21 May 2025: Case Reports 
Non-Adjacent Bilateral Postherpetic Neuralgia in a Multiple Myeloma Patient: A Case Report
Unusual clinical course, Rare disease
Hua ZhangDOI: 10.12659/AJCR.946562
Am J Case Rep 2025; 26:e946562






Abstract
BACKGROUND: Postherpetic neuralgia is a refractory neuropathic pain that persists after healing from an acute herpes zoster infection. The pain is often perceived as a sensation akin to needling, cauterization, or electric shock. Clinically, it often manifests with unilateral onset, whereas patients with different sides and multiple segments of postherpetic neuralgia have not yet been reported. Owing to the incompletely elucidated pathogenesis, the therapeutic effects of currently available treatments in different patients are heterogenous, resulting in enormous pain. The risk factors for PHN include age >60 years, malignant tumors, diabetes, and immune dysfunction.
CASE REPORT: We report a case of a 65-year-old man with multiple myeloma who developed left T3 and right T11 postherpetic neuralgia. We used drugs as the basic treatment and then combined nerve pulse radio frequency, nerve block, and other treatments. After discharge, we followed up the patient for 3 months, gradually reducing the dose to wean the patient off the drug treatment, and intermittent pain occasionally occurred. The numerical rating scale score was 0-1 points, which is pain that does not affect daily activities or sleep.
CONCLUSIONS: We report a rare case of postherpetic neuralgia with multiple myeloma occurring on different sides, but not on adjacent nerve segments. We performed left T3 and right T11 nerve pulse radiofrequency surgery, after poor drug treatment efficacy, followed by postoperative nerve block therapy; then, the patient’s pain had been effectively controlled. We hope that our case can provide reference for doctors who encounter similar cases in the future.
Keywords: Multiple Myeloma, Neuralgia, Postherpetic, Neurology, Humans, Male, Aged, Nerve Block
Introduction
Postherpetic neuralgia (PHN) is a neuropathic pain caused by the activation of varicella zoster virus (VZV), which persists after the healing of skin rashes and blisters. The most common symptoms occur in the chest, followed by the neck, head, face, and lower waist [1]. The pain is often perceived as a sensation akin to needling, cauterization, or electric shock, most of which is unilateral or adjacent to 2 spinal cord segments. Currently, few cases of PHN in bilateral and non-adjacent segments have been reported. As the mechanism of PHN is not fully elucidated and mainly involves central and peripheral sensitization, inflammatory reactions, denervation, and sympathetic dysfunction, there is no optimal treatment method, and the efficacies of these treatments are inconsistent. Patients often experience physical and mental health problems. Currently, the mainstream recommended treatment for PHN is based on various drug therapies, such as calcium channel modulators, tricyclic antidepressants, and local sodium channel blockers [1,2]. Treatment of PHN often requires a combination of multiple minimally invasive treatment techniques, including neuraxial glucocorticoid infusion, nerve block, nerve pulse radio frequency, nerve destruction, percutaneous spinal cord electrical stimulation, and intrathecal morphine pump [3–5].
Herein, we report the case of non-ipsilateral and non-adjacent multi-segment thoracic PHN with multiple myeloma. After repeatedly administering various medications, with poor therapeutic effects, we ultimately implemented nerve pulse radiofrequency based on the currently accepted treatment approach, achieving significant therapeutic benefits.
Case Report
DISEASE CHARACTERISTICS:
A 65-year-old man received a diagnosis of herpes zoster at another hospital approximately 3 months earlier, due to a rash and blisters on the left chest and back, right abdomen, and back, with intermittent needling-like pain which distributed along the intercostal nerves in the area of skin lesions. The patient was treated with famciclovir for antiviral therapy, pregabalin for pain relief, and mecobalamin for nutritional nerve therapy. The rash and blisters on the skin were cured; however, there was residual pigmentation (Figure 1A, 1B) and intermittent needling- and burning-like pain that was distributed along the intercostal nerves. The site of pain was consistent with that of herpes zoster, and the degree of pain was severe, affecting daily activities and nighttime sleep. Spontaneous pain occurred dozens of times per day and lasted from a few minutes up to an hour. His numeric rating scale (NRS) score was 3–6 points (based on a scale of 0–10, where 0 indicates no pain and 10 indicates the most severe pain imaginable), indicating that the lesion site was significantly hyperalgesic, without tenderness or rebound pain, and he denied any trauma. No significant abnormalities were noted on spinal examination, including no chest tightness, shortness of breath, coughing, and expectoration. He had a history of multiple myeloma for more than 1 year and had been undergoing chemotherapy at another hospital. One month earlier, he was evaluated using positron emission tomography/computed tomography (PET/CT) and was found to be in a stable condition.
