20 July 2025: Articles 
Surgical Approach to Littre’s Hernia: A Rare Presentation of Meckel’s Diverticulum
Rare coexistence of disease or pathology
João Maria Regueiras Mendes ABCDEFG 1*, Dimitrios ChatziisaakDOI: 10.12659/AJCR.947174
Am J Case Rep 2025; 26:e947174






Abstract
BACKGROUND: Littre’s hernia is a rare entity defined as the herniation of a Meckel’s diverticulum through a defect in the abdominal wall. Although Meckel’s diverticulum occurs in up to 2% of the population, its manifestation within a hernia is extremely rare, comprising around 1% of Meckel’s cases. This report describes the case of a 32-year-old man presenting as an emergency with lower abdominal pain and a diagnosis of Littre’s hernia.
CASE REPORT: A 32-year-old man presented with a 3-day history of lower abdominal pain and periumbilical erythema. Clinical examination revealed an irreducible umbilical hernia. Laboratory tests showed leukocytosis and elevated CRP. A CT scan suggested an incarcerated hernia with signs of ischemia, but no clear identification of Meckel’s diverticulum. Diagnostic laparoscopy followed by mini-laparotomy revealed a necrotic Meckel’s diverticulum 110 cm proximal to the ileo-cecal valve. A stapled diverticulectomy was performed without mesh repair due to contamination. The wound was managed with a vacuum-assisted closure (VAC) system. The postoperative course was uneventful, and histopathology confirmed necrotizing inflammation without malignancy.
CONCLUSIONS: Littre’s hernia is a rare but important differential diagnosis in abdominal wall hernias and can present symptomatically as an acute abdomen. This case highlights the presentation, diagnosis, and surgical management of an atypical umbilical Littre’s hernia and reinforces the value of prompt surgical exploration and intraoperative assessment to avoid ischemic complications.
Keywords: Diverticulum, Hernia, Abdominal, Meckel Diverticulum, Rare Diseases, Humans, Male, adult, Tomography, X-Ray Computed, Diagnosis, Differential, Laparoscopy, Abdominal Pain, herniorrhaphy
Introduction
An abdominal hernia is defined as the protrusion of the parietal peritoneum, which may contain a variety of contents, through one of the physiological or secondary abdominal hiatuses [1]. Although the prevalence of abdominal hernia in the general population is estimated to be about 1.7% for all ages [2], and abdominal hernia-repairs account about 15–17% of all surgical procedures [3], the incidence of a herniated Meckel diverticulum and consequently Littre hernias is low [4–7].
Meckel’s diverticulum is a relatively common congenital malformation, with a prevalence of approximately 2% in the adult population [6–8]. It is typically found in the last 100 cm of the Ileum in the antimesenteric border [6,7,9]. In most cases there are no symptoms [4,6,10]. However, symptoms include gastrointestinal bleeding, obstruction, inflammation of heterotopic gastric mucosa, or herniation [4]. The term ‘Littre’s hernia’ was first coined by Alexis Littre in the 17th century to describe an abdominal hernia containing the contents of the Meckel’s diverticulum. The name ‘diverticula acquisita’ was also proposed by Littre [4,10,11]. The incidence of Littre hernias is exceedingly low, manifesting in around 1% of Meckel’s diverticula cases [11,12]. Its embryological origin is proven to be insufficient closure of the omphalocentric duct (vitello-intestinal duct) after the sixth week of intrauterine life [13].
A Littre’s hernia is a rare condition that requires a high level of clinical suspicion and prompt diagnosis to ensure effective and safe treatment [5,6]. This report describes the case of a 32-year-old man presenting as an emergency with lower abdominal pain and a diagnosis of Littre’s hernia, highlighting the diagnostic and therapeutic considerations of this rare entity.
Case Report
PATIENT INFORMATION:
A 32-year-old White man presented to the Emergency Department at the Hospital of the Canton of St. Gallen with a 3-day history of sudden-onset lower-abdominal pain. The pain was localized to the periumbilical region and worsened with movement. He denied having nausea, vomiting, or altered bowel movements. He had no significant past medical history, no previous surgeries, and was not taking any medications.
