24 May 2025: Articles 
Recurrent Angiomatous Meningioma in a Young Adult: A Case Report
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Viktorija Loginova ABCDEF 1, Raimonds Mikijanskis BCD 2, Daira Krišāne BCD 3,4, Inese BriedeDOI: 10.12659/AJCR.947185
Am J Case Rep 2025; 26:e947185






Abstract
BACKGROUND: Meningiomas stand as the predominant primary intracranial tumors, encompassing a broad spectrum of histological variations. Within this spectrum, angiomatous meningiomas are notable for their significant vascularity within the tumor structure and rarity, making up only 2.1% of all meningiomas. These tumors typically present with slow-onset symptoms, commonly manifesting as seizures and compression-related effects. This report describes a 27-year-old man presenting with seizures and a diagnosis of angiomatous meningioma with postoperative recurrence, emphasizing the challenges in imaging, diagnosis, and disease management.
CASE REPORT: A 27-year-old man presented with a generalized seizure and unconsciousness. He had a history of exposure to chemicals from road construction and logging and smoked for 7 pack years. Initial CT scan revealed a 2.8-cm irregular tumor on the convex surface of his right frontal lobe. Craniotomy and resection of the lesion revealed angiomatous meningioma (central nervous system [CNS] World Health Organization [WHO] grade I). Six months later, control MRI showed recurrence at the excision site (2.4×2.0×1.4 cm). Re-craniotomy confirmed atypical meningioma (CNS WHO grade 2), and the patient received postoperative radiotherapy (56 Gy).
CONCLUSIONS: This case report highlights the importance of MRI in diagnosing angiomatous meningioma, a rare subtype comprising only 2.1% of all meningiomas. Although the tumor was initially resected successfully, its rapid recurrence as a WHO grade 2 atypical meningioma within 6 months underscores the surgical challenges and high recurrence risk associated with its vascular nature. These findings emphasize the need for careful postoperative monitoring and management.
Keywords: Angiomatosis, Central Nervous System, Magnetic Resonance Imaging, Meningioma, Oncology Service, Hospital, Humans, Male, Meningeal Neoplasms, adult, Neoplasm Recurrence, Local, Craniotomy, Tomography, X-Ray Computed
Introduction
Meningiomas are the most common type of primary intracranial tumor, originating from the meninges, the protective membranes surrounding the brain [1]. They present a diverse group with various histological subtypes. Among these subtypes, angiomatous meningiomas are notable for being uncommon and having a significantly vascular composition, with more than 50% of the entire tumor comprised of blood vessels. These tumors constitute a minor proportion of all meningiomas, specifically only 2.1% [2,3].
The classification of angiomatous meningiomas as World Health Organization (WHO) grade I tumors underscores their typically benign nature, lacking cellular atypia and anaplasia [4,5]. The 2021 WHO update introduced a molecular-based grading system for meningiomas, highlighting critical prognostic markers. Treatment options, including observation, surgery, and radiotherapy, vary based on patient and tumor characteristics [6].
Angiomatous meningioma typically manifests as a slow onset of progressively developing symptoms. The primary symptoms arise from the tumor pressing on nearby structures, causing seizures and compression-related effects [1,3].
One of the challenges with radiological findings in angiomatous meningiomas is their resemblance to other meningioma subtypes, making accurate differentiation through imaging alone difficult. Angiomatous meningiomas typically exhibit a low signal on T1-weighted imaging and a high signal on T2-weighted imaging. High frequency of peritumoral edema, which is often moderate to severe, along with uniform enhancement, is also observed [7].
The vivid contrast enhancement and vascularity seen in angiomatous meningiomas can sometimes be misinterpreted as high-grade tumors or more aggressive lesions, leading to diagnostic dilemmas [8–10].
Epithelial membrane antigen (EMA) and progesterone receptors are 2 markers used in the immunohistochemical analysis of tumors. Angiomatous meningiomas typically show positive EMA staining, among other meningioma subtypes. At the same time, they can demonstrate variable expressions of progesterone receptors [11,12].
Since angiomatous meningioma has an extremely rich blood supply, and intraoperative hemorrhage can occur, the operation is more difficult than in the case of conventional meningiomas. While surgical resection remains the primary management approach, the potential for recurrence and the role of adjuvant therapies in cases of incomplete resection or regrowth necessitate a more comprehensive understanding of the behavior and treatment strategies for angiomatous meningiomas [13]. This report describes a 27-year-old man presenting with seizures and a diagnosis of angiomatous meningioma with postoperative recurrence.
Case Report
A 27-year-old man presented with a generalized convulsive seizure and loss of consciousness and ultimately received a diagnosis of angiomatous meningioma with postoperative recurrence.
The patient had worked for 10 years in road construction and for the last 5 years in logging, where he was exposed to the effects of chemicals, specifically the effects of fuel and oil. The patient was a smoker with a history of 7 pack years.