DIAGNOSIS AND DIFFERENTIATION:
After admission, thoracic spine magnetic resonance imaging (MRI) showed no significant abnormalities in the inner and outer spinal canals of the degenerative lesion of the thoracic spine (Figure 2A–2D). Chest CT findings included multiple small nodules scattered in both lungs, as well as chronic inflammatory changes, emphysema, and bullae in both lungs. Cardiac color Doppler ultrasonography indicated an enlarged left atrium, with mild aortic, pulmonary, mitral, and tricuspid regurgitation. Electrocardiography revealed an atrial flutter. Abdominal and urinary system color Doppler ultrasonography showed fatty liver and a 7-mm small stone in the left kidney, respectively. After consultation with cardiovascular physicians, it was believed that there was no correlation between the patient’s symptoms and the cardiovascular symptoms; however, it was recommended that radiofrequency ablation be performed for atrial flutter. After consultation, hematologists believed that the patient’s routine blood tests indicated that the counts and percentages of leukocytes, erythrocytes, platelets were normal, the tumor index was only 4.56 ng/mL of prostate-specific antigen, and blood coagulation function was completely normal. The patient’s liver function, kidney function, and blood calcium level were all normal, but due to the loss of test results in other hospital, we did not obtain the patient’s free light chains, serum protein electrophoresis, and immunofixation electrophoresis results. The patient provided only pathological results of bone marrow biopsy, which indicated a significant decrease in hematopoietic tissue proliferation. A routine urine test indicated that the urine protein was negative, and there was no special treatment at that time. Therefore, regular follow-up was required. Based on the clinical manifestations, physical examination, various imaging findings, and examination reports of the disease, the patient was given a diagnosis of PHN, with the main site of nerve damage being the 3rd and 11th thoracic (T3 and T11) spinal nerves.
TREATMENT STRATEGIES:
Before hospitalization, the patient was administered various drugs orally, such as pregabalin, gabapentin, amitriptyline, and oxycodone hydrochloride prolonged-release tablets, with poor efficacy. On admission, the patient took pregabalin (225 mg) twice daily, oxcarbazepine (0.3 g) twice daily, oxycodone (10 mg) once every 12 h, and mecobalamin (0.5 mg) 3 times daily, and the NRS score was 3–6 points. The patient stopped taking oxcarbazepine, and duloxetine (30 mg) capsules were added twice daily. Then, under the guidance of digital subtraction angiography, left T3 and right T11 nerve pulse radiofrequency surgery was completed (Beijing Beiqi D13333; radio frequency parameters: the temperature, time, pulse width and frequency were set at 42°C, 240 s, 20 ms, and 2 Hz, respectively [Figure 3A, 3B]). Three cycles were administered in auto-standard mode. From the day of surgery to 1 week after surgery, the number of episodes of pain per day reduced to 2–4, and the NRS score reduced to 3–4 points, and within the week, the patient gradually stopped taking oxycodone successfully. Therefore, a color Doppler ultrasound-guided paravertebral nerve block was performed on the left T3 and right T11 thoracic vertebrae (each thoracic segment was injected with 2.5 mL lidocaine 2%, 0.9% normal saline, and 3.5 mg dexamethasone, with a total volume of 5 mL). The patient was discharged after the NRS score decreased to 1–3 points in the following week. For the first 2 weeks after discharge, nerve block therapy was performed once a week, and the NRS stabilized at 1–3 points. The pregabalin and duloxetine doses were gradually reduced. After 4 weeks, only oral pregabalin capsules were administered, and the dose was reduced to 150 mg twice daily. The NRS was stable at 1–3 points. After 3 months, the pregabalin dose was further reduced to 75 mg twice daily. After 4 months, all drugs were successfully discontinued, with occasional intermittent needle-pricking pain, and the NRS score was 0–1 points.