CLINICAL FINDINGS:
On physical examination, the patient was alert, afebrile, and hemodynamically stable. Inspection revealed periumbilical erythema with localized tenderness. The abdomen was soft, with normal bowel sounds and no generalized peritonism. No other hernias were palpable.
DIAGNOSTIC ASSESSMENT:
The subsequent diagnostic workup of the patient revealed a leukocytosis (20 G/l) and elevated C-reactive protein (CRP) values (260 mg/l). Abdominal sonography indicated the presence of an incarcerated umbilical hernia, with no signs of free intra-abdominal fluid. To gain further insight, a computed tomography (CT) scan of the abdomen was conducted (Figures 1, 2). The radiologists finding read as follows: “Incarcerated umbilical hernia with predominantly pre-peritoneal herniated cecal pole with signs of ischemia and individual small gas formations that cannot be assigned to the lumen with certainty”.
This eliminated the possibility of either indirect or direct evidence of bowel perforation, thereby confirming the diagnosis of an incarcerated umbilical hernia with ischemic bowel content. The hernia content was not described as being a Meckel’s diverticulum.
After providing written informed consent, the patient was transferred to the operating room. A diagnostic laparoscopy was conducted. The incarcerated hernia was visualized (Figure 3). Following the unsuccessful repositioning of the hernia content and the potential risk of iatrogenic perforation of the bowel, a hybrid open repair was undertaken via mini-laparotomy. This revealed the presence of a Meckel’s diverticulum, which was identified as the incarcerated intestine and was located 110 cm proximal to the ileo-cecal valve (Figure 4). The location was atypical, as Meckel’s diverticulum is usually defined as being within 100 cm of the ileo-cecal valve.
A diverticulectomy was performed using a linear stapler due to the presence of necrotic tissue within the Meckel’s diverticulum. The hernia was closed without use of mesh due to the contamination caused by the necrotic intestine. A vacuum-assisted closure (VAC) system was used to manage the surgical incision.
The postoperative course was uneventful. The patient was discharged on the seventh postoperative day after secondary wound closure on the fourth day after surgery. There have been no reports of complications or recurrence since discharge.
The histopathological examination of the specimen corroborated the diagnosis of a necrotic perforation of a Meckel’s diverticulum in association with a coprolite: “A small bowel diverticulum with severe acute, ulcero-phlegmonous, predominantly necrotizing inflammation with transmural perforation and severe purulent-abscessed inflammation and necrosis of the surrounding fatty tissue as well as evidence of a large coprolith (diameter 2 cm) within the necrosis. Adjacent to this was a second, vital and largely inflammation-free diverticulum of the small intestine. No malignancy.”
Discussion
This case highlights the clinical significance of a rare and diagnostically challenging entity: a strangulated Littre’s hernia in an umbilical location. Littre’s hernia is one of the rarest complications of a Meckel’s diverticulum, characterized by its protrusion with the abdominal peritoneum through a natural or secondary opening of the abdominal wall. Since its initial description 4 centuries ago, the precise incidence of this condition has remained uncertain. A recent publication by Racareanu et al [5] reviewed 98 cases in total in 2022. This constellation – umbilical Littre’s hernia with strangulation and necrosis – is extremely uncommon and is rarely reported in the literature. This condition is exceedingly rare and should be considered alongside the so-called mixed Littre’s hernias, which also contain small intestine or other abdominal viscera within the sac of the hernia alongside the Meckel’s diverticulum [14].
Despite the origin of the Meckel’s diverticulum as a remnant of the omphalomesenteric duct, the location of Littre’s hernia is rarely umbilical [15]. The umbilical hernia seems to be one of the rarest, while the inguinal hernia and the femoral hernia seem to be the most common, depending on the publication [15–17]. In their systematic literature review, Schizas et al found that most of the hernias (39.6%) were femoral hernias and 34% were inguinal hernias. The remaining cases were classified as umbilical hernias (11.3%), with obturator hernias accounting for a further 5.7% [6].
