27 May 2025: Articles 
Diagnosis and Management of Autoimmune Hepatitis After Hepatitis A in a Young Woman
Challenging differential diagnosis, Unusual setting of medical care, Rare disease
Siddharth PatelDOI: 10.12659/AJCR.946795
Am J Case Rep 2025; 26:e946795






Abstract
BACKGROUND: Hepatitis A (Hep A) is a common cause of viral hepatitis in developing nations. Autoimmune hepatitis is characterized by subacute to chronic liver inflammation, which can lead to liver cirrhosis if untreated. Both conditions remain uncommon in the United States. Development of autoimmune hepatitis following viral Hep A is extremely rare. However, viral infections, including Hep A, have been implicated in triggering autoimmune diseases through immune system activation, molecular mimicry, and inflammatory cytokine surges. Early recognition of this phenomenon is crucial for timely intervention and improved outcomes.
CASE REPORT: A 32-year-old Hispanic woman with a history of Hep A presented to the emergency room with chief concerns of intermittent epigastric abdominal pain and jaundice for 2 weeks. Physical exam revealed scleral icterus with right upper-quadrant tenderness. Although abdominal imaging was concerning for gallbladder wall thickening, the degree of hyperbilirubinemia (10 mg/dL) and ALT (2100 U/L) elevation were out of proportion to that commonly seen with cholecystitis. The patient’s condition deteriorated despite supportive treatment. Further investigations detected IgG against Hep A, positive anti-nuclear antibodies, and anti-smooth muscle antibodies. The liver biopsy confirmed autoimmune hepatitis. The patient showed rapid clinical improvement after initiation of intravenous steroids and was ultimately discharged home.
CONCLUSIONS: Autoimmune hepatitis developing after acute Hep A is rare. High clinical suspicion and prompt treatment with systemic steroids are key for rapid clinical improvement and preventing complications. Recognizing viral infections as potential autoimmune triggers may help guide earlier diagnosis and intervention.
Keywords: hepatitis A, Hepatitis, Autoimmune, Jaundice, Hepatitis, Viral, Human, Liver failure, Humans, Female, adult
Introduction
Hepatitis A (Hep A) is a self-limited, infectious liver disease that is transmitted via the fecal-oral route. In developing countries, Hep A is commonly transmitted through consumption of contaminated water [1]. However, in the U.S. and other developed countries, it is classically seen in immigrants or in patients who have consumed contaminated food [2]. According to the Centers for Disease Control (CDC), approximately 4500 new Hep A cases were reported in the U.S. in 2022 [3].
Autoimmune Hepatitis (AIH) is a chronic inflammatory liver disease caused by immune-mediated hepatocyte inflammation. The clinical presentation of AIH varies depending on the stage at which patients are diagnosed. The prevalence of AIH in the U.S. is estimated to be 31.4 per 100 000 persons [4], which is more than the worldwide pooled prevalence of 15.65 per 100 000 persons [5]. Although AIH is rare, it has serious ramifications, as untreated AIH can progress to cirrhosis, hepatic failure, and hepatocellular carcinoma.
The literature suggests that acute viral infections, such as Hep A, can act as triggers for the development of AIH, although there is no definitive evidence to establish a cause-and-effect relationship [6]. The proposed mechanism involves activation of the immune system during the acute viral infection, leading to autoreactivity and inflammation, culminating in AIH. We present a rare case of AIH triggered by a recent Hep A infection in a 32-year-old Hispanic woman.
