25 May 2025: Articles 
A Rare Case of Severe Pernicious Anemia with Neuropsychiatric Implications
Challenging differential diagnosis, Unusual setting of medical care, Rare disease
Stanley KimDOI: 10.12659/AJCR.946911
Am J Case Rep 2025; 26:e946911






Abstract
BACKGROUND: Pernicious anemia (PA) is caused by a deficiency in intrinsic factor (IF), which is necessary for vitamin B12 (cobalamin) absorption, resulting in vitamin B12 deficiency and subsequent megaloblastic anemia. Diagnosis of PA relies on the detection of circulating antibodies to IF. In addition to anemia, patients can develop neuropsychiatric conditions, such as subacute combined degeneration of the spinal cord or psychosis. We present the case of a patient with a history of schizophrenia who exhibited unusually severe manifestations of pernicious anemia, including life-threatening anemia, multiple hypersegmented neutrophils, and significantly elevated methylmalonic acid (MMA) levels.
CASE REPORT: A 51-year-old Hispanic woman with a history of schizophrenia was admitted with severe weakness, shortness of breath, and diarrhea. The hemoglobin (Hb) level was 2.5 g/dL and mean corpuscular volume (MCV) was 133 fL. A diagnosis of pernicious anemia was made by a low vitamin B12 level, high levels of methylmalonic acid (MMA) and homocysteine, and positive IF-blocking antibodies. Her anemia did not improve initially, even after 3 units of blood were transfused. She had no signs of bleeding. It was thought that hemoconcentration due to severe dehydration falsely raised her initial Hb levels, which were corrected by hydration. A peripheral blood smear showed many hypersegmented neutrophils. With parenteral cyanocobalamin therapy, her anemia and schizophrenia symptoms improved. The hypersegmented neutrophils disappeared by 2 weeks.
CONCLUSIONS: This is an extreme case of pernicious anemia with life-threatening anemia. The hypersegmented neutrophils disappeared in 2 weeks with vitamin B12 therapy. The symptoms of schizophrenia also improved.
Keywords: Anemia, Pernicious, Vitamin B 12 Deficiency, Neutrophils, Humans, Female, Middle Aged, Vitamin B 12, Schizophrenia, Methylmalonic Acid
Introduction
Pernicious anemia (PA) is a form of autoimmune gastritis (AIG) resulting from destruction of gastric parietal cells, leading to a deficiency in intrinsic factor (IF), which is necessary for vitamin B12 (cobalamin) absorption by binding ingested vitamin B12. This deficiency results in vitamin B12 deficiency and subsequent megaloblastic anemia [1–4].
Vitamin B12 is necessary for the development and initial myelination of the central nervous system as well as for maintenance of its normal function. In addition to anemia-related symptoms, patients with vitamin B12 deficiency can develop neuropsychiatric conditions, such as subacute combined degeneration of the spinal cord or psychosis [1,2,4]. Less common conditions associated with vitamin B12 deficiency include glossitis, malabsorption, infertility, and thrombosis [2,3].
In the absence of the Schilling test, a definitive diagnosis of pernicious anemia (PA) relies on the detection of circulating antibodies to intrinsic factor (IF) and gastric parietal cells. Cobalamin of <200 ng/L plus the presence of anti-IF antibodies confirm a diagnosis of pernicious anemia [1].
Hypersegmented neutrophils are a characteristic feature of megaloblastic anemia caused by vitamin B12 or folate deficiency, or both [5]. However, neutrophil hypersegmentation does not appear to be a sensitive indicator of mild B12 deficiency. Leukopenia and thrombocytopenia may be present but only rarely cause clinical problems [6]. Although the classical presentation of B12 deficiency is hematological, it is important to note that neuropsychiatric manifestations can be the initial symptoms of a developing B12 deficiency syndrome [7]. Patients with confirmed PA require lifelong vitamin B12 treatment with intramuscular (IM) injections initially followed by high-dose oral supplementation [1–4].
