherton syndrome. We did not perform a biopsy, as the clinical presentation, trichoscopic findings, and genetic testing were strongly indicative of Netherton syndrome. In addition, there are no documented characteristic histologic features of the syndrome.
The initial treatment regimen for the patient was topical corticosteroid ointment; mometasone furoate twice daily for 2 weeks, then once daily for 1 month; 10 mg cetirizine taken orally once daily for 2 weeks; and moisturizers. Two months later, the patient returned, presenting with multiple vesiculopustular-crusted lesions on the face with yellow-golden colored crusts, resembling that of eczema herpeticum with secondary bacterial infection (Figure 3), consistent with a generalized flare-up of atopic dermatitis, despite the treatment with topical steroids. Serology was performed and showed increased anti-HSV1-IgG antibodies (145 IU/mL). The patient was started on low-dose acyclovir, 400 mg thrice daily for 7 days; amoxicillin-clavulanic acid 500 mg/125 mg twice daily for 7 days; and methylprednisolone 16 mg twice daily for 7 days.
After his condition stabilized, the decision was made to start the patient on secukinumab, as monotherapy. The loading dose regimen was half of the weight-adapted dose for psoriasis: 150 mg at baseline and at weeks 1, 2, 3, and 4, then monthly thereafter [7]. After 2 injections, the general condition of the patient improved, and after 4 injections, scaling and crusting was alleviated (Figure 4). The patient’s IgE levels were measured at the beginning and during the treatment. After the third injection of secukinumab, the levels of IgE and eosinophils dropped to 129 kU/L and 438 U/μL, respectively; IASItotal was 14.4 and NASAtotal was 16.4. Despite the overall symptom improvement, his trichorrhexis invaginata persisted during and after the treatment.
After 5 injections, a maintenance dose was planned. However, the patient did not return for the follow-up visit. The effect achieved by the loading phase of secukinumab lasted for approximately 2 months. Four months after the last dose of secukinumab, the patient returned with the recurrence of generalized scaling, erythema, and pruritus. Re-administration of secukinumab led to remission that lasted for 4–5 months. Further observation of the patient showed no recurrence of symptoms and flare-up of the disease. Also, the patient demonstrated no adverse effects to the treatment.
Discussion
Netherton syndrome is a rare congenital disorder. The clinical manifestations of the disease include hair shaft abnormalities, such as trichorrhexis invaginata, elevated serum IgE levels, and linear ichthyosis, which can be present at birth [1]. The incidence of the disease is approximately 1 in 200 000 births, and the prevalence is 1 to 9 per million births [2].
The pathogenesis of the disease is not fully understood; however, there are some possible explanations for the development of the disease. One of the proposed mechanisms includes gene alterations and dysregulation of the proteases involved in keratinocyte maturation and desquamation [8]. The SPINK5 gene, which is located at chromosome 5q31–32, encodes a serine protease inhibitor called lymphoepithelial Kazal-type inhibitor (LEKTI) [9]. LEKTI is synthesized by a variety of tissues of the body. In the skin, it is produced by the lamellar bodies in the stratum granulosum [10]. Under normal conditions, it regulates desquamation of keratinocytes by countering the group of proteases called kallikreins (KLKs) [11]. An autosomal recessive mutation of the SPINK5 gene can lead to partial or complete loss of function of LEKTI. The decreased quantity or defective production of LEKTI, in turn, causes unopposed activity of KLKs, especially KLK5, KLK7, and KLK14, leading to proteolytic destruction and the premature breakage of the corneodesmosomal junction at the level of the stratum corneum, abnormal desquamation, and development of ichthyosiform skin lesions in Netherton syndrome patients [12]. LEKTI is also responsible for inhibiting intracellular signaling molecules, the most relevant of them being caspase 14 [13]. It is thought to be one of the important mediators regulating the process of cornification. The disruption of this process can contribute not only to abnormal desquamation, but also hair shaft abnormalities. Another mechanism contributing to Netherton syndrome, attributed to LEKTI, is the upregulation of inflammatory cytokines in the epidermis, promoting the inflammation seen during the disease [14]. There is ongoing research on a drug that selectively inhibits KLK5, thus countering the activity of the cascade of enzymes and improving the general condition of Netherton syndrome. The results of the study have yet to be published [15].
The most common lymphocytes upregulated in Netherton syndrome often include Th2 helper T cells [1]. Consequently, the events of their activation, including the upregulation of IL-4 and IL-13 and the overproduction of IgE, can result in outcomes resembling atopic dermatitis [16]. Thus, drugs that decrease the effect of these mediators have commonly been used to control the symptoms of Netherton syndrome [5].