Case Report
A 32-year-old Hispanic woman with a history of Hep A and gastroesophageal reflux disease (GERD) presented to the emergency room (ER) with chief concerns of intermittent epigastric abdominal pain of 2 weeks’ duration. The pain was burning or fullness-like, 5/10 in intensity, occasionally radiating to the right upper quadrant, and associated with nausea and dry heaves without vomiting. It was not related to the type or timing of food intake. She also noted jaundice of the skin and sclera and dark urination associated with it. She denied fever, weight loss, recent travel, sick contacts, stool frequency alteration, or blood in the stool. She did not have burning micturition, hematuria, or flank pain. She had a recent diagnosis of Hep A about 3 months ago, which manifested as jaundice and nausea. It was managed symptomatically, and she recovered within 1 month of diagnosis. She denied any prior surgery or the use of tobacco, alcohol, or recreational substances. She denied any history of autoimmune disease, and no-one in her family has a history of similar illness or liver disease. She reported the use of daily pantoprazole but denied current/prior use of medications linked to drug-induced AIH, such as nitrofurantoin and statins [7]. She denied other medication use or allergies. Physical examination in the ER detected a blood pressure of 138/75, heart rate of 86, respiratory rate of 20, O2 saturation at 99%, temperature of 37°C, and BMI of 27.1 kg/m2. She had marked jaundice affecting the sclera and skin, and her abdomen was soft and non-distended, with no hepatosplenomegaly. She had mild tenderness in the right upper quadrant, without guarding or rigidity, and equivocal Murphy’s sign. Cardiovascular, respiratory, and musculoskeletal exams were unremarkable. She was awake, alert, oriented, and had no tremors.
Complete blood count, comprehensive metabolic panel, coagulation studies, and urinalysis were performed (Table 1). The results were remarkable for transaminitis and hyperbilirubinemia – both direct and indirect. A computed tomography (CT) scan and ultrasound of the abdomen/pelvis demonstrated a normal appearance of the liver but showed mucosal gallbladder thickening without cholelithiasis (Figure 1A). Magnetic resonance cholangiopancreatography (MRCP) did not detect any evidence of biliary obstruction. Despite supportive treatment with intravenous (IV) fluids, antiemetics, and prophylactic antibiotics, liver function tests (LFTs) showed deterioration. Considering the severity of abnormal LFTs and relatively benign abdominal exam, cholecystitis was less likely. Serology ruled out acute viral hepatitis but confirmed prior Hep A with positive IgG. A chronic liver disease work-up returned positive for anti-nuclear antibody (ANA) and anti-smooth muscle antibody (anti-SMA). A Revised Original Score for Autoimmune Hepatitis was performed. This patient’s score was calculated to be 14, which is significant for probable AIH. Our suspicion of autoimmune hepatitis was ultimately confirmed with a CT-guided liver biopsy and histopathology, which showed extensive lymphoplasmacytic infiltrate with mild portal fibrosis without cirrhosis (Figure 1B). The patient was started on IV steroids (40 mg methylprednisolone) on Day 7, to which she showed a marked response. LFTs trended down, and she improved symptomatically (Figure 2). The timing of her presentation indicated post-viral autoimmune hepatitis. She was discharged after 13 days of hospitalization on 40 mg oral prednisone daily with a weekly taper of 5 mg, and close follow-up was advised.
Discussion
Hep A, a Picornaviridae family virus, is primarily transmitted via the fecal-oral route and causes self-limiting acute hepatitis worldwide [1]. In developing countries, Hep A is commonly seen in areas with inadequate sewage systems [2]. Conversely, in the U.S., Hep A outbreaks tend to occur in high-risk populations, such as those who have consumed contaminated food or recently traveled to regions where Hep A is endemic [2]. The World Health Organization (WHO) estimates more than 100 million people worldwide contract Hepatitis A each year, leading to 15 000–30 000 deaths annually [8]. In the U.S., the CDC reported 4500 new Hep A infections in 2022 [3]. While this represented a 59% decrease compared to 2021, it was still 1.6 times higher than in 2015 [3]. Hep A outbreaks have been a public health concern over the last decade, with cases occurring across 37 states, 61% of them needing hospitalization and resulting in 424 deaths [9]. The clinical presentation of Hep A can range from asymptomatic infection to fulminant liver failure, although chronic liver disease is quite rare [10]. Typical symptoms of acute Hep A include fatigue, abdominal pain, malaise, nausea, vomiting, and fever. Treatment primarily focuses on supportive care, as most infections resolve spontaneously. In rare instances, Hep A can cause prolonged or relapsing illness, with a few cases advancing to fulminant liver failure [11].