Preoperative diagnosis of a Littre’s hernia appears to be nearly impossible. While physical examination can raise suspicion for strangulation and bowel obstruction, comprehensive diagnostic evaluation with sonography and CT is generally required to confirm the diagnosis and plan appropriate management [18]. Although a recent radiologic review described characteristic imaging features of Littre’s hernia [19], the definitive diagnosis in most cases – including ours – remains an intraoperative finding [20].
Similar cases of Littre’s hernia have been recently reported, showing both the rarity and variability of clinical presentation and surgical management. Khalifa et al described a pediatric case of umbilical Littre’s hernia presenting with small-bowel obstruction, where preoperative imaging was inconclusive and intraoperative findings led to a wedge resection of a strangulated Meckel’s diverticulum [21]. Evola et al reported an adult case of recurrent umbilical hernia containing an uncomplicated Meckel’s diverticulum, discovered intraoperatively; the diverticulum was left in place and the hernia was repaired with mesh [16]. Pinto et al presented the case of a man with a femoral Littre’s hernia, where the Meckel’s diverticulum was resected and hernia repair performed via a pre-peritoneal approach [22].
A further crucial element in the management of these patients is the intraoperative decision on how to manage the Meckel’s diverticulum once it has been successfully repositioned within the abdominal cavity. In cases where a diagnosis of strangulation with necrosis has been made, the decision to perform either a diverticulectomy or a resection of a part of the small intestine with direct anastomosis is mandatory. A recent publication by Rahmat et al indicates that there is currently no clear consensus regarding the resection of asymptomatic Meckel’s diverticula [23]. In their study, Park et al retrospectively analyzed the data of 1476 patients. They found that Meckel’s diverticula fulfilling 4 specific criteria should be resected. The identified risk factors were as follows: a) patients under the age of 50 years old, b) male sex, c) diverticulum less than 2 cm, and d) presence of histologically abnormal tissue [4]. While these criteria are undoubtedly useful for the management of Meckel’s diverticula, the question of whether the fourth criterion is applicable in the context of an emergency surgical procedure ultimately depends on the availability of resources. Taking into consideration the data presented by the Racareanu group, which reported the presence of ectopic tissue or tumors in the herniated Meckel’s diverticulum of 42% of cases [5], and the findings of Park et al (2005), which indicated the presence of up to 33% ectopic tissue and up to 2% involved carcinoid, the evaluation of any Meckel’s diverticulum found during surgery – especially in the context of a Littre’s hernia – should include a careful histopathological assessment to rule out malignancy and guide further management. Park et al also found no complications attributable to Meckel’s diverticulum resection in 100 cases [4]. It can be concluded that diverticulectomy is the safest procedure when considering the potential complications [5].
The surgical technique employed for the closure of an abdominal hernia remains at the discretion of the surgeon, with consideration given to the presence of infection. In general, adherence to international guidelines is the optimal approach.
In our case, a hybrid approach was deemed the most appropriate course of action to prevent unnecessary contamination and postoperative complications. This approach was selected in accordance with the literature on the subject [24].
Conclusions
Littre’s hernia is a rare and often unexpected cause of acute abdomen. This case emphasizes the importance of considering Littre’s hernia in differential diagnosis, the limitations of preoperative imaging, and the need for prompt surgical exploration. Intraoperative assessment remains key to diagnosis and appropriate management.