We present the case of a patient with a history of schizophrenia who exhibited unusually severe manifestations of pernicious anemia, including life-threatening anemia, multiple hypersegmented neutrophils, and significantly elevated methylmalonic acid (MMA) levels. We also discuss the neuropsychiatric implications of PA.
Case Report
A 51-year-old woman with a history of schizophrenia was admitted with severe weakness, shortness of breath, and intermittent non-bloody diarrhea. She had been mostly bedridden for the past month. Her medical records showed refills for trazodone, risperidone, and duloxetine for several years. She was homeless, unemployed, and living in a motel. Detailed information about her schizophrenia was not available.
Her vital signs were: blood pressure 84/57 mmHg, pulse 90 beats per minute, temperature 36.4°C, respiratory rate 18 per minute, and oxygen saturation 95% on room air. On examination, she had pale conjunctivae, non-icteric sclera, dry skin and oral mucous membranes, and a scaphoid abdomen with no hepatosplenomegaly. She was drowsy but able to move her extremities. Deep tendon reflex (knee jerk) was absent. Her laboratory test results are summarized in Table 1. On the first day (Day 1) of hospitalization, notable results included hemoglobin (Hb) 2.5 g/dL, MCV 133.2, reticulocyte 2.7%, total bilirubin 2.7 mg/dL (direct bilirubin 0.5 mg/dL), LDH 2385 U/L, vitamin B12 level 72 pg/mL, positive intrinsic factor-blocking antibody, and negative anti-parietal cell antibody. The serum MMA was extremely high at 34 920 nmol/L (normal range: 73–475), and homocysteine was elevated at 198 μmol/L (normal range: 5–15).
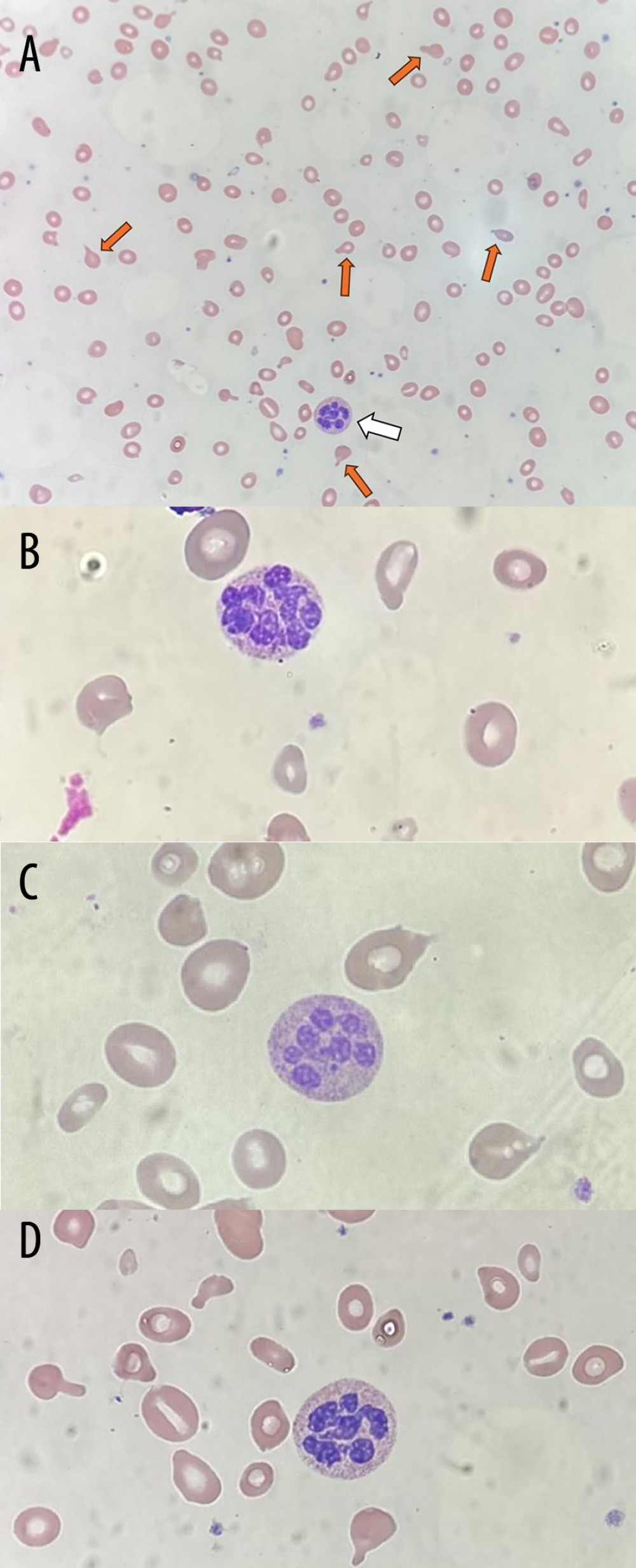
The peripheral blood smear on Day 1 (Figure 1A–1D) revealed frequent hypersegmented neutrophils with 6–8 lobes, as well as poikilocytosis, anisocytosis, hypochromia, and occasional teardrop cells. Hypersegmented neutrophils were seen in 5–10% of the cells.