Discussion
PHN is a common complication of herpes zoster caused by the reactivation of VZV that lays dorment in the dorsal root ganglia of the spinal cord, leading to neuroinflammation, pain sensitization, or nerve damage, ultimately leading to neuropathic pain. Tseng et al reported a herpes zoster incidence rate of 9.92 per 1000 person-years in an integrated healthcare system. The proportions of cutaneous, neurologic, and other complications were 6.40% (95% CI, 1.73%–11.07%), 0.77% (95% CI, 0.00%–2.36%), and 1.01% (95% CI, 0.00%–2.93%), respectively [6]. PHN is characterized by nerve damage involving a single or adjacent nerve segment; the simultaneous occurrence of PHN in multiple segments and different parts is rare and has not been reported to date. In clinical practice, there are many cases of generalized herpes zoster in multiple segments or locations in patients with multiple myeloma. Yaffee et al (1961), Orbaneja et al (1965), and Saidi et al (1973) reported that patients with multiple myeloma developed systemic or multiple herpes zoster, but none of them developed severe neuropathic complications [7–9]. Cao et al reported a case of cervical refractory PHN in a patient with multiple myeloma who received lenalidomide maintenance therapy [10]. In the present case, a patient with multiple myeloma developed rare left T3 and right T11 segment herpes zoster simultaneously, and both developed PHN complications. The mechanism behind this phenomenon is currently unclear, but we believe that it may be related to the following 2 points: (1) the site of VZV infection belongs to the spinal cord region, with similar anatomical functions and morphology; and (2) VZV spreads to other spinal cord segments through the cerebrospinal fluid, which is similar to VZV causing multiple cranial neurites. This was elucidated in a study on VZV causing multiple cranial neuritis [11–13]. However, it is currently unknown how the virus can cause infection across multiple segments, and there can be other causes; therefore, the pathogenesis requires further in-depth research.
PHN in patients with herpes zoster is more common in older, immunosuppressed, or immunodeficient populations. Age, sex, prodromal pain, surgery, trauma, malignant tumor, infection, tuberculosis, chronic respiratory diseases, diabetes, and immune dysfunction are all risk factors for herpes zoster [6,14–17]. The exact mechanism of herpes zoster neuralgia has not been fully elucidated and is mainly related to peripheral sensitization, central sensitization, inflammatory response, nerve deafferents, and sympathetic nerve dysfunction [18]. Patients with PHN can also have multiple myeloma, and those with hematological tumors often have impaired immune system functioning. During the treatment process, chemotherapeutic drugs downregulate immune function, thus activating VZV and causing PHN. Di Meo et al reported bilateral herpes zoster in a patient with multiple myeloma who underwent bortezomib therapy [19]. Cao et al reported refractory PHN in a patient with multiple myeloma who received lenalidomide maintenance therapy [10]. Neuralgia can be caused by the compression of tumor tissue or direct infiltration of nerve tissue, leading to nerve damage. Chemotherapy-induced peripheral neuropathy is common. However, peripheral neuropathy induced by bortezomib, thalidomide, and other chemotherapeutic drugs can be related to both genetic factors and dose-dependent neurotoxicity [20–23].
The treatment principles for PHN are as follows: early, sufficient, full, and combined treatment. Drug treatment is the cornerstone of the whole process of PHN treatment. First-line drugs for PHN include calcium channel regulators (pregabalin and gabapentin), tricyclic antidepressants (amitriptyline), and 5% lidocaine patches. The second-line drugs include opioids and tramadol [18]. In this case, the therapeutic effect of pregabalin combined with tricyclic antidepressants, opioids, and other drugs was still unsatisfactory; therefore, we combined a variety of minimally invasive treatment technologies. Minimally invasive treatments for PHN include nerve block therapy, nerve pulse radio-frequency regulation, spinal cord electrical stimulation, neurolytic therapy, and intrathecal drug infusion therapy [24]. Although the parameters for the treatment of PHN are yet to be standardized, and the mechanism of radio frequency has not yet been fully clarified, radio frequency modulation technology currently has good therapeutic effects in the treatment of refractory peripheral neuropathy [25,26]. Pulsed radio frequency can affect the ATP metabolism of sensory nerves and the function of ion channels, continuously and reversibly inhibiting the excitatory afferents of C fibers, thus blocking pain conduction in related nerves [24,25]. In this case, we performed left T3 and right T11 radiofrequency surgery, followed by postoperative nerve block therapy. This treatment regimen significantly reduced the pain scores and oral medication dosages and achieved satisfactory results. Clinical studies using botulinum toxin injections have achieved good results, and autologous fat transplantation has been reported effective for the treatment of PHN. Herpes zoster vaccination is one of the most effective methods for preventing herpes zoster and reducing the incidence of PHN [27–29]. Low-dose antiviral drugs can prevent herpes zoster infection in patients with multiple myeloma treated with autologous stem cell transplantation [30]. In summary, the treatment of refractory PHN should adopt a multimodal plan that combines medication and multiple treatment modalities.