Figures
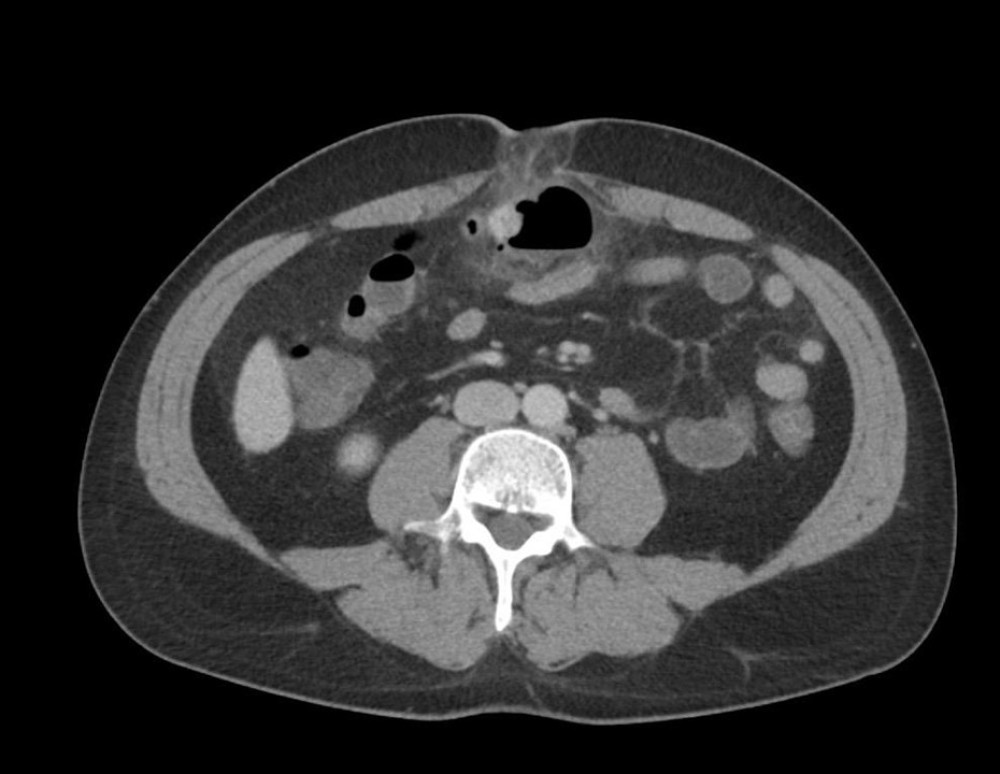 Figure 1. CT scan showing umbilical hernia with coprolith and ischemic signsAxial contrast-enhanced CT scan showing an umbilical hernia containing small-bowel loops and a rounded structure consistent with a coprolith (fecalith). Surrounding fat stranding indicates inflammatory changes and early signs of ischemia.
Figure 1. CT scan showing umbilical hernia with coprolith and ischemic signsAxial contrast-enhanced CT scan showing an umbilical hernia containing small-bowel loops and a rounded structure consistent with a coprolith (fecalith). Surrounding fat stranding indicates inflammatory changes and early signs of ischemia.  Figure 2. CT scan showing progression of herniated content and inflammationAxial CT scan at a slightly cranial level showing progression of herniated pre-peritoneal content with surrounding fat stranding and air inclusions. The abdominal wall defect and location of the incarcerated segment are clearly visible.