A computed tomography (CT) examination of the head was performed natively. In the right hemisphere of the brain, an irregularly shaped lesion about 2.8 cm in size was visualized. Areas of heterogeneous hypodense edema around the tumor were seen. Due to cerebral edema around the lesion, a slight deformation of the occipital horn of the right lateral ventricles was observed. There was no evidence of acute ischemia or hemorrhage. A differential diagnosis was made between a malignant volume process or an atypical edematous meningioma (Figure 1).
On the following day, magnetic resonance imaging (MRI) of the head with intravenous contrast was performed. Located on the convex region of the parietal lobe of the right hemisphere, there was an extra-axial lesion of irregular shape, with slightly polycyclic contours, about 2.5×1.6 cm in diameter, and a homogeneous structure. After the administration of contrast, it accumulated uniformly and intensively. Pronounced perifocal edema around the tumor was noted. The tumor was associated with the meninges (Figure 2).
With the patient’s agreement, surgical therapy was indicated. A craniotomy in the right parietal region was performed shortly after radiological findings, followed by resection of the lesion. After surgery, the tissue obtained was sent for pathohistological examination. The material consisted of round-shaped cells chaotically arranged in different directions. Multiple blood vessels of small caliber were seen in the tissues, along with focal blood effusions. Glial fibrillary acidic protein was negative, progesterone was focally positive, EMA was focally positive, CD34 was positive in blood vessels, Ki-67 was positive at 4–5%, CD10 was negative, and S-100 was focally positive. Areas of atypical meningioma and mitoses were not visualized. Despite the Ki-67 proliferation index being focally slightly higher, this can be considered a common feature in meningiomas. The morphological and immunohistochemical picture was consistent with angiomatous meningioma, central nervous system (CNS) WHO Grade 1 (Figure 3).
Six months after the surgery, an MRI of the head was undertaken as a follow-up. In the right parietal lobe, at the site of excision, there was a postoperative space with hemosiderin deposits. An irregularly shaped, polycyclic extra-axial lesion measuring 2.4×2.0×1.4 cm in antero-posterior × latero-lateral × cranio-caudal directions was observed. After contrast administration, the tissues of the lesion steadily and intensely accumulated it. Perifocal edema had spread around the tumor. The meningioma was associated with the meninges. Recurrence of a convexity meningioma above the right parietal lobe was suspected (Figures 4, 5).
After a week, the patient was hospitalized for planned surgical treatment of a recurrence of an intracranial, extra-axial tumor. A recraniotomy of the right temporal region and resection of a recurrence of an unspecified tumor in the right temporal lobe area were performed (Figures 6, 7).
The MRI of the head after the osteoplastic recraniotomy and resection of the lesion was performed. In the surgical cavity, blood products were seen, and there were no indications of residual tumor tissue. Extensive perifocal edema was observed. According to the MRI data, taking into account the pathology data, it was more likely an atypical meningioma (Figure 8).
Due to the time in which the recurrence of the tumor developed, the result of the first pathohistological examination may not have corresponded to grade I. Therefore, the material from the previous operation was re-examined, but the answer remained the same: angiomatous meningioma, CNS WHO grade I.
The material of the recurrent tumor was highly cellular, consisting of meningothelial and some spindle-shaped cells with visible nuclei, showing focal layering of nuclei. Four to five mitotic figures were visualized in 10 high-magnification fields of view. EMA was overwhelmingly positive, progesterone was punctate positive, and Ki-67 was 12–15%. The morphological and immunohistochemical picture corresponded to an atypical meningioma, CNS WHO grade 2 (Figure 9).
Considering the rapid recurrence of the lesion, postoperative radiotherapy to the surgical area was strongly recommended. The patient received radiotherapy with 2 Gy to 56 Gy within a month.
Discussion
The aim of our case to demonstrate the importance of understanding the behavior and progression of angiomatous meningiomas, particularly when atypical features are present. It underscores the necessity of considering potential recurrence, even in benign tumors, and the influence of factors such as surgical resection extent and tumor location. By analyzing this case, we aim to provide insights into the management of these rare tumors, emphasizing the role of long-term follow-up, molecular analysis, and postoperative therapies like radiotherapy to reduce recurrence risks.
This case emphasizes the unpredictable nature of some meningiomas and the possibility of the tumor grade changing upon recurrence. The complexity of the situation is likely impacted by the extent of initial resection, the tumor’s anatomical location, and the age of the patient.