There are some limitations to this case. First, whether the different stages of multiple myeloma affect the pain level of herpes zoster neuralgia requires further researches to verify. Second, CT guidance can also be used instead of digital subtraction angiography guidance for nerve pulse radiofrequency therapy in this case. Although digital subtraction angiography guidance has the advantage of a lower radiation dose and can better avoid patient exposure to radiation, many studies have confirmed that CT guidance can more accurately locate the dorsal root ganglion [31,32].
Conclusions
This is a very rare case of PHN in clinical practice, with nerve damage affecting the left and right sides and 2 adjacent segments. PHN often occurs in elderly patients and in those with multiple chronic diseases, immune dysfunction, and tumors. The development of PHN in our patient may have been related to the presence of multiple myeloma. Once diagnosed, the most effective treatment is to initiate the use of medication as early as possible, combined with multimodal treatment methods, such as nerve pulse radio frequency and nerve block. With the development of minimally invasive interventional therapy, there is increasing evidence indicating that spinal cord electrical stimulation is also a good choice for refractory PHN cases. Minimally invasive interventional therapy, such as nerve pulse radiofrequency, nerve block, and spinal cord electrical stimulation, should be more widely promoted.
Figures
 Figure 1. (A) The patient’s frontal view shows significant skin pigmentation (black arrow) in the left chest (T3 segment) and right abdomen (T11 segment). (B) The patient also had pigmentation on the skin of the same nerve segment on the back. The pain also came from the skin pigmentation areas shown in figures a and b above.
Figure 1. (A) The patient’s frontal view shows significant skin pigmentation (black arrow) in the left chest (T3 segment) and right abdomen (T11 segment). (B) The patient also had pigmentation on the skin of the same nerve segment on the back. The pain also came from the skin pigmentation areas shown in figures a and b above. 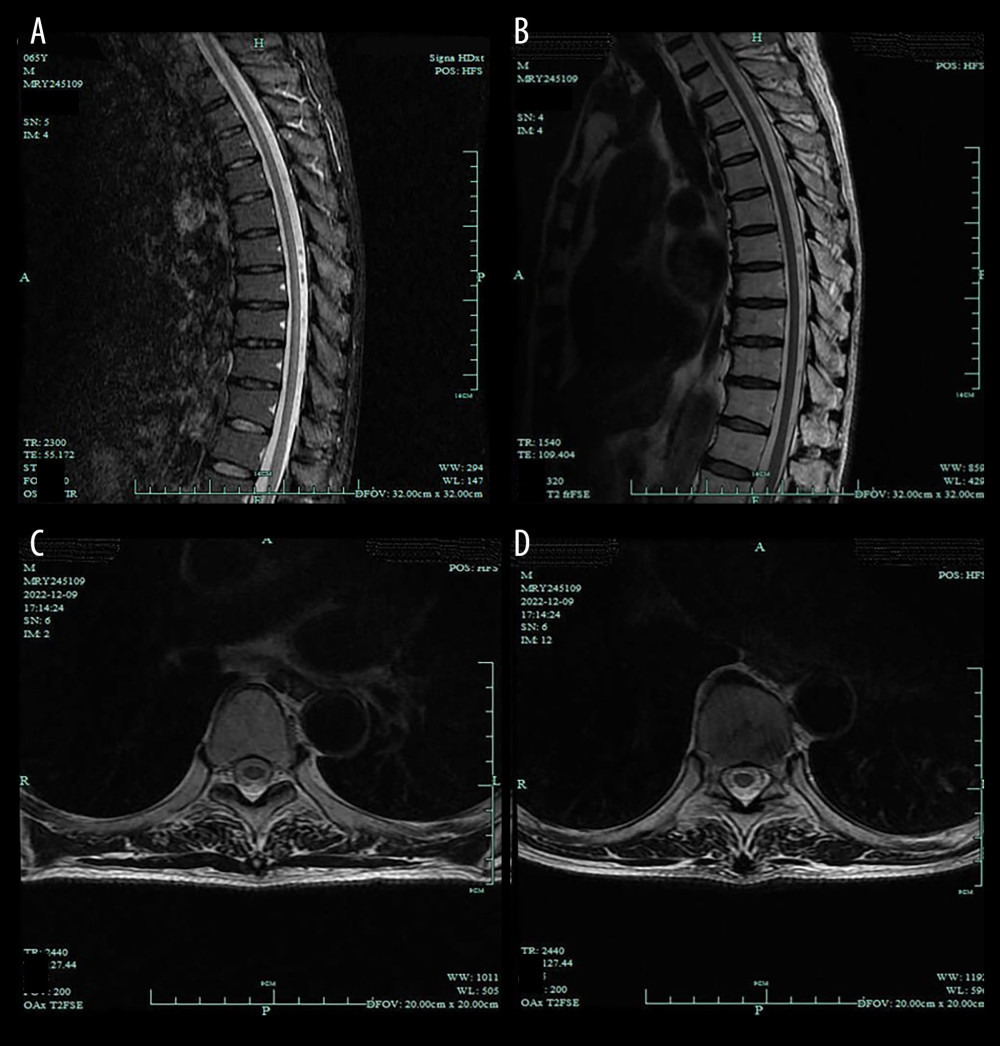 Figure 2. (A–D) The patient’s thoracic MRI showed no intraspinal- or extraspinal-related lesions, intervertebral disc herniation, spinal cord lesions, intraspinal tumors, or vertebral fractures.
Figure 2. (A–D) The patient’s thoracic MRI showed no intraspinal- or extraspinal-related lesions, intervertebral disc herniation, spinal cord lesions, intraspinal tumors, or vertebral fractures. 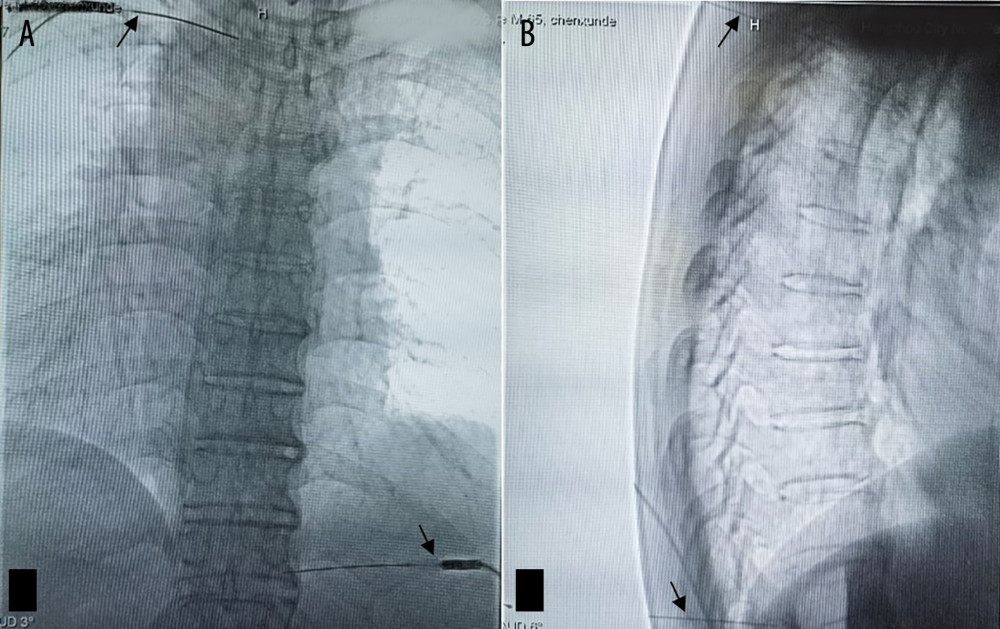 Figure 3. (A) In the prone position, digital subtraction angiography (DSA)-guided T3 and T11 nerve pulse radiofrequency anteroposterior films were taken, with the tip of the radiofrequency puncture needle (black arrow) located below the external pedicle of the vertebral arch. (B) DSA-guided T3 and T11 nerve pulse radiofrequency lateral films are shown, with the tip of the radiofrequency puncture needle located in the upper middle of the intervertebral foramen.