A more recent link to Netherton syndrome pathogenesis is tied to the IL-17 pathway [5]. The disease was found to have pathogenesis resembling that of psoriasis [11]. Th17 cells, which are the predominant lymphocytes in psoriatic plaques, are also upregulated in the epidermal layer of the skin in Netherton syndrome patients [6]. IL-17 and its isoforms, such as IL-17A and IL-17F, cause a signal cascade activation that leads to prominent inflammation of the skin, keratinocyte hyperplasia, and impaired barrier function, thus increasing susceptibility to infections [17].
The diagnosis of Netherton syndrome is mostly based on clinical and laboratory findings, as there are no described specific histological characteristics. Genetic testing usually confirms the diagnosis [6,11,17]. In our case, what raised suspicion of the syndrome was the presence of trichorrhexis invaginata, a hair shaft disorder that is a highly specific trichoscopic finding in patients with Netherton syndrome [18].
There is no specific treatment for the disease. The standard management for Netherton syndrome is the daily use of moisturizers to maintain the barrier function of the skin and decrease transepidermal water loss [19,20]. Due to an impaired skin barrier, patients with Netherton syndrome are susceptible to secondary infections and sometimes require oral antibiotics [21].
A systemic treatment option for Netherton syndrome is the use of systemic retinoids [22]. Due to their anti-keratinizing effect, systemic retinoids can provide some relief to patients with Netherton syndrome [6]. The most common systemic retinoids used to treat the disease are acitretin, isotretinoin, alitretinoin, and etretinate. However, the efficacy of treatment is not fully established, and the outcomes vary among patients. Another treatment for the disease is systemic prednisone [23]. Due to its anti-inflammatory activity, it is a good option for the control of inflammation. However, the risks of adverse effects from long-term use outweigh the benefits [24].
Certain biologicals have been used in patients with Netherton syndrome. Even though the disease symptoms, presentation, and outcomes are variable, targeting certain inflammatory cytokines such as TNF-alpha (adalimumab, infliximab) [25], IL-4 and IL-13 (dupilumab) [26], IgE (omalizumab) [24], IL-12 and IL-23 (ustekinumab) [27], and IL-17 (secukinumab, ixekizumab) [28] can lead to beneficial outcomes. Secukinumab has been used in several cases for the treatment for Netherton syndrome [29–31]. By selectively blocking IL-17, the degree of inflammation and scaling is decreased. In our case, the patient, who was previously treated with omalizumab and systemic corticosteroids without success, has shown a dramatic improvement after secukinumab. The patient also did not report any adverse effects of the drug, including the commonly observed ones, such as fungal infections, fatigue, or nasopharyngitis [32]. Various doses of secukinumab injections have been used in different case reports of Netherton syndrome; we used the the wight-adjusted dose that is used for psoriasis [7]. The effect achieved by the drug lasted for several weeks and with little to no adverse effects reported by the patient. It is worth mentioning that the patient showed no signs of secondary bacterial or fungal infection throughout the treatment with secukinumab.
Conclusions
Netherton syndrome is one of the rare hereditary diseases in dermatology. Due to its low incidence and prevalence and the fact that there are only a few cases reported, the disease lacks a standardized management strategy. Based on what is known regarding the pathogenesis of the disease, our decision to use secukinumab, an IL-17 inhibitor, as a treatment proved effective and well-tolerated. Further studies are required to establish the efficacy and tolerability of secukinumab in the management of Netherton syndrome.
Figures
 Figure 1. Generalized erythema with polycyclic and serpiginous erythematous plaques with double-edged scales at the margins. Photos taken during the initial examination.