Although angiomatous meningioma is classified as a WHO grade 1 tumor, it can exhibit atypical histopathological features. To assign atypical CNS meningioma WHO grade 2 criteria must be met, according to WHO Classification of CNS tumors [14]. These atypical characteristics could contribute to its recurrence, despite its generally benign classification. Previous research indicates that there could be a connection between the Ki-67 index in grade 1 meningiomas with atypical features and the progression/recurrence (P/R) rate. Marciscano et al reported actuarial P/R rates for tumors based on the Ki-67 index. For tumors with a Ki-67 index below 3%, the incidence was 2.4% (95% CI: 0.6–9.3) at 1 year and 16.3% (95% CI: 8.5–30.0) at 5 years. In comparison, tumors with a Ki-67 index of 3% or higher had rates of 10.6% (95% CI: 4.9–22.1) at 1 year and 31.2% (95% CI: 18.6–49.1) at 5 years. Furthermore, the presence of any atypical features – such as increased cellularity, sheeting, a high nuclear-to-cytoplasmic ratio, necrosis, or prominent nucleoli – was associated with a significantly elevated risk of P/R (hazard ratio [HR]: 2.4;
The recurrence rate in benign meningioma with atypical features could also be associated with the extent of the operation, as described by Marciscano et al. Patients with Simpson grade 2–4 resection without atypical features (intermediate risk) had a significantly increased risk of P/R (HR=16.0;
The research indicates that meningiomas exhibit significant genetic diversity. The most frequently modified gene is the tumor suppressor merlin (NF2), with mutations occurring in about 45% of cases. Additionally, several other genes are often associated with these tumors, including TRAF7, AKT1, KLF4, PIK3CA, and SMO [4,8]. In an analysis involving 553 meningioma samples conducted by Yuzawa et al., the mutation frequencies for these genes were recorded as follows: 20%, 9%, 9%, 4.5%, and 3% [9,16].
The absence of genetic or molecular analysis can lead to overlooking critical factors, allowing a tumor initially classified as grade 1 to potentially progress to a grade 2 tumor, due to its underlying genetic background. Incorporating such analyses into routine evaluation could provide a more accurate prognosis and help in identifying cases with a higher potential for aggressive behavior.
Challenges can arise in achieving complete surgical removal of meningioma masses, resulting in increased recurrence rates. Thus, considering adjuvant treatment after surgery, especially in cases in which complete mass removal is unattainable, is strongly recommended to minimize the risk of recurrence. Studies, such as the report by Liu et al on the clinical characteristics and treatment of angiomatous meningiomas, further support the importance of postoperative management [2]. Considering our patient’s successful tolerance of radiotherapy following surgery, coupled with the absence of recurrence thus far, we recommend the consideration of radiotherapy as a post-surgical treatment option.
The return of a meningioma, especially with an escalation in grade, vividly reflects the necessity for long-term follow-up and close collaboration between clinicians and patients, allowing for the timely detection of recurrences and the implementation of appropriate therapeutic interventions.
Our study is particularly valuable because it presents rare and highly accurate radiological and histopathological images, which are scarce in current literature. These images contribute to a deeper and more precise approach to managing meningiomas in young adults, a demographic often overlooked in existing research, which predominantly examines older patients with mostly benign cases. By offering a detailed visual resource, our work not only broadens the existing knowledge but also serves as a valuable reference for future clinical studies and practical applications.
Conclusions
This case report highlights the critical role of MRI in diagnosing angiomatous meningioma, a rare subtype accounting for only 2.1% of meningiomas. Although the initial removal was successful, the rapid recurrence of a WHO grade 2 atypical meningioma within 6 months highlights the significant surgical challenges and the tumor’s aggressive nature, emphasizing the need for close postoperative monitoring and management. Considering the rapid recurrence of the tumor, postoperative radiotherapy to the surgical area is strongly recommended.
Figures
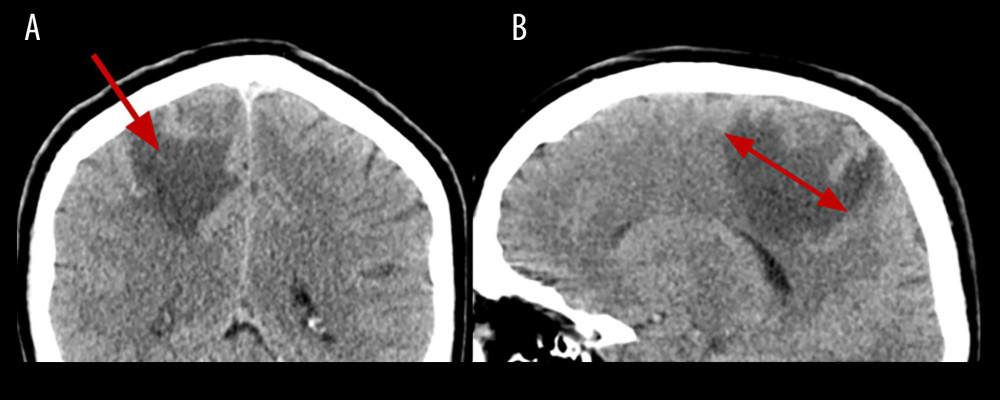 Figure 1. The head native CT with reconstructions in the coronal plane (A) and sagittal plane (B) zoomed in. In the right hemisphere of the brain an irregularly shaped lesion around 2.8 cm. Areas of heterogeneous hypodense edema around the lesion.