Figure 3. (A) In the prone position, digital subtraction angiography (DSA)-guided T3 and T11 nerve pulse radiofrequency anteroposterior films were taken, with the tip of the radiofrequency puncture needle (black arrow) located below the external pedicle of the vertebral arch. (B) DSA-guided T3 and T11 nerve pulse radiofrequency lateral films are shown, with the tip of the radiofrequency puncture needle located in the upper middle of the intervertebral foramen. References
1. Johnson RW, Rice AS, Clinical practice. Postherpetic neuralgia: N Engl J Med, 2014; 371(16); 1526-33
2. Gross GE, Eisert L, Doerr HW, S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia: J Dtsch Dermatol Ges, 2020; 18(1); 55-78
3. Hempenstall K, Nurmikko TJ, Johnson RW, Analgesic therapy in postherpetic neuralgia: A quantitative systematic review: PLoS Med, 2005; 2(7); e164
4. Liu Q, Wu X, Guo J, Analgesic effect of electroacupuncture on postherpetic neuralgia: A trial protocol for a multicenter randomized controlled trial: Pain Ther, 2021; 10(2); 1755-71
5. Bian Z, Yu J, Tu M, Acupuncture therapies for postherpetic neuralgia: A protocol for a systematic review and Bayesian network meta-analysis: BMJ Open, 2022; 12(3); e056632
6. Tseng HF, Bruxvoort K, Ackerson B, The epidemiology of herpes zoster in immunocompetent, unvaccinated adults ≥50 years old: Incidence, complications, hospitalization, mortality, and recurrence: J Infect Dis, 2020; 222(5); 798-806
7. Yaffee HS, Greenberg MS, Herpes zoster resembling acute varicella associated with multiple myeloma: JAMA, 1961; 175; 1008-10
8. Orbaneja Gomez J, Ledo Pozueta A, Lozano de Sosa SGeneralized herpes zoster in a patient with multiple myeloma: Actas Dermosifiliogr, 1965; 56(1); 3-8
9. Saidi P, Uhlman WE, Goldberg I, Herpes zoster and multiple myeloma: J Med Soc N J, 1973; 70(11); 836-38
10. Cao X, Wu G, Jiao B, Zhang X, Refractory postherpetic neuralgia in a multiple myeloma patient with lenalidomide maintenance therapy: A case report: J Int Med Res, 2022; 50(9); 3000605221123882
11. Schnall JA, Khan SF, Zolio L, Polyneuritis cranialis from varicella zoster virus reactivation: Med J Aust, 2020; 213(8); 352-353e1
12. Kim YH, Choi IJ, Kim HM, Bilateral simultaneous facial nerve palsy: Clinical analysis in seven cases: Otol Neurotol, 2008; 29(3); 397-400
13. Syal R, Tyagi I, Goyal A, Bilateral Ramsay Hunt syndrome in a diabetic patient: BMC Ear Nose Throat Disord, 2004; 4(1); 3
14. Kim M, Han K, Yoo SA, Lee JH, Herpes zoster and subsequent cancer risk: A nationwide population-based cohort study in Korea: Dermatology, 2021; 237(1); 73-78
15. König C, Kleber M, Reinhardt H, Incidence, risk factors, and implemented prophylaxis of varicella zoster virus infection, including complicated varicella zoster virus and herpes simplex virus infections, in lenalidomide-treated multiple myeloma patients: Ann Hematol, 2014; 93(3); 479-84
16. John AR, Canaday DH, Herpes zoster in the older adult: Infect Dis Clin North Am, 2017; 31(4); 811-26
17. Marra F, Parhar K, Huang B, Vadlamudi N, Risk factors for herpes zoster infection: A meta-analysis: Open Forum Infect Dis, 2020; 7(1); ofaa005
18. Werner RN, Nikkels AF, Marinović B, European consensus-based (S2k) Guideline on the Management of Herpes Zoster – guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 2: Treatment: J Eur Acad Dermatol Venereol, 2017; 31(1); 20-29
19. di Meo N, Bergamo S, Dondas A, Trevisan G, Bortezomib and bilateral herpes zoster: Acta Dermatovenerol Alp Pannonica Adriat, 2012; 21(1); 21-22
20. Argyriou AA, Iconomou G, Kalofonos HP, Bortezomib-induced peripheral neuropathy in multiple myeloma: A comprehensive review of the literature: Blood, 2008; 112(5); 1593-99 [Erratum in: Blood. 2009;113(18):4478]