Figure 1. Generalized erythema with polycyclic and serpiginous erythematous plaques with double-edged scales at the margins. Photos taken during the initial examination. 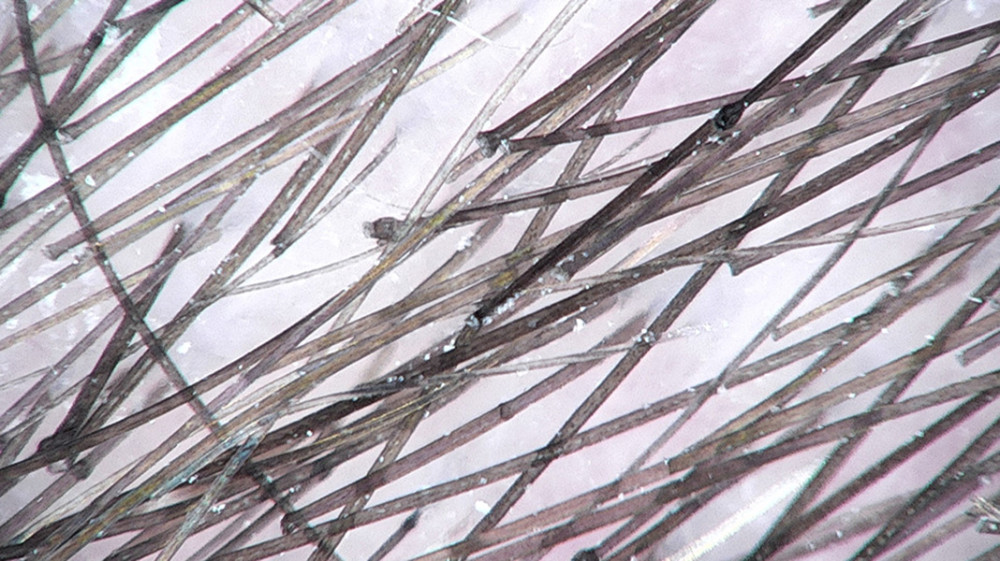 Figure 2. Trichoscopic photo showing trichorrhexis invaginata (bamboo hair), a condition in which the hair shaft invaginates into itself.
Figure 2. Trichoscopic photo showing trichorrhexis invaginata (bamboo hair), a condition in which the hair shaft invaginates into itself.  Figure 3. Picture of the patient’s face with eczema herpeticum showing erythema, swelling, white to yellow-golden crusts and pustulation.
Figure 3. Picture of the patient’s face with eczema herpeticum showing erythema, swelling, white to yellow-golden crusts and pustulation.  Figure 4. Pictures of the patient after 2 injections of secukinumab. The patient demonstrated mild erythema without scales or plaques.
Figure 4. Pictures of the patient after 2 injections of secukinumab. The patient demonstrated mild erythema without scales or plaques. References
1. Briot A, Deraison C, Lacroix M, Kallikrein 5 induces atopic dermatitis-like lesions through PAR2-mediated thymic stromal lymphopoietin expression in Netherton syndrome: J Exp Med, 2009; 206; 1135-47
2. Dey V, Netherton syndrome: A rare genodermatosis: Indian Dermatol Online J, 2011; 2; 38
3. Samuelov L, Shehadeh W, Sarig O, Ustekinumab therapy for Netherton syndrome: J Dermatol, 2023; 50; 494-99
4. Martin-García C, Godoy E, Cabrera A, Report of two sisters with Netherton syndrome successfully treated with dupilumab and review of the literature: Int J Immunopathol Pharmacol, 2023; 37; 03946320231172881
5. Pontone M, Giovannini M, Filippeschi C, Biological treatments for pediatric Netherton syndrome: Front Pediatr, 2022; 10; 1074243
6. Ecoeur F, Weiss J, Kaupmann K, Antagonizing retinoic acid-related-orphan receptor gamma activity blocks the T Helper 17/interleukin-17 pathway leading to attenuated pro-inflammatory human keratinocyte and skin responses: Front Immunol, 2019; 10; 577
7. Langley RG, Elewski BE, Lebwohl M, Secukinumab in plaque psoriasis – results of two phase 3 trials: N Engl J Med, 2014; 371; 326-38
8. Komatsu N, Takata M, Otsuki N, Elevated stratum corneum hydrolytic activity in Netherton syndrome suggests an inhibitory regulation of desquamation by SPINK5-derived peptides: J Invest Dermatol, 2002; 118; 436-43
9. Descargues P, Deraison C, Bonnart C, Spink5-deficient mice mimic Netherton syndrome through degradation of desmoglein 1 by epidermal protease hyperactivity: Nat Genet, 2005; 37; 56-65
10. Hovnanian A, Netherton syndrome: Skin inflammation and allergy by loss of protease inhibition: Cell Tissue Res, 2013; 351; 289-300
11. Tartaglia-Polcini A, Bonnart C, Micheloni A, SPINK5, the defective gene in Netherton syndrome, encodes multiple LEKTI isoforms derived from alternative pre-mRNA processing: J Invest Dermatol, 2006; 126; 315-24
12. Sakabe J, Yamamoto M, Hirakawa S, Kallikrein-related Peptidase 5 functions in proteolytic processing of profilaggrin in cultured human keratinocytes: J Biol Chem, 2013; 288; 17179-89
13. Deraison C, Bonnart C, Lopez F, LEKTI fragments specifically inhibit KLK5, KLK7, and KLK14 and control desquamation through a pH-dependent interaction: Mol Biol Cell, 2007; 18; 3607-19
14. Ng E, Hale CS, Meehan SA, Cohen DE, Netherton syndrome with ichthyosis linearis circumflexa and trichorrhexis invaginatum: Dermatol Online J, 2014; 20; 13030/qt7m95t6v6
15. Liddle J, Beneton V, Benson M, A potent and selective kallikrein-5 inhibitor delivers high pharmacological activity in skin from patients with Netherton syndrome: J Invest Dermatol, 2021; 141; 2272-79