The patient was treated with daily intramuscular (IM) injections of cyanocobalamin (1000 mcg) and she received packed red blood cell (PRBC) transfusions along with intravenous (IV) fluids. Despite receiving 3 units of PRBCs, her Hb levels did not initially improve. A stool occult blood test was negative, and she had no other clinical signs of bleeding. It was thought that hemoconcentration due to severe dehydration falsely raised her initial Hb levels, which were corrected by IV hydration.
After receiving 4 units of PRBCs, her Hb increased to 3.1 g/dL. Gradually, she regained strength and mental clarity. By Day 7, she was able to walk without any assistance. She said she had mild numbness in both lower extremities. After a total of 6 units of PRBCs and daily IM cobalamin injections, the Hb increased to 8.1 g/dL and reticulocytes to 20.7%. She was discharged on Day 9 with a prescription for oral vitamin B12 (1000 mcg daily). A peripheral blood smear on Day 9 still showed occasional hypersegmented neutrophils, but fewer than before (<5%), with a maximum of 6 nuclear lobes. After discharge, she was placed in a public residential facility and has been monitored by a social worker on a weekly basis.
On Day 15, the patient returned to the hematology clinic with the social worker for a follow-up. She appeared mentally clear and reported feeling well. She denied any symptoms such as paresthesia, ataxia, abdominal pain, nausea, or diarrhea. Her Hb was 9.2 g/dL, and the vitamin B12 level had risen to 988 pg/mL. The total bilirubin level decreased to 1.1 mg/dL. The peripheral smear no longer showed hypersegmented neutrophils.
Two months after discharge, she no longer had anemia. The Hb was 15.1 g/dL and MCV 94.1 fL. The MMA level also normalized at 240 nmol/L. To evaluate for AIG, she was referred to a gastroenterologist for endoscopy. According to her social worker who accompanied the patient, she no longer takes psychiatric medications and shows no signs of mental disorder.
Discussion
EXTREME ANEMIA WITH CRITICALLY LOW INITIAL HEMOGLOBIN LEVEL (PROBABLY LESS THAN 2.0 G/DL):
The patient’s initial Hb was 2.5 g/dL, and this did not increase initially despite transfusion of 3 units of PRBCs. Upon presentation, she was dehydrated due to poor oral intake and diarrhea, as evidenced by both physical (dry skin) and laboratory findings (BUN 41 mg/dL and creatinine 1.51 mg/dL on Day 1). Apparently, dehydration caused hemoconcentration resulting in falsely high Hb levels initially. With IV hydration, her dehydration and hemoconcentration were corrected, lowering the Hb levels. By Day 5, the BUN had decreased to 16 mg/dL and creatinine to 0.93 mg/dL. Thus, her true initial hemoglobin level must have been lower than 2.5 g/dL, likely less than 2 g/dL. Postoperatively, extreme anemia (Hb <2 g/dL) is often fatal [10,11], although there is a reported case of a patient with megaloblastic anemia due to vitamin B12 deficiency who survived with a Hb level of 1.7 g/dL [10]. It is extremely unusual for a patient to develop critical anemia with Hb 2.5 (actual Hb: probably <2.0 g/dL) and survive.