Figure 1. The head native CT with reconstructions in the coronal plane (A) and sagittal plane (B) zoomed in. In the right hemisphere of the brain an irregularly shaped lesion around 2.8 cm. Areas of heterogeneous hypodense edema around the lesion. 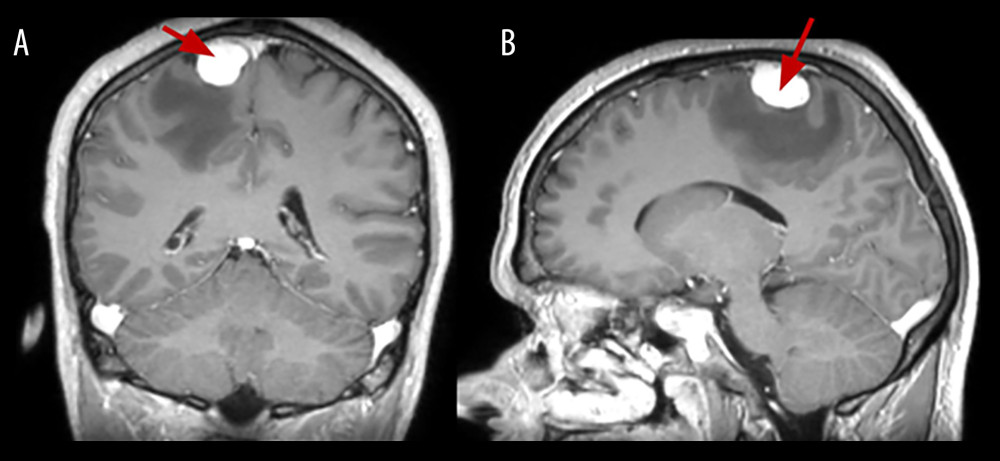 Figure 2. The brain MRI sequence T1 after contrast injection in the coronal plane (A) and sagittal plane (B). On the convex surface of the parietal lobe of the right hemisphere is about 2.5×1.6 cm homogeneous lesion. Accumulation of the contrast is consistent and intensive.
Figure 2. The brain MRI sequence T1 after contrast injection in the coronal plane (A) and sagittal plane (B). On the convex surface of the parietal lobe of the right hemisphere is about 2.5×1.6 cm homogeneous lesion. Accumulation of the contrast is consistent and intensive. 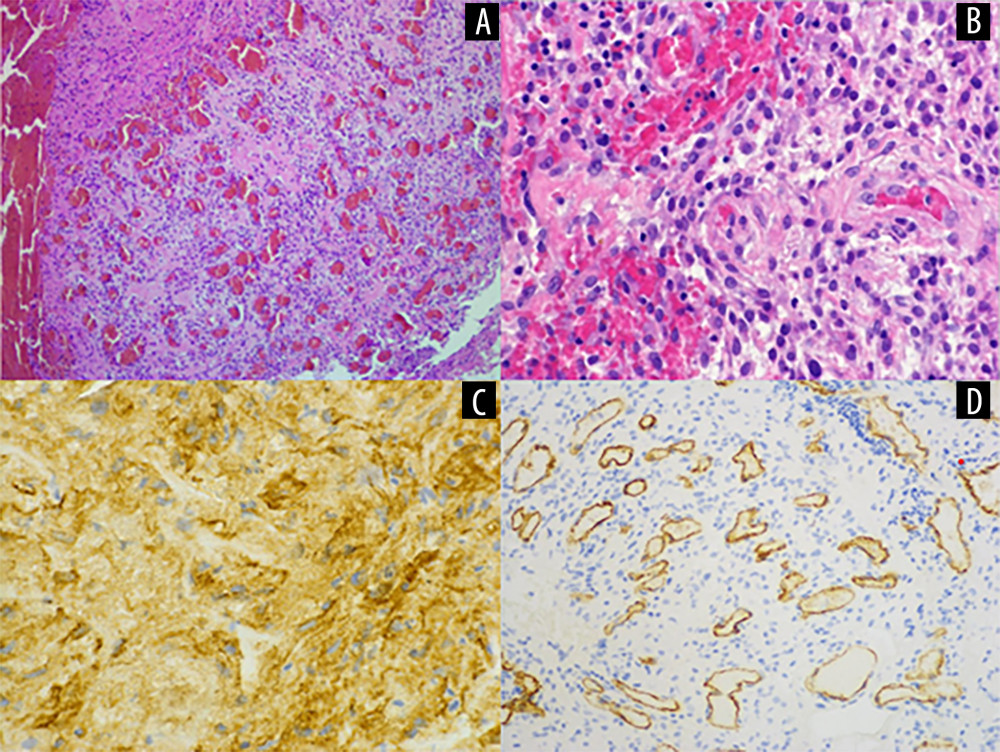 Figure 3. Multiple blood vessels of small calibre in the tumor with focal blood effusions, hematoxylin-eosin stain, original magnification (OM) 100× (A). Angiomatous meningioma (CNS WHO grade 1), hyalinization of blood vessel wall, enffusion of erihrocytes, OM 400× (B). Eepithelial membanous antigen-positive expression in angiomatous meningioma (WHO grade 1), OM 400× (C). CD34 expression in blood vessels in angiomatous meningioma, WHO grade 1, OM 400× (D).