16. Kaminishi K, Flow cytometric analysis of IL-4, IL-13 and IFN-γ expression in peripheral blood mononuclear cells and detection of circulating IL-13 in patients with atopic dermatitis provide evidence for the involvement of type 2 cytokines in the disease: J Dermatol Sci, 2002; 29; 19-25
17. Wang C, He D, Shi C, SIRT5 reduces the inflammatory response and barrier dysfunction in IL-17A-induced epidermal keratinocytes: Allergol Immunopathol (Madr), 2023; 51; 30-36
18. Bittencourt MDJS, Moure ERD, Pies OTC, Trichoscopy as a diagnostic tool in trichorrhexis invaginata and Netherton syndrome: An Bras Dermatol, 2015; 90; 114-16
19. Barbati F, Giovannini M, Oranges T, Netherton syndrome in children: Management and future perspectives: Front Pediatr, 2021; 9; 645259
20. Erickson TR, Murphrey MB, Abu-Zayed H, Transepidermal water loss in the orphan forms of ichthyosis: Pediatr Dermatol, 2020; 37; 771-73
21. Eränkö E, Ilander M, Tuomiranta M, Immune cell phenotype and functional defects in Netherton syndrome: Orphanet J Rare Dis, 2018; 13; 213
22. Nouwen AEM, Schappin R, Nguyen NT, Outcomes of systemic treatment in children and adults with Netherton syndrome: A systematic review: Front Immunol, 2022; 13; 864449
23. Hausser I, Anton-Lamprecht I, Hartschuh W, Petzoldt D, Netherton’s syndrome: Ultrastructure of the active lesion under retinoid therapy: Arch Dermatol Res, 1989; 281; 165-72
24. Yalcin AD, A case of netherton syndrome: successful treatment with omalizumab and pulse prednisolone and its effects on cytokines and immunoglobulin levels: Immunopharmacol Immunotoxicol, 2016; 38; 162-66
25. Almalki Y, Khan F, Naeem A, Alabdulghany MH, Netherton syndrome, a rare genetic disorder – case report: Dr Sulaiman Al Habib Med J, 2023; 5(1); 29-32
26. Yan S, Wu X, Jiang J, Dupilumab improves clinical symptoms in children with Netherton syndrome by suppressing Th2-mediated inflammation: Front Immunol, 2022; 13; 1054422
27. Volc S, Maier L, Gritsch A, Successful treatment of Netherton syndrome with ustekinumab in a 15-year-old girl: Br J Dermatol, 2020; 183; 165-67
28. Murashkin NN, Opryatin LA, Bridan-Rostovskaya AS, Results of combined pathogenetic therapy in Netherton syndrome: Clinical case: Curr Pediatr, 2023; 22; 433-42
29. Blanchard SK, Prose NS, Successful use of secukinumab in Netherton syndrome: JAAD Case Rep, 2020; 6; 577-78
30. Luchsinger I, Knöpfel N, Theiler M, Secukinumab therapy for Netherton syndrome: JAMA Dermatol, 2020; 156; 907
31. Gan C, King E, Orchard D, Secukinumab use in the treatment of Netherton’s syndrome: Australas J Dermatol, 2022; 63; 365-67
32. Oguz Topal I, Baysak S, Altunay İK, Evaluation of the efficacy, safety, and side effects of secukinumab in patients with moderate-to-severe psoriasis: Real-world data from a retrospective multicenter study: An Bras Dermatol, 2022; 97; 566-74
Figures
Figure 1. Generalized erythema with polycyclic and serpiginous erythematous plaques with double-edged scales at the margins. Photos taken during the initial examination.Figure 2. Trichoscopic photo showing trichorrhexis invaginata (bamboo hair), a condition in which the hair shaft invaginates into itself.Figure 3. Picture of the patient’s face with eczema herpeticum showing erythema, swelling, white to yellow-golden crusts and pustulation.Figure 4. Pictures of the patient after 2 injections of secukinumab. The patient demonstrated mild erythema without scales or plaques. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133