Figure 2. CT scan showing progression of herniated content and inflammationAxial CT scan at a slightly cranial level showing progression of herniated pre-peritoneal content with surrounding fat stranding and air inclusions. The abdominal wall defect and location of the incarcerated segment are clearly visible. 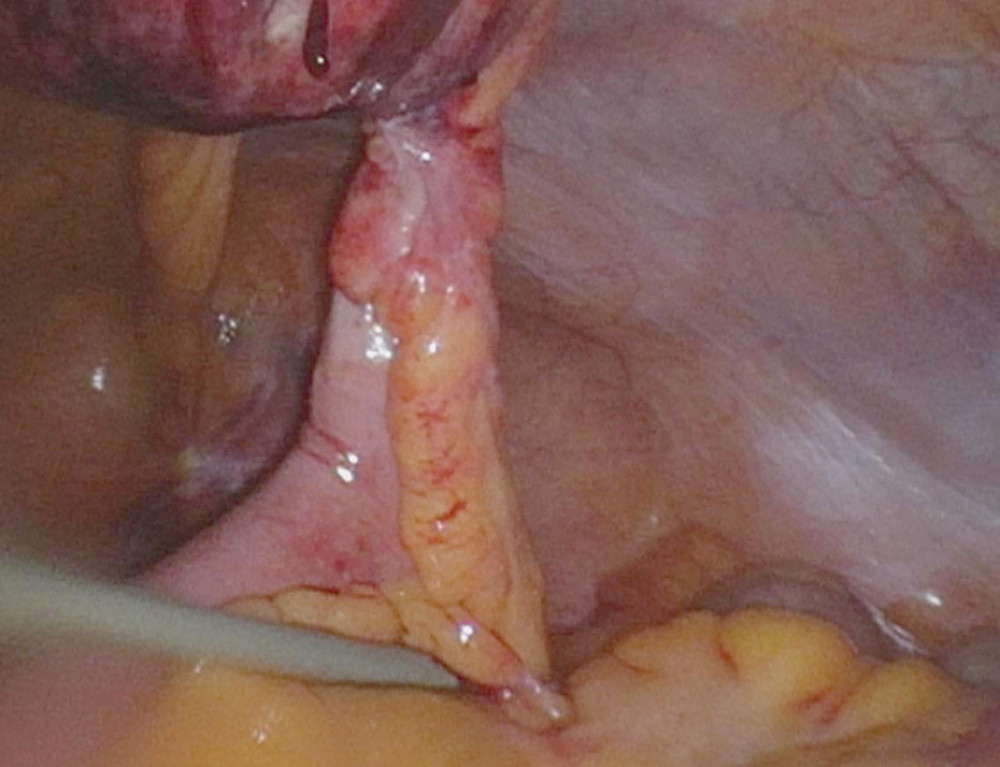 Figure 3. Laparoscopic view of incarcerated Meckel’s diverticulumIntraoperative laparoscopic view showing the incarcerated and ischemic Meckel’s diverticulum protruding into the umbilical hernia sac. The antimesenteric location and inflammatory reaction of the surrounding tissue are visible.
Figure 3. Laparoscopic view of incarcerated Meckel’s diverticulumIntraoperative laparoscopic view showing the incarcerated and ischemic Meckel’s diverticulum protruding into the umbilical hernia sac. The antimesenteric location and inflammatory reaction of the surrounding tissue are visible.  Figure 4. Resected specimen showing Meckel’s diverticulum with necrosis and coprolithIntraoperative image following mini-laparotomy. The star marks the viable ileum, and the arrow points to the resected Meckel’s diverticulum with signs of necrosis and perforation. A large coprolith is visible within the diverticulum tip.
Figure 4. Resected specimen showing Meckel’s diverticulum with necrosis and coprolithIntraoperative image following mini-laparotomy. The star marks the viable ileum, and the arrow points to the resected Meckel’s diverticulum with signs of necrosis and perforation. A large coprolith is visible within the diverticulum tip. References
1. Holzheimer RG, Mannick JA: Surgical treatment: Evidence-based and problem-oriented, 2001, Munich, Zuckschwerdt Copyright© 2001, W. Zuckschwerdt Verlag GmbH
2. Jenkins JT, O’Dwyer PJ, Inguinal hernias: BMJ, 2008; 336(7638); 269-72
3. Kingsnorth A, LeBlanc K, Hernias: Inguinal and incisional: Lancet, 2003; 362(9395); 1561-71
4. Park JJ, Wolff BG, Tollefson MK, Meckel diverticulum: The Mayo Clinic experience with 1476 patients (1950–2002): Ann Surg, 2005; 241(3); 529-33
5. Răcăreanu M, Preda SD, Preda A, Management of Littre hernia – case report and systematic review of case reports: J Clin Med, 2023; 12(11); 3743
6. Schizas D, Katsaros I, Tsapralis D, Littre’s hernia: A systematic review of the literature: Hernia, 2019; 23(1); 125-30
7. Meyerowitz BR, Littre’s hernia: Br Med J, 1958; 1(5080); 1154-56
8. Matsagas MI, Fatouros M, Koulouras B, Giannoukas AD, Incidence, complications, and management of Meckel’s diverticulum: Arch Surg, 1995; 130(2); 143-46
9. Horkoff MJ, Smyth NG, Hunter JM, A large incarcerated Meckel’s diverticulum in an inguinal hernia: Int J Surg Case Rep, 2014; 5(12); 899-901
10. Sagar J, Kumar V, Shah DK, Meckel’s diverticulum: A systematic review: J R Soc Med, 2006; 99(10); 501-5
11. Littre AObservation on a new species of hernia: Mem Acad r Sci Paris; 1700
12. Messina M, Ferrucci E, Meucci D, Littre’s hernia in newborn infants: Report of two cases: Pediatr Surg Int, 2005; 21(6); 485-87