21. Campo C, da Silva Filho MI, Weinhold N, Bortezomib-induced peripheral neuropathy: A genome-wide association study on multiple myeloma patients: Hematol Oncol, 2018; 36(1); 232-37
22. Goel L, Gupta P, Pahuja M, Mechanistic involvement of inflammation in bortezomib-induced peripheral neuropathy: Comb Chem High Throughput Screen, 2022; 25(10); 1595-600
23. Zhao W, Wang W, Li X, Peripheral neuropathy following bortezomib therapy in multiple myeloma patients: Association with cumulative dose, heparanase, and TNF-α: Ann Hematol, 2019; 98(12); 2793-803
24. Lin CS, Lin YC, Lao HC, Chen CC, Interventional treatments for postherpetic neuralgia: a systematic review: Pain Physician, 2019; 22(3); 209-28
25. Chang MC, Efficacy of pulsed radiofrequency stimulation in patients with peripheral neuropathic pain: A narrative review: Pain Physician, 2018; 21(3); E225-E34
26. Vuka I, Marciuš T, Došenović S, Efficacy and safety of pulsed radiofrequency as a method of dorsal root ganglia stimulation in patients with neuropathic pain: A systematic review: Pain Med, 2020; 21(12); 3320-43
27. Lal H, Cunningham AL, Godeaux OZOE-50 Study Group, Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults: N Engl J Med, 2015; 372(22); 2087-96
28. Cunningham AL, Lal H, Kovac MZOE-70 Study Group, Efficacy of the Herpes zoster subunit vaccine in adults 70 years of age or older: N Engl J Med, 2016; 375(11); 1019-32
29. Tricco AC, Zarin W, Cardoso R, Efficacy, effectiveness, and safety of herpes zoster vaccines in adults aged 50 and older: Systematic review and network meta-analysis: BMJ, 2018; 363; k4029
30. Minarik J, Pika T, Bacovsky J, Low-dose acyclovir prophylaxis for bortezomib-induced herpes zoster in multiple myeloma patients: Br J Haematol, 2012; 159(1); 111-13
31. Ding Y, Li H, Hong T, Efficacy and safety of computed tomography-guided pulsed radiofrequency modulation of thoracic dorsal root ganglion on herpes zoster neuralgia: Neuromodulation, 2019; 22(1); 108-14
32. Chazen JL, Roytman M, Yoon ES, CT-guided C2 dorsal root ganglion radiofrequency ablation for the treatment of cervicogenic headache: Case series and clinical outcomes: Am J Neuroradiol, 2022; 43(4); 575-78
Figures
Figure 1. (A) The patient’s frontal view shows significant skin pigmentation (black arrow) in the left chest (T3 segment) and right abdomen (T11 segment). (B) The patient also had pigmentation on the skin of the same nerve segment on the back. The pain also came from the skin pigmentation areas shown in figures a and b above.Figure 2. (A–D) The patient’s thoracic MRI showed no intraspinal- or extraspinal-related lesions, intervertebral disc herniation, spinal cord lesions, intraspinal tumors, or vertebral fractures.Figure 3. (A) In the prone position, digital subtraction angiography (DSA)-guided T3 and T11 nerve pulse radiofrequency anteroposterior films were taken, with the tip of the radiofrequency puncture needle (black arrow) located below the external pedicle of the vertebral arch. (B) DSA-guided T3 and T11 nerve pulse radiofrequency lateral films are shown, with the tip of the radiofrequency puncture needle located in the upper middle of the intervertebral foramen. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.949976
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950290
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950607
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950985
Most Viewed Current Articles
07 Dec 2021 : Case report  17,691,734
17,691,734
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  164,491
164,491
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
113,090
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
59,175
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133