23 July 2025: Articles 
Percutaneous Closure of an Ischemic Ventricular Septal Rupture in a 73-Year-Old Man: A Case Report
Unusual clinical course, Management of emergency care, Rare disease
Carlos Andres Mejia-GomezDOI: 10.12659/AJCR.947065
Am J Case Rep 2025; 26:e947065






Abstract
BACKGROUND: Acquired ventricular septal defect is an uncommon complication of myocardial infarction that can require surgical repair. Percutaneous closure techniques avoid the risks associated with major cardiac surgery, particularly in elderly patients. This report presents the case of a 73-year-old man with a post-infarction ventricular septal defect successfully treated by percutaneous closure.
CASE REPORT: A 73-year-old man was admitted with ST-elevation myocardial infarction. Coronary angiography revealed 2-vessel disease, and successful stenting of the left anterior descending artery was performed. Transthoracic echocardiography demonstrated an apical ventricular septal defect. Given the patient’s hemodynamic stability, the heart team recommended delayed percutaneous closure. However, the patient requested voluntary discharge. He was readmitted 2 weeks later with dyspnea and chest pain. The defect was closed percutaneously due to technical feasibility, elevated surgical risk, and patient preference. Post-procedural recovery was uneventful, and he was in NYHA functional class I at outpatient follow-up.
CONCLUSIONS: Ischemic ventricular septal rupture is a rare but potentially fatal complication of transmural myocardial infarction, requiring prompt recognition and management by a heart team. Presentation ranges from chest pain or a new murmur to cardiogenic shock. Diagnosis relies on imaging modalities, including transthoracic or transesophageal echocardiography and cardiac magnetic resonance imaging. Management options include surgical and percutaneous closure, with ventricular septal rupture repair mortality exceeding 40%. Treatment selection depends on the patient’s clinical status and the size, location, and complexity of the defect. This report highlights the role of percutaneous closure in post-infarction ventricular septal rupture and illustrates a successful outcome in an elderly patient.
Keywords: Echocardiography, Myocardial Infarction, Septal Occluder Device, Ventricular Septal Rupture, Humans, Male, Aged, cardiac catheterization
Introduction
Myocardial infarction (MI) is a high-incident pathology and one of the main contributors to the overall burden of death and disability worldwide [1]. Transmural MI is associated with an increased risk of mechanical complications, including ventricular septal rupture (VSR) [2], even though timely reperfusion of MI has decreased the overall incidence of this event. Closure of the defect is the definitive treatment, but the type and timing of closure are still a matter of debate [3]. To date, no randomized trials have been published regarding the management of post-infarction VSR [4], and the literature on its percutaneous closure consists mainly of case series and case reports [5,6]. An analysis of the Society of Thoracic Surgeons data showed operative mortality of 42.9% after surgical repair [7], while a systematic review of observational series of percutaneous closure showed a 30-day mortality of 32% [8]. Comparing outcomes between management strategies remains difficult, due to selection bias and the scarcity of head-to-head data [4]. This report presents the case of a 73-year-old man with a post-infarction ventricular septal defect successfully treated by percutaneous closure.
Case Report
A 73-year-old man with a history of type 2 diabetes mellitus was admitted to the Emergency Department because of 3 days of oppressive retrosternal pain with no irradiation, increasing in intensity 3 hours before admission. On admission, the patient had tachycardia and diaphoresis and was normotensive, with a holosystolic murmur best heard in the lower left sternal border. The electrocardiogram showed ST segment elevation in anterior leads. Emergency coronary angiography revealed occlusion of the mid portion of the left anterior descending artery (LAD), considered the culprit lesion, and 80% of the right coronary artery (RCA); angioplasty and insertion of a drug-eluting stent in the mid-LAD was performed (Figure 1). A transthoracic echocardiogram (TTE) showed apical ballooning and dyskinesia, a preserved left ventricular ejection fraction (LVEF) of 65%, a 7-mm VSR in the apical septum, normal valvular function, and no evidence of pericardial effusion. The patient remained hemodynamically stable, without signs of heart failure, but persisted with moderate chest pain that improved with nitrates. Based on this, the heart team decided to perform percutaneous coronary intervention of the RCA, which was performed without complications, and a delayed percutaneous closure of the VSR. The patient was informed of the required 3-week hospital stay before the procedure and requested voluntary discharge, understanding the high risk of heart failure, cardiogenic shock, and death.