13. Skandalakis PN, Zoras O, Skandalakis JE, Mirilas P, Littre hernia: Surgical anatomy, embryology, and technique of repair: Am Surg, 2006; 72(3); 238-43
14. Balani A, Marda SS, Alwala S, Perforated Littre’s hernia diagnosed on imaging: Case report and review of literature: Jpn J Radiol, 2015; 33(6); 366-69
15. Haber JJ, Meckel’s diverticulum; Review of literature and analytical study of 23 cases with particular emphasis on bowel obstruction: Am J Surg, 1947; 73(4); 468-85
16. Evola G, Piazzese E, Bonanno S, Complicated Littre’s umbilical hernia with normal Meckel’s diverticulum: A case report and review of the literature: Int J Surg Case Rep, 2021; 84; 106126
17. Citgez B, Yetkin G, Uludag M, Littre’s hernia, an incarcerated ventral incisional hernia containing a strangulated meckel diverticulum: Report of a case: Surg Today, 2011; 41(4); 576-78
18. HerniaSurge Group, International guidelines for groin hernia management: Hernia, 2018; 22(1); 1-165
19. Ghahremani GG, Littre hernia in adults: Imaging features and clinical implications: Abdom Radiol (NY), 2025 [Online ahead of print]
20. De Simone B, Birindelli A, Ansaloni L, Emergency repair of complicated abdominal wall hernias: WSES guidelines: Hernia, 2020; 24(2); 359-68
21. Khalifa MB, Belaid AB, Ghannouchi M, Umbilical Littre hernia: A rare case report of an acute abdomen: Int J Surg Case Rep, 2024; 114; 109182
22. Pinto J, Viana CM, Pereira A, Falcão J, Littré’s hernia: BMJ Case Rep, 2019; 12(2); e228784
23. Rahmat S, Sangle P, Sandhu O, Does an incidental Meckel’s diverticulum Warrant resection?: Cureus, 2020; 12(9); e10307
24. Blouhos K, Boulas KA, Tsalis K, Meckel’s diverticulum in adults: Surgical concerns: Front Surg, 2018; 5; 55
Figures
Figure 1. CT scan showing umbilical hernia with coprolith and ischemic signsAxial contrast-enhanced CT scan showing an umbilical hernia containing small-bowel loops and a rounded structure consistent with a coprolith (fecalith). Surrounding fat stranding indicates inflammatory changes and early signs of ischemia.Figure 2. CT scan showing progression of herniated content and inflammationAxial CT scan at a slightly cranial level showing progression of herniated pre-peritoneal content with surrounding fat stranding and air inclusions. The abdominal wall defect and location of the incarcerated segment are clearly visible.Figure 3. Laparoscopic view of incarcerated Meckel’s diverticulumIntraoperative laparoscopic view showing the incarcerated and ischemic Meckel’s diverticulum protruding into the umbilical hernia sac. The antimesenteric location and inflammatory reaction of the surrounding tissue are visible.Figure 4. Resected specimen showing Meckel’s diverticulum with necrosis and coprolithIntraoperative image following mini-laparotomy. The star marks the viable ileum, and the arrow points to the resected Meckel’s diverticulum with signs of necrosis and perforation. A large coprolith is visible within the diverticulum tip. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133