AIH is a chronic disease characterized by hepatocyte inflammation due to circulating autoantibodies. Women are more likely to be affected by AIH, with a prevalence of 80% of patients in the United States [4] and 75% of patients worldwide identifying as female [12]. Early epidemiological studies presented a bimodal age distribution, with age ranges 10–30 and 40–60 being affected the most. However, recent international and national studies have found the prevalence to be higher in patients aged >65 [4,12,13]. AIH also has differences in prevalence among ethnic groups. Bitterman et al reported prevalence to be 40.5/100 000 in African Americans, 34.9/100 000 in Hispanics, and 33.1/100 000 in Whites (95% CI,
AIH can be subclassified into autoimmune hepatitis type 1 (AIH-1) and type 2 (AIH-2). AIH 1 is usually positive for anti-smooth muscle, whereas type 2 is positive for anti-liver/kidney microsomal antibody type 1 (anti-LKM1) or anti-LKM type 3. Autoimmune hepatitis type 1 is significantly more frequent than type 2, with AIH-1 accounting for about 80–90% of AIH cases, while AIH-2 is less common and more often seen in children [13]. Clinical assessment of AIH requires testing of autoimmune serologic markers such as ANA, anti-SMA, anti-LKM1, and anti-LKM type 3 [14,15]. Liver biopsy also confirms diagnosis and guides treatment [12]. Common histopathological findings in patients with AIH include interface hepatitis, inflammatory infiltration with plasma and lymphocyte cell predominance, and rosettes [15]. Our patient’s diagnostic markers were like those described in the literature, with findings of positive ANA and anti-SMA and a biopsy that showed extensive lymphoplasmacytic infiltrate.
AIH has been historically linked to viral pathologies causing chronic liver damage such as Hepatitis B, C, D, and Herpesviridae [16]. Although not fully understood, the pathologic process is believed to be induced by molecular mimicry [15]. Cytochrome P450 IID6 has been identified as the autoantigen most closely associated with autoimmune hepatitis. Several pathogens have been shown to have epitopes like these self-antigens. Sometimes, vaccine-induced peptides and gut-derived antigens also mimic the tissue antigens. Studies also suggest that chaperone molecules can potentiate the pathogenicity of molecular mimics [17]. Defective suppressor-inducer T lymphocyte response to asialoglycoprotein receptor expressed on the hepatocyte surface is also proposed as a potential mechanism of AIH following Hep A [18].
Through mechanisms like molecular mimicry and cytokine surges, the infection can unmask or accelerate conditions such as autoimmune hepatitis, lupus, or thyroid disorders. Inflammatory cytokines like TNF-α and IL-6 contribute to immune dysregulation, potentially worsening underlying autoimmunity. Due to the self-limiting nature of Hepatitis A infections, its association with AIH is rare, although some cases have been reported. We performed a thorough literature search to investigate this association further.
Subramanian et al, Jo et al, and S-Are et al have published cases of AIH following acute viral Hep A. The majority of patients presenting with AIH after Hep A were women and had jaundice, elevated liver enzymes, and icteric sclerae [16,19]. All the patients had a serologic diagnosis of Hep A through positive anti-Hep A immunoglobulin M (IgM) before testing positive for AIH markers such as anti-smooth muscle antibodies. These findings are like those found in our patient. However, the timeline between the episode of Hep A infection and diagnosis of AIH differed between case reports. In the case described by Jo et al, the patient experienced a rebound increase in LFTs as early as 20 days after the diagnosis of Hep A, as compared to nearly 3 months in our case. Unlike our patient, all the case reports found a positive anti-Hep A IgM at the time of diagnosis with AIH as compared to IgG. Like our case, treatment regimens in Subramanian et al and Jo et al included the use of prednisolone with the addition of azathioprine.
Steroids, usually prednisone, form the mainstay in the first-line treatment of AIH to suppress liver inflammation. Azathioprine is commonly added to minimize overall steroid dosage. Patients typically improve clinically and biochemically within weeks to months. Treatment usually continues for at least 1–2 years to maintain remission, after which long-term follow-up is required to adjust medications and prevent relapse.