Two weeks later, he returned to the Emergency Department, due to progressive chest pain and dyspnea. Chest X-ray showed pulmonary edema. Medical treatment was initiated, including intravenous diuretics. A new echocardiogram revealed a stable LVEF, a 10-mm VSR, and an LV apical aneurysm; the heart team decided to pursue percutaneous closure of the septum defect. The procedure was performed with simultaneous fluoroscopic and transesophageal echocardiogram (TEE) guidance (Figures 2, 3). Considering the apical location of the defect, a femoral arterial/jugular venous loop using a guidewire was the selected approach to ease the manipulation of the occlusive device and ensure better final positioning. An intraprocedural ventriculogram was performed, revealing an asymmetric apical defect measuring 10 mm. TEE guidance using orthogonal-biplane imaging and 3-dimensional (3D) reconstruction with the Xplane technique showed an irregular VSD measuring 16×10 mm. A 24-mm Amplatzer Muscular VSD PI occluder was selected, considering 50% oversizing. From the arterial access, the septal defect was crossed with a 0.035” guidewire, toward the right ventricle, and externalized by the right internal jugular introducer. Via the venous route, the 6 Fr introducer was changed for a 10 Fr introducer, and under TEE guidance, the 2 discs of the septal occluder were deployed with adequate positioning on both sides; the device was released without complications. The patient was hemodynamically stable after the intervention. A post-procedure echocardiogram showed a 45% LVEF and a well-positioned device with moderate intraprosthetic and periprosthetic shunt. The patient was discharged with dual antiplatelet, betablocker, and high-intensity statin therapy.
At the follow-up outpatient appointment, he was asymptomatic at rest and exercise, classified as NYHA functional class I, normotensive, with a holosystolic murmur, and without any signs of heart failure. He was advised to continue cardiac rehabilitation and cardiology follow-up.
Discussion
This case report underscores the importance of a heart team approach in the management of post-infarction VSR, emphasizing the need for early clinical suspicion of mechanical complications of MI, comprehensive evaluation through multimodal cardiac imaging, and the development of individualized therapeutic strategies based on the patient’s clinical status and morphological features of the VSR.
Ischemic rupture of the ventricular septum is the most frequent mechanical complication of a transmural MI, usually presenting within the first week, particularly in the first 24 hours. It is mostly associated with anterior MI, due to single vessel perfusion of the anterior septum by the LAD. The presentation ranges from chest pain or heart murmur to severe hemodynamic compromise and cardiogenic shock [9]. Hemodynamically, the interventricular connection leads to a left-to-right shunt with volume overload of the right ventricle, pulmonary hyperflow, and left ventricular volume overload, eventually leading to left ventricular dysfunction [10]. Our patient was hemodynamically stable and presented with chest pain and dyspnea.
TTE is the image of choice to detect a VSR and characterize its size, location, and direction of the shunt, also allowing assessment of biventricular function and probability of pulmonary hypertension. TEE and 3D reconstruction with Xplane imaging are valuable for complex or irregularly shaped defects, displaying more precisely their morphology, sizing, rims, and adjacent structures [3,11]. Cardiac MRI is especially useful in difficult to assess areas, such as the apical septum [12]. Functional computed tomography provides higher spatial resolution than cardiac MRI and is useful in defects with complex anatomy or when cardiac MRI is contraindicated; however, radiation exposure must be considered [13]. The discrepancy in the size of the VSD in the preprocedural TTE and the intraprocedural TEE in the present case highlights the relevance of multimodal cardiac imaging in the evaluation and planning of the closure of a VSR.