Figure 3. Multiple blood vessels of small calibre in the tumor with focal blood effusions, hematoxylin-eosin stain, original magnification (OM) 100× (A). Angiomatous meningioma (CNS WHO grade 1), hyalinization of blood vessel wall, enffusion of erihrocytes, OM 400× (B). Eepithelial membanous antigen-positive expression in angiomatous meningioma (WHO grade 1), OM 400× (C). CD34 expression in blood vessels in angiomatous meningioma, WHO grade 1, OM 400× (D). 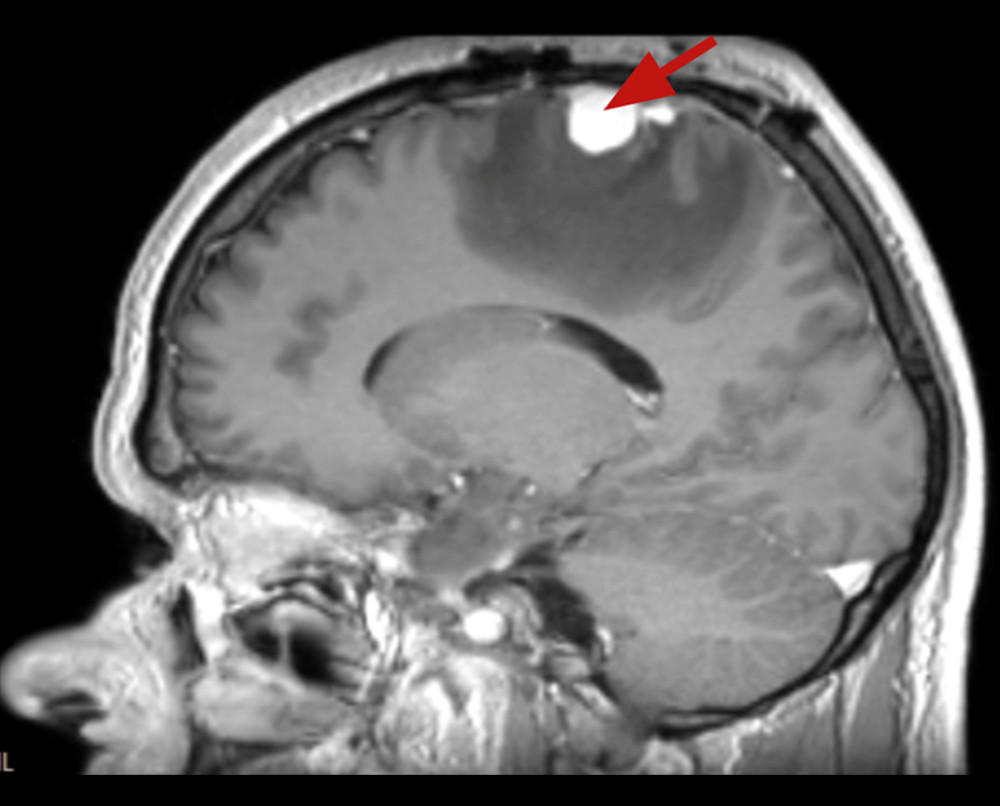 Figure 4. The brain MRI 6 months after the surgery sequence T1 in the sagittal plane with contrast injection. In the right parietal lobe, at the site of excision, an irregularly shaped lesion 2.4×2.0×1.4 cm in antero-posterior×latero-lateral×cranio-caudal directions. Tissues of the lesion steadily and intensely accumulated contrast.