EXTREME HYPERSEGMENTED NEUTROPHILS WITH 8-10 NUCLEAR LOBES:
Hypersegmented neutrophils are seen in 98.3% of patients with megaloblastic anemia [2]. The neutrophils in our patient displayed an unusually high number of nuclear lobes. One of the neutrophils (Figure 1A) had at least 8 lobes, and depending on the observer, it could be argued that it had as many as 10 lobes, as they could be overlapped in the crowded neutrophil. We reviewed the peripheral blood smears daily during her hospital stay and observed a gradual decrease in the number of hypersegmented neutrophils and their nuclear lobes. On Day 9, hypersegmented neutrophils were still present, but their number was lower, with a maximum of 6 nuclear lobes. By Day 15, no hypersegmented neutrophils were present in the blood smear, consistent with Nath and Lindenbaum’s observations that hypersegmented neutrophils disappear by 14 days [12]. They observed no relationship between the severity of anemia and the degree of hypersegmentation [5]. However, we observed the number of nuclear lobes of hypersegmented neutrophils decrease as the Hb levels increase.
EXTREMELY HIGH SERUM MMA LEVELS WHICH TOOK A WEEK TO DECREASE:
The initial serum MMA level of our patient was 34 920 nmol/L (normal: 73–475 nmol/L). Elevated MMA is specific to vitamin B12 deficiency, unlike homocysteine levels, which can also be elevated in folate and pyridoxine deficiencies and hypothyroidism. It was reported that MMA levels tend to remain elevated for several days after vitamin B12 therapy [6]. In our patient, the MMA elevation persisted for over a week, probably due to its extremely high initial level, which took longer to be normalized.
NEUROPSYCHIATRIC IMPLICATIONS (PERIPHERAL NEUROPATHY AND POSSIBLY SCHIZOPHRENIA):
After cellular uptake and intracellular release of vitamin B12 in a normal situation, it is metabolized into its active forms, adenosylcobalamin and methylcobalamin, which act as essential cofactors for 2 key enzymatic reactions. A deficiency in vitamin B12 disrupts these pathways, resulting in elevated levels of methylmalonic acid (MMA) and homocysteine in the bloodstream. While increased homocysteine has been linked to neurodegenerative changes such as white matter damage, brain atrophy, and cognitive impairment, the precise impact of elevated MMA remains less well defined [1]. Peripheral neuropathy often is one of the earliest neurologic signs of vitamin B12 deficiency and can progress to subacute combined degeneration (SCD) of the spinal cord if left untreated. This condition usually presents symmetrically, predominantly affecting the lower extremities. On clinical examination, patients can have diminished sensation to vibration, pinprick, and light touch, along with hypoactive or absent deep tendon reflexes, especially at the ankles. Notably, neurologic deficits can occur even in the absence of anemia. Advanced cases of SCD can feature limb weakness, ataxia, and visual disturbances. Timely identification and treatment are essential, as early intervention with B12 replacement offers the best chance for neurological recovery before permanent damage sets in [1,4]. Our patient presented with mild peripheral neuropathy with numbness of both lower legs and absent DTR, which improved with vitamin B12 replacement therapy.
Neuropsychiatric symptoms, including those of schizophrenia, can be an initial manifestation or even the sole symptom of vitamin B12 deficiency [7]. Vitamin B12 levels are often low in hospitalized psychiatric patients with schizophrenia [13]. It is advisable to rule out vitamin B12 deficiency in patients with psychotic symptoms instead of directly diagnosing psychiatric disorders [14]. A recent longitudinal study (3849 patients, aged ≥50 years) revealed the relationship between low blood plasma B12/folate levels and depressive symptoms. Older adults with deficient-low B12 status had a 51% higher likelihood of developing depressive symptoms over 4 years, but no associations of folate status with incident depression were observed. These findings highlight the need to further explore the low-cost benefits of optimizing vitamin B12 status for depression in older adults [15]. In cases of established psychiatric disorders, it is advisable to maintain serum B12 levels within the higher normal range [7].