In patients with acute symptoms, afterload reduction with vasodilators and inotropic agents is the mainstay of therapy, provided systolic blood pressure is greater than 90 mmHg. Periprocedural mechanical circulatory support, particularly intra-aortic balloon pump, could be considered in patients with unstable condition [6,14]. Given the high mortality rate of patients with an unclosed VSR, exceeding 90%, all defects must be closed unless a prohibitive risk exists [15].
Traditionally, surgical intervention was the mainstay of therapy, with a 42.9% in-hospital mortality in the Society of Thoracic Surgeons database [7]. Nowadays, with the advent of percutaneous techniques, the optimal closure strategy is not defined. Schlotter et al [8] published a systematic review of observational series regarding percutaneous post-MI VSR closure, reporting in-hospital or 30-day mortality of 32% among 273 patients, with mortality ranging from 18% to 75% in individual series. Giblett et al [16] conducted a retrospective review of 362 patients with post-infarction VSR across 16 centers in the United Kingdom (2010–2021), involving 416 interventions (131 percutaneous, 231 surgical). Procedural success was 88.3% in surgical closure and 79.4% in percutaneous closure. In-hospital mortality was 48.1% overall, higher in the percutaneous group (55.0% vs 44.2%,
Comparing outcomes between management strategies remains challenging due to the low volume of post-MI VSR procedures, the scarcity of head-to-head comparative data, and the presence of confounding factors and selection bias in observational studies, often related to patient age, frailty, hemodynamic stability, and the inclusion of centers where percutaneous repair is reserved for patients considered unsuitable for surgery [4,6].
Percutaneous closure is generally preferred in patients in stable condition with a simple defect less than 24 mm in diameter, an adequate rim for septal occluder device placement, and sufficient distance from the valve apparatuses. It is also considered when surgical intervention is not feasible or poses a prohibitive risk, as was the case in the report by Ishiyama et al [6]. On the other hand, surgical closure is favored in patients with hemodynamic instability, those with large, complex, or multiple defects, or in those for which there is another surgical indication, such as coronary bypass graft or valvular heart surgery [4].
In patients in stable condition, a delayed approach (2–3 weeks) has led to lower mortality rates in several studies, possibly due to a technically easier repair when fibrosis of the initially friable infarcted tissue has taken place [7,17]. Chen et al [5] reported that delayed closure beyond 3 weeks after MI was associated with a significantly lower 30-day mortality rate, compared with earlier interventions (12.5% vs 48%,
A delayed percutaneous approach was selected for our patient, who was hemodynamically stable, had an above average surgical risk of any complication (ACS-NSQIP surgical risk calculator), and had no other indications for cardiovascular surgery, presenting with an isolated defect measuring less than 24 mm, with adequate rim for the device anchoring and a distance greater than 5mm from the device disc to the apex, avoiding apical free wall contact of the device with systolic contraction. An Amplatzer Muscular VSD PI occluder with 50% oversizing was selected due to the friable nature of the infarcted tissue and risk of necrosis progression with enlargement of the VSD. The intervention was successful, and the post-procedural clinical course was satisfactory. This strategy mirrors that reported in previous publications [5,8,16] and underscores that appropriate timing, careful patient selection, and advanced imaging guidance are essential components to optimize outcomes in percutaneous closure of post-infarction VSR.
Conclusions
Ischemic VSR remains a rare but potentially fatal complication of MI. Early recognition and management by a heart team are critical. Closure of the defect is mandatory and can be achieved surgically or percutaneously depending on the patient’s clinical stability and anatomical characteristics, and institutional expertise. In our case, delayed percutaneous closure led to a successful outcome in a hemodynamically stable elderly patient.