Figure 4. The brain MRI 6 months after the surgery sequence T1 in the sagittal plane with contrast injection. In the right parietal lobe, at the site of excision, an irregularly shaped lesion 2.4×2.0×1.4 cm in antero-posterior×latero-lateral×cranio-caudal directions. Tissues of the lesion steadily and intensely accumulated contrast. 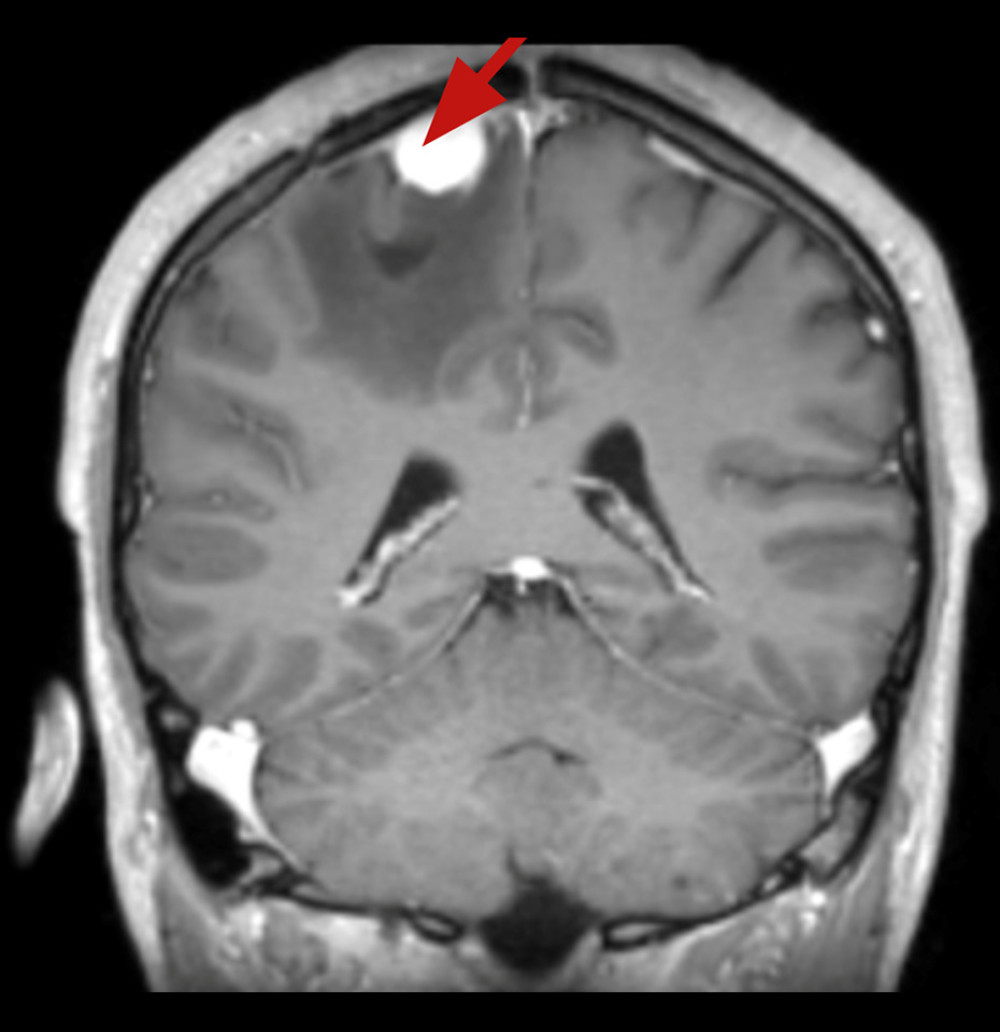 Figure 5. The brain MRI 6 months after the surgery sequence T1 in the coronal plane with contrast injection. Recurrence of a convexity tumor above the right parietal lobe: atypical meningioma is suspected
Figure 5. The brain MRI 6 months after the surgery sequence T1 in the coronal plane with contrast injection. Recurrence of a convexity tumor above the right parietal lobe: atypical meningioma is suspected 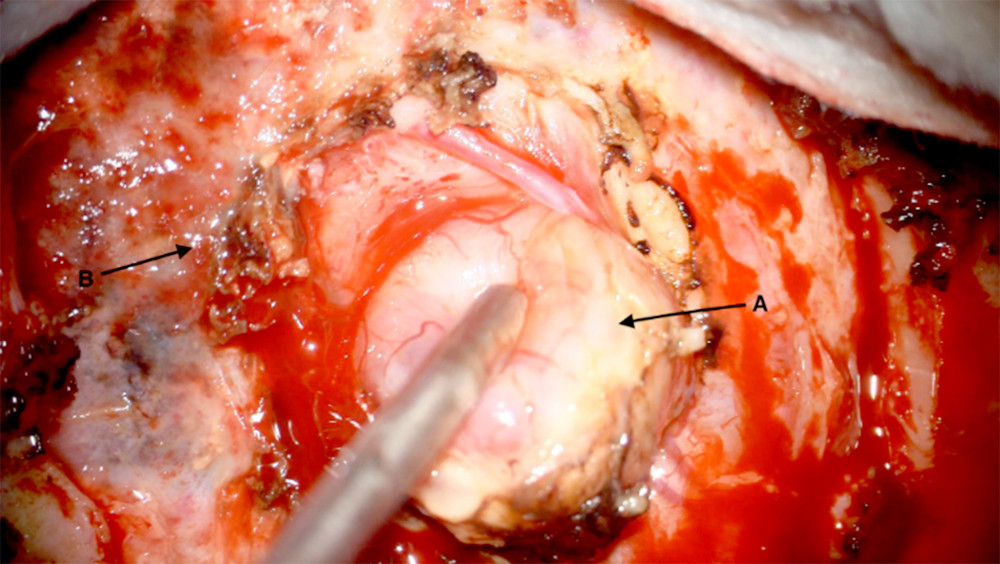 Figure 6. Surgical area in right temporal region, resection of a recurrent tumor (A), dura mater of the brain (B).
Figure 6. Surgical area in right temporal region, resection of a recurrent tumor (A), dura mater of the brain (B).  Figure 7. Surgical area after tumor evacuation. The tumor was completely evacuated at the site of the operation.