Although no detailed information about her psychiatry history was available, our patient was reportedly diagnosed with schizophrenia and started taking antipsychotic medications several years ago. As it takes about 10–12 years to clinically develop symptomatic PA, PA can begin with subclinical vitamin B12 deficiency [4]. Therefore, it may be possible that her diagnosis of schizophrenia coincided with the onset of PA several years ago. While it is unclear whether PA directly caused her schizophrenia or exacerbated underlying psychiatric conditions, this case underscores the importance of considering vitamin B12 deficiency in patients with psychiatric symptoms.
Conclusions
We present a severe case of pernicious anemia characterized by life-threatening anemia, unusually abundant hypersegmented neutrophils with many nuclear lobes, extremely high MMA levels, and improvement in schizophrenia symptoms following vitamin B12 replacement therapy. While it remains unclear whether the patient’s schizophrenia was directly caused by PA or PA exacerbated her underlying mental condition, she improved dramatically after correction of her vitamin B12 deficiency. Further investigation into the relationship between pernicious anemia and schizophrenia is warranted.

References
1. Vaqar S, Shackelford KB, Pernicious anemia: StatPearls May 8, 2023, Treasure Island (FL), StatPearls Publishing
2. Stabler SP, Clinical practice. Vitamin B12 deficiency: N Engl J Med, 2013; 368; 149-60
3. Htut TW, Thein KZ, Oo TH, Pernicious anemia: Pathophysiology and diagnostic difficulties: J Evid Based Med, 2021; 14(2); 161-69
4. Esposito G, Dottori L, Pivetta G, Pernicious anemia: The hematological presentation of a multifaceted disorder caused by cobalamin deficiency: Nutrients, 2022; 14(8); 1672
5. Lindenbaum J, Nath BJ, Megaloblastic anaemia and neutrophil hypersegmentation: Br J Haematol, 1980; 44(3); 511-13
6. Green R, Vitamin B12 deficiency from the perspective of a practicing hematologist: Blood, 2017; 129(19); 2603-11
7. Sahu P, Thippeswamy H, Chaturvedi SK, Neuropsychiatric manifestations in vitamin B12 deficiency: Vitam Horm, 2022; 119; 457-70
8. Vannella L, Lahner E, Osborn J, Annibale B, Systematic review: Gastric cancer incidence in pernicious anaemia: Aliment Pharmacol Ther, 2013; 37(4); 375-82
9. Shah SC, Piazuelo MB, Kuipers EJ, Li D, AGA clinical practice update on the diagnosis and management of atrophic gastritis: Expert review: Gastroenterology, 2021; 161(4); 1325-32e7
10. Esteves JM, Fernandes J, Oliveira Monteiro P, Surviving extreme anaemia: Eur J Case Rep Intern Med, 2021; 8(3); 002357
11. Carson JL, Noveck H, Berlin JA, Gould SA, Mortality and morbidity in patients with very low postoperative Hb levels who decline blood transfusion: Transfusion, 2002; 42(7); 812-18
12. Nath BJ, Lindenbaum J, Persistence of neutrophil hypersegmentation during recovery from megaloblastic granulopoiesis: Ann Intern Med, 1979; 90; 757-60
13. Silver H, Vitamin B12 levels are low in hospitalized psychiatric patients: Isr J Psychiatry Relat Sci, 2000; 37(1); 41-45
14. Zheng X, Qiu R, Zhang W, Vitamin B12 deficiency presenting as psychotic symptoms in a psychiatry department: A case report: Cureus, 2023; 15(12); e50492
15. Laird EJ, O’Halloran AM, Molloy AM, Low vitamin B12 but not folate is associated with incident depressive symptoms in community-dwelling older adults: A 4-year longitudinal study: Br J Nutr, 2023; 130(2); 268-75
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133