Figures
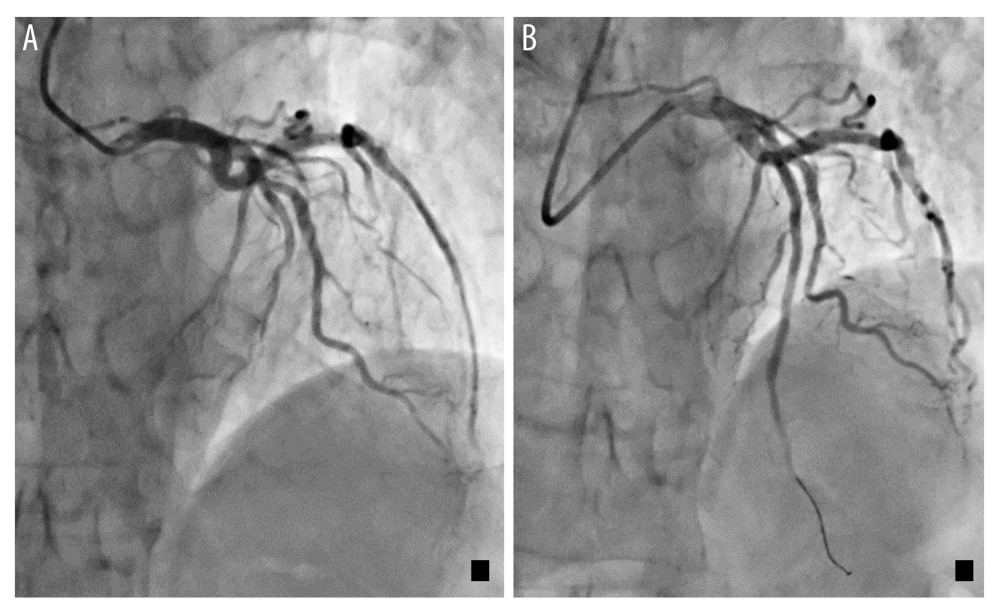 Figure 1. Coronary angiogram images showing (A) left anterior descending artery (LAD) occlusion; (B) LAD reperfusion after angioplasty and stent insertion.
Figure 1. Coronary angiogram images showing (A) left anterior descending artery (LAD) occlusion; (B) LAD reperfusion after angioplasty and stent insertion. 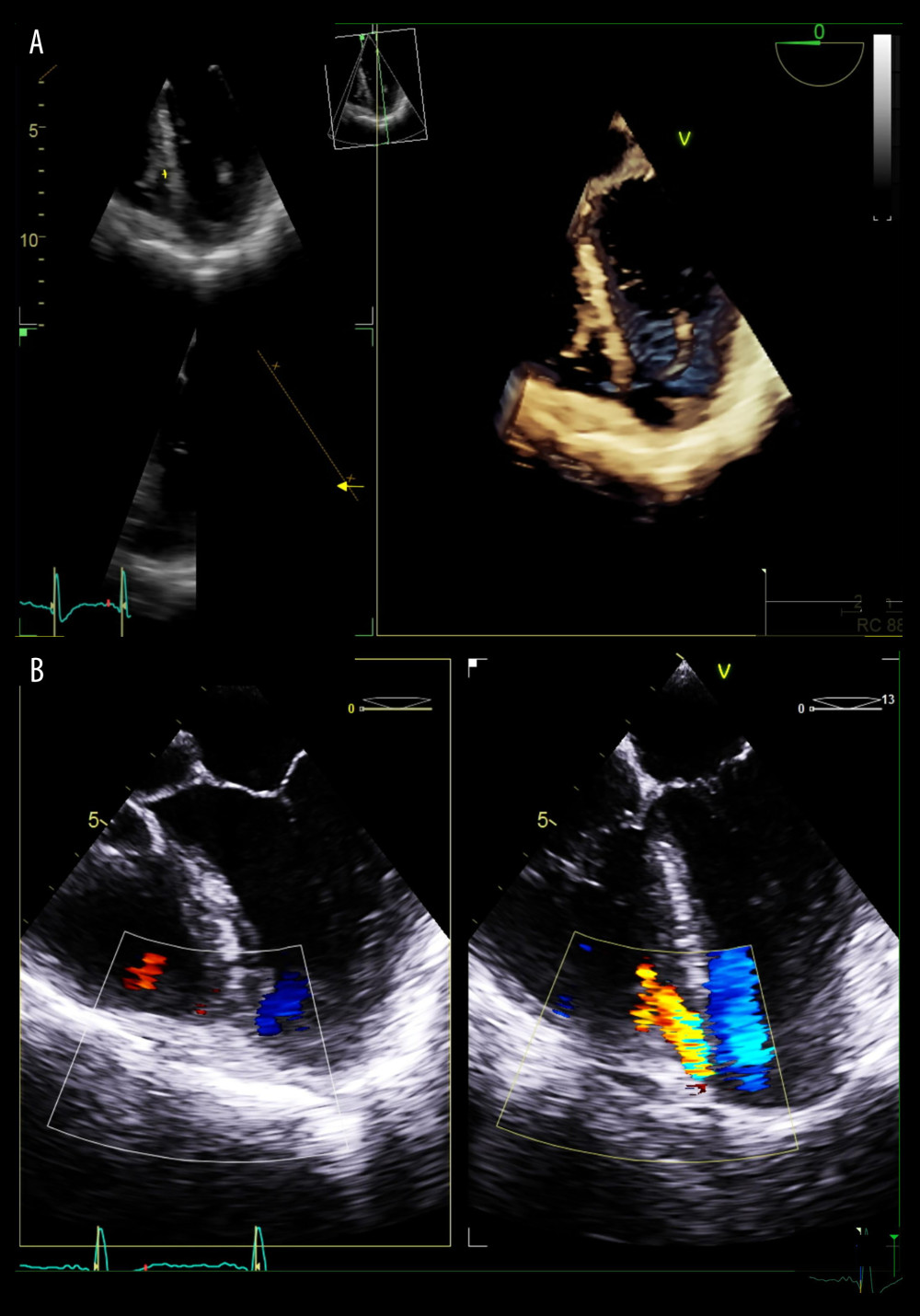 Figure 2. Preprocedural transesophageal