Conclusions
Although AIH after an episode of acute Hep A infection is an extremely rare occurrence, clinicians should be aware of the possibility. The treatment of AIH following hepatitis A infection centers around prompt initiation of immunosuppression with corticosteroids and azathioprine. In the present case, prednisone treatment led to rapid clinical improvement. Regular follow-up with frequent liver function tests and clinical assessments is important to prevent progression of liver disease and its associated complications.
Figures
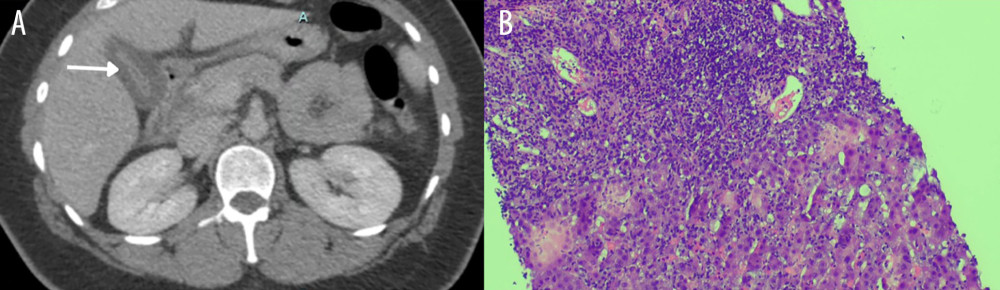 Figure 1. (A) Abdominal CT scan. The image shows marked mucosal thickening of the gallbladder and is indicated by the white arrow. (B) Histopathology of the liver showing autoimmune hepatitis. The sample is a core-needle biopsy of the right liver lobe. Hepatic architecture shows centrilobular-portal bridging necrosis and pronounced portal and lobular mixed inflammation with prominent plasma cells. The parenchyma shows marked lobular disarray with regeneration.
Figure 1. (A) Abdominal CT scan. The image shows marked mucosal thickening of the gallbladder and is indicated by the white arrow. (B) Histopathology of the liver showing autoimmune hepatitis. The sample is a core-needle biopsy of the right liver lobe. Hepatic architecture shows centrilobular-portal bridging necrosis and pronounced portal and lobular mixed inflammation with prominent plasma cells. The parenchyma shows marked lobular disarray with regeneration. 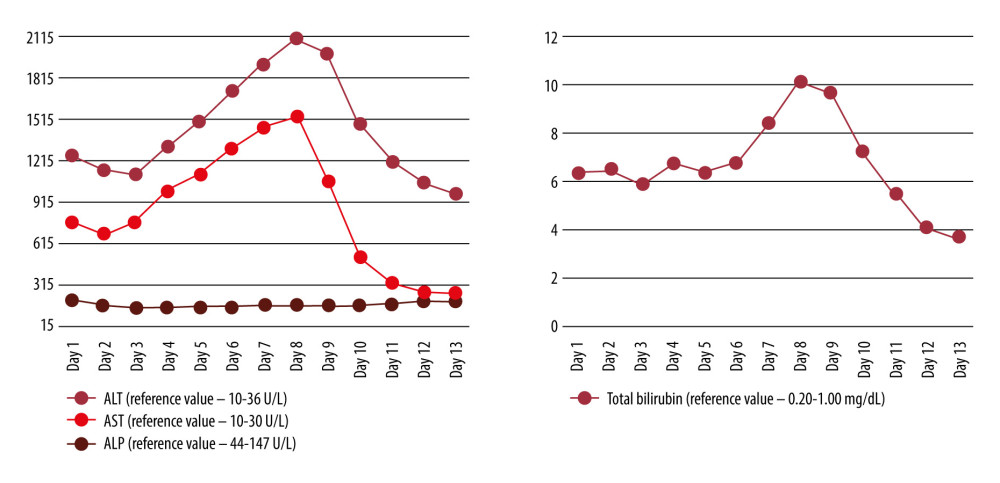 Figure 2. Trend of liver function tests during hospital stay. Aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and bilirubin levels were followed throughout the length of stay.
Figure 2. Trend of liver function tests during hospital stay. Aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and bilirubin levels were followed throughout the length of stay. 