Figure 7. Surgical area after tumor evacuation. The tumor was completely evacuated at the site of the operation. 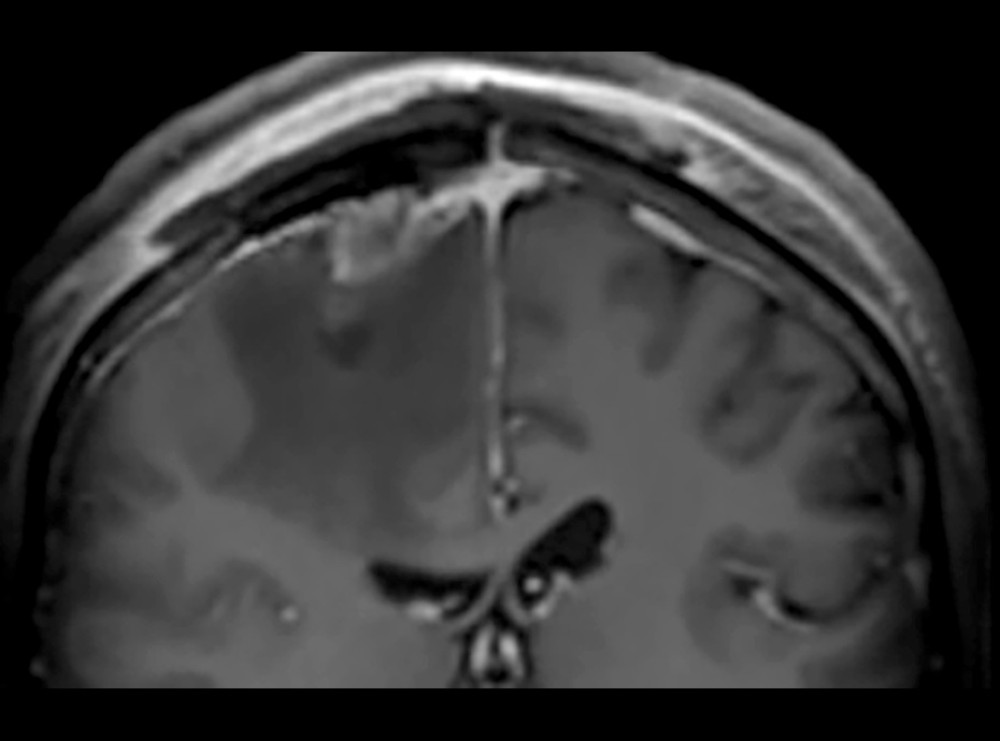 Figure 8. An MRI of the head sequence T1 in the coronal plane following osteoplastic recraniotomy and removal of the tumor, zoomed in. Blood products were observed in the surgical site, with no signs of remaining tumor tissue. Extensive perifocal edema was noted.
Figure 8. An MRI of the head sequence T1 in the coronal plane following osteoplastic recraniotomy and removal of the tumor, zoomed in. Blood products were observed in the surgical site, with no signs of remaining tumor tissue. Extensive perifocal edema was noted. 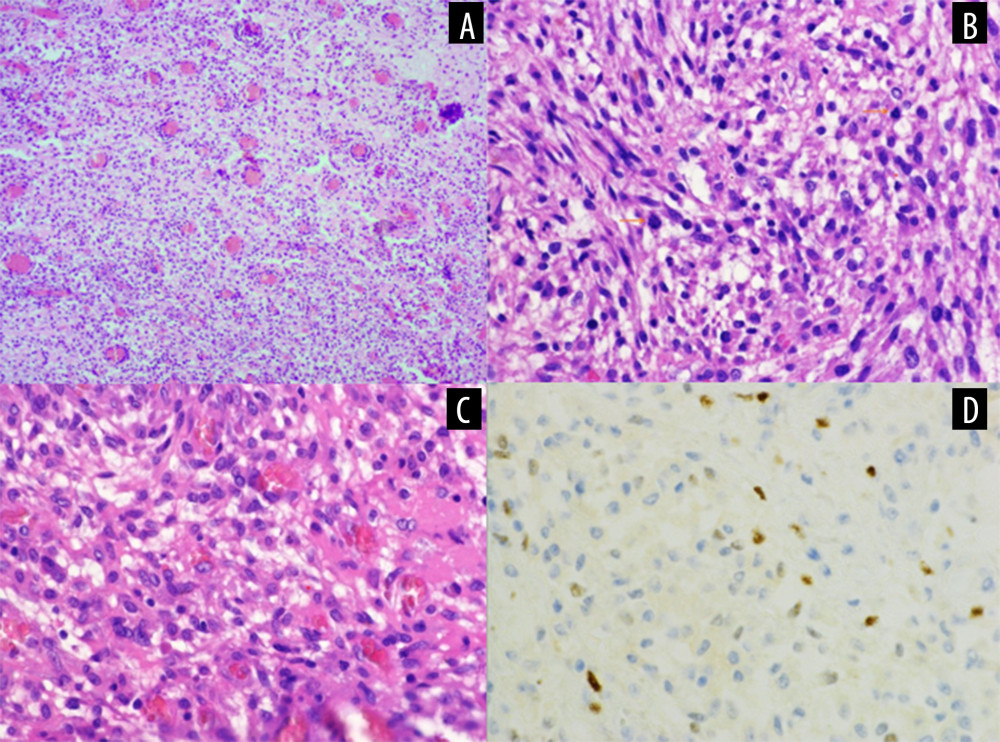 Figure 9. Atypical angiomatous meningioma (CNS WHO grade 2), with notably increased cellularity, original magnification (OM) 100× (A). Atypical angiomatous meningioma (WHO grade 2), note presence of mitotic figures (arrows) and increased tumor cellularity, OM 400× (B). Atypical angiomatous meningioma (WHO grade 2), note spindle shaped tumor cells, with overall increased tumor cellularity, and vascular network, OM 400× (C). Progesterone expression in atypical angiomatous meningioma (WHO grade 2), OM 400× (D).