echocardiogram with apical 4-chamber window. (A) 3D image of a ventricular septal defect (VSD) is shown at the junction of the septum and an apical ventricular aneurism measuring 10 mm. (B) Color Doppler of the VSD shows a left-to-right shunt.
Figure 2. Preprocedural transesophageal echocardiogram with apical 4-chamber window. (A) 3D image of a ventricular septal defect (VSD) is shown at the junction of the septum and an apical ventricular aneurism measuring 10 mm. (B) Color Doppler of the VSD shows a left-to-right shunt. 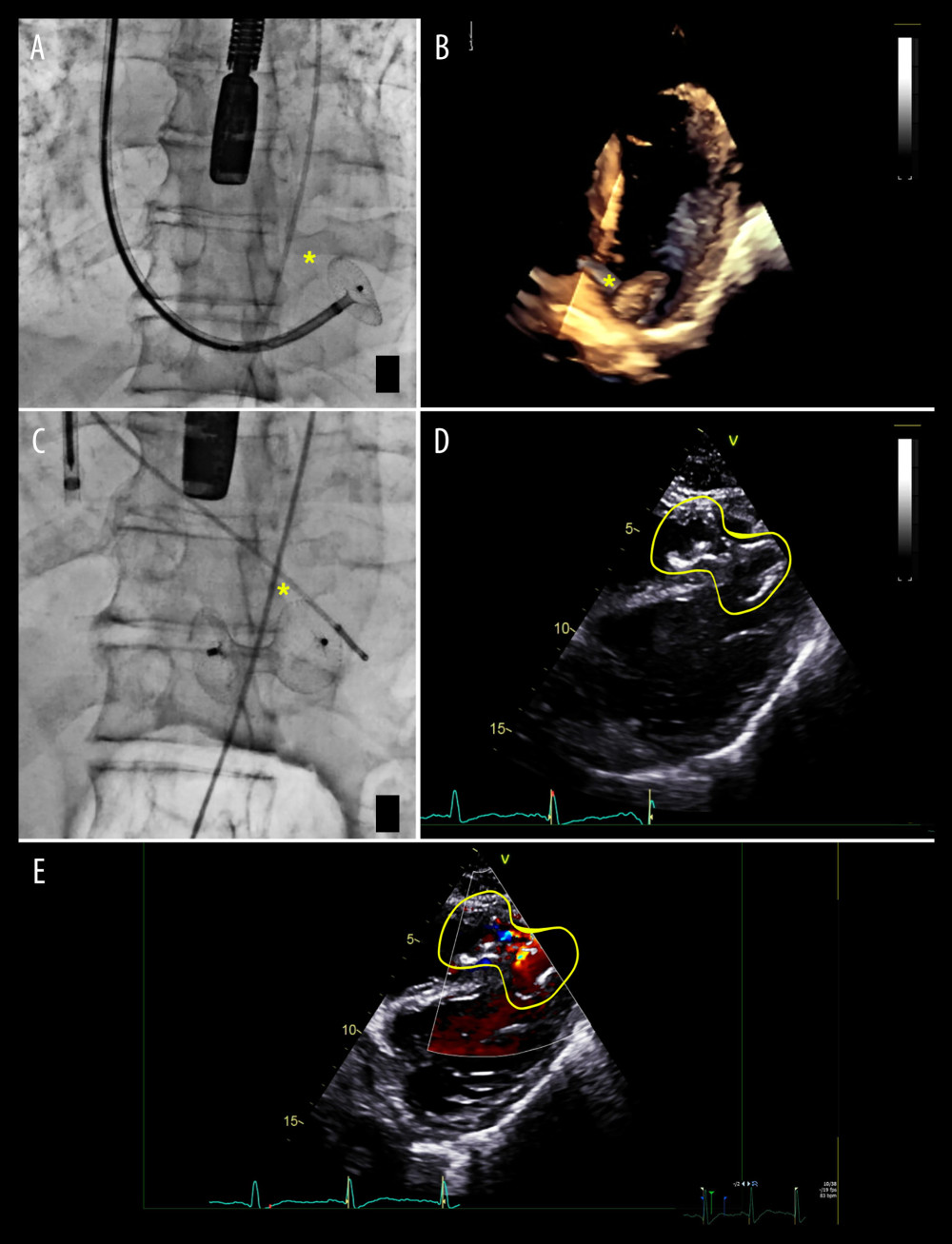 Figure 3. Fluoroscopic and transesophageal echocardiogram (TEE) guidance images showing (*) (yellow) septal defect closure device; (A, B) opening of the left disc on fluoroscopy (A) and 3D TEE (B); (C, D) properly positioned septal occluder on fluoroscopy (C) and TEE (D); and (E) TEE Doppler imaging: residual left-to-right shunt.