References
1. Shin EC, Jeong SH, Natural history, clinical manifestations, and pathogenesis of Hepatitis A: Cold Spring Harb Perspect Med, 2018; 8(9); a031708
2. Tjon GMS, Coutinho RA, van den Hoek A, High and persistent excretion of hepatitis A virus in immunocompetent patients: J Med Virol, 2006; 78(11); 1398-405
3. , 2022 Hepatitis A: Viral Hepatitis Surveillance Report April 1, 2024, CDC https://www.cdc.gov/hepatitis/statistics/2022surveillance/hepatitis-a.htm
4. Tunio NA, Mansoor E, Sheriff MZ, Epidemiology of Autoimmune Hepatitis (AIH) in the United States between 2014 and 2019: A population-based national study: J Clin Gastroenterol, 2021; 55(10); 903
5. Hahn JW, Yang HR, Moon JS, Global incidence and prevalence of autoimmune hepatitis, 1970–2022: A systematic review and meta-analysis: eClinicalMedicine, 2023; 65; 102280
6. Jo HI, Kim M, Yoo JJ, Acute Hepatitis A – induced autoimmune hepatitis: A case report and literature review: Medicina (Mex), 2022; 58(7); 845
7. , LiverTox: Clinical and research information on drug-induced liver injury [Internet]: Autoimmune Hepatitis. [Updated 2019 May 4], 2012, Bethesda (MD), National Institute of Diabetes and Digestive and Kidney Diseases Available from: https://www.ncbi.nlm.nih.gov/books/NBK548188/
8. Organization WH: WHO Immunological basis for immunization series: Module 18: Hepatitis A, 2019, World Health Organization https://iris.who.int/handle/10665/326501
9. CDC, Hepatitis A outbreak linked to person-to-person contact: Viral Hepatitis May 24, 2024 https://www.cdc.gov/hepatitis/outbreaks/ongoing-hepatitis-a/index.html
10. Kemmer NM, Miskovsky EP, Hepatitis A: Infect Dis Clin North Am, 2000; 14(3); 605-15
11. Koff RS, Clinical manifestations and diagnosis of hepatitis A virus infection: Vaccine, 1992; 10(Suppl 1); S15-17
12. Shiffman ML, Autoimmune hepatitis: Epidemiology, subtypes, and presentation: Clin Liver Dis, 2024; 28(1); 1-14
13. Linzay CD, Sharma B, Pandit S, Autoimmune hepatitis. [Updated 2023 Aug 14]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK459186/
14. Bittermann T, Lewis JD, Levy C, Goldberg DS, Sociodemographic and geographic differences in the US epidemiology of autoimmune hepatitis with and without cirrhosis: Hepatology, 2023; 77(2); 367
15. Yadav V, Irfan R, Safdar S, Advances in understanding and managing autoimmune hepatitis: A narrative review: Cureus, 2023; 15; e43973
16. S-Are V, Yoder L, Samala N, An outbreak presents an opportunity to learn about a rare phenotype: Autoimmune hepatitis after acute Hepatitis A: Ann Hepatol, 2020; 19(6); 694-96
17. Czaja AJ, Incorporating the molecular mimicry of environmental antigens into the causality of autoimmune hepatitis: Dig Dis Sci, 2023; 68(7); 2824-42
18. Vento S, Garofano T, Di Perri G, Identification of Hepatitis A virus as a trigger for autoimmune chronic hepatitis type 1 in susceptible individuals: Lancet, 1991; 337(8751); 1183-87
19. Subramanian SK, Patel JM, Younes M, Nevah Rubin MI, Postinfectious autoimmune hepatitis-induced liver failure: A consequence of Hepatitis A virus infection: ACG Case Rep J, 2020; 7(8); e00441
Figures
Figure 1. (A) Abdominal CT scan. The image shows marked mucosal thickening of the gallbladder and is indicated by the white arrow. (B) Histopathology of the liver showing autoimmune hepatitis. The sample is a core-needle biopsy of the right liver lobe. Hepatic architecture shows centrilobular-portal bridging necrosis and pronounced portal and lobular mixed inflammation with prominent plasma cells. The parenchyma shows marked lobular disarray with regeneration.Figure 2. Trend of liver function tests during hospital stay. Aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and bilirubin levels were followed throughout the length of stay. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133