Figure 9. Atypical angiomatous meningioma (CNS WHO grade 2), with notably increased cellularity, original magnification (OM) 100× (A). Atypical angiomatous meningioma (WHO grade 2), note presence of mitotic figures (arrows) and increased tumor cellularity, OM 400× (B). Atypical angiomatous meningioma (WHO grade 2), note spindle shaped tumor cells, with overall increased tumor cellularity, and vascular network, OM 400× (C). Progesterone expression in atypical angiomatous meningioma (WHO grade 2), OM 400× (D). References
1. Wiemels J, Wrensch M, Claus EB, Epidemiology and etiology of meningioma: J Neurooncol, 2010; 99(3); 307-14
2. Liu Z, Wang C, Wang H, Clinical characteristics and treatment of angiomatous meningiomas: A report of 27 cases: Int J Clin Exp Pathol, 2013; 6(4); 695-702
3. Hasselblatt M, Nolte KW, Paulus W, Angiomatous meningioma: A clinicopathologic study of 38 cases: Am J Surg Pathol, 2004; 28(3); 390-93
4. Torp SH, Solheim O, Skjulsvik AJ, The WHO 2021 Classification of Central Nervous System tumours: A practical update on what neurosurgeons need to know – a minireview: Acta Neurochir (Wien), 2022; 164(9); 2453-64
5. Louis DN, Perry A, Wesseling P, The 2021 WHO Classification of Tumors of the Central Nervous System: A summary: Neuro Oncol, 2021; 23(8); 1231-51
6. Yarabarla V, Mylarapu A, Han TJ, Intracranial meningiomas: An update of the 2021 World Health Organization classifications and review of management with a focus on radiation therapy: Front Oncol, 2023; 13; 1137849
7. Zhang T, Yu JM, Wang YQ, WHO grade I meningioma subtypes: MRI features and pathological analysis: Life Sci, 2018; 213; 50-56
8. Azizyan A, Eboli P, Drazin D, Differentiation of benign angiomatous and microcystic meningiomas with extensive peritumoral edema from high grade meningiomas with aid of diffusion weighted MRI: Biomed Res Int, 2014; 2014; 650939
9. Hwang J, Kong DS, Seol HJ, Clinical and radiological characteristics of angiomatous meningiomas: Brain Tumor Res Treat, 2016; 4(2); 94-99
10. An HY, Yu IK, Kim MS, Angiomatous meningioma: CT and MR imaging features: J Korean Soc Radiol, 2011; 64(5); 429-34
11. Yang T, Wu L, Yang C, Xu Y, Epidural angiomatous meningioma of the thoracic spine: A case report: Oncol Lett, 2016; 11(1); 458-60
12. Shen Y, Liu X, Yang W, Angiomatous meningioma with bizarre nuclei: A case report: Mol Clin Oncol, 2023; 18(6); 46
13. Goldbrunner R, Stavrinou P, Jenkinson MD, EANO guideline on the diagnosis and management of meningiomas: Neuro Oncol, 2021; 23(11); 1821-34
14. International Agency for Research on Cancer: WHO Classification of Tumours [Internet], Lyon, World Health Organization [cited 2025 Mar 25]. Available from: https://tumourclassification.iarc.who.int
15. Marciscano AE, Stemmer-Rachamimov AO, Niemierko A, Benign meningiomas (WHO Grade I) with atypical histological features: Correlation of histopathological features with clinical outcomes: J Neurosurg, 2016; 124(1); 106-14
16. Dullea JT, Vasan V, Rutland JW, Association between tumor mutations and meningioma recurrence in Grade I/II disease: Oncoscience, 2022; 9; 70-81
Figures
Figure 1. The head native CT with reconstructions in the coronal plane (A) and sagittal plane (B) zoomed in. In the right hemisphere of the brain an irregularly shaped lesion around 2.8 cm. Areas of heterogeneous hypodense edema around the lesion.Figure 2. The brain MRI sequence T1 after contrast injection in the coronal plane (A) and sagittal plane (B). On the convex surface of the parietal lobe of the right hemisphere is about 2.5×1.6 cm homogeneous lesion. Accumulation of the contrast