Figure 3. Fluoroscopic and transesophageal echocardiogram (TEE) guidance images showing (*) (yellow) septal defect closure device; (A, B) opening of the left disc on fluoroscopy (A) and 3D TEE (B); (C, D) properly positioned septal occluder on fluoroscopy (C) and TEE (D); and (E) TEE Doppler imaging: residual left-to-right shunt. References
1. World Health Organization: The top 10 causes of death [Internet] [cited 2024 Dec 4]. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
2. Elbadawi A, Elgendy IY, Mahmoud K, Temporal trends and outcomes of mechanical complications in patients with acute myocardial infarction: JACC Cardiovasc Interv, 2019; 12(18); 1825-36
3. Gong FF, Vaitenas I, Malaisrie SC, Maganti K, Mechanical complications of acute myocardial infarction: A review: JAMA Cardiol, 2021; 6(3); 341-49
4. Cadogan D, Daghem M, Snosi M, Percutaneous transcatheter closure of post-infarction ventricular septal defect: An alternative to surgical intervention: Interv Cardiol, 2023; 18; e19
5. Chen T, Liu Y, Zhang J, Percutaneous closure of ventricular septal rupture after myocardial infarction: A retrospective study of 81 cases: Clin Cardiol, 2023; 46(7); 737-44
6. Ishiyama M, Kurita T, Ishiura J, Successful percutaneous treatment of recurrent post-infarction ventricular septal rupture using an Amplatzer duct occluder: J Cardiol Cases, 2019; 21(1); 12-15
7. Arnaoutakis GJ, Zhao Y, George TJ, Surgical repair of ventricular septal defect after myocardial infarction: Outcomes from the Society of Thoracic Surgeons National Database: Ann Thorac Surg, 2012; 94(2); 436-43 discussion 443–44
8. Schlotter F, de Waha S, Eitel I, Interventional post-myocardial infarction ventricular septal defect closure: A systematic review of current evidence: EuroIntervention, 2016; 12(1); 94-102
9. Kutty RS, Jones N, Moorjani N, Mechanical complications of acute myocardial infarction: Cardiol Clin, 2013; 31(4); 519-31
10. Birnbaum Y, Fishbein MC, Blanche C, Siegel RJ, Ventricular septal rupture after acute myocardial infarction: N Engl J Med, 2002; 347(18); 1426-32
11. Charakida M, Qureshi S, Simpson JM, 3D echocardiography for planning and guidance of interventional closure of VSD: JACC Cardiovasc Imaging, 2013; 6(1); 120-23
12. Stauder NI, Miller S, Scheule AM, MRI diagnosis of a previously undiagnosed large trabecular ventricular septal defect in an adult after multiple catheterizations and angiocardiograms: Br J Radiol, 2001; 74(879); 280-82
13. Azarine A, Scalbert F, Garçon P, Cardiac functional imaging: Presse Med, 2022; 51(2); 104119
14. Tripathi A, Bisht H, Arya A, Ventricular septal rupture management in patients with acute myocardial infarction: A review: Cureus, 2023; 15(6); e40390
15. Menon V, Webb JG, Hillis LD, Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: A report from the SHOCK Trial Registry: SHould we emergently revascularize Occluded Coronaries in cardiogenic shocK? J Am Coll Cardiol, 2000; 36(3 Suppl A); 1110-16
16. Giblett JP, Matetic A, Jenkins D, Post-infarction ventricular septal defect: Percutaneous or surgical management in the UK national registry: Eur Heart J, 2022; 43(48); 5020-32
17. Jeppsson A, Liden H, Johnsson P, Surgical repair of post infarction ventricular septal defects: A national experience: Eur J Cardiothorac Surg, 2005; 27(2); 216-21
Figures
Figure 1. Coronary angiogram images showing (A) left anterior descending artery (LAD) occlusion; (B) LAD reperfusion after angioplasty and stent insertion.Figure 2. Preprocedural transesophageal echocardiogram with apical 4-chamber window. (A) 3D image of a ventricular septal defect (VSD) is shown at the junction of the septum and an apical ventricular aneurism measuring 10 mm. (B) Color Doppler of the VSD shows a left-to-right shunt.Figure 3. Fluoroscopic and transesophageal echocardiogram (TEE) guidance images showing (*) (yellow) septal defect closure device; (A, B) opening of the left disc on fluoroscopy (A) and 3D TEE (B); (C, D) properly positioned septal occluder on fluoroscopy (C) and TEE (D); and (E) TEE Doppler imaging: residual left-to-right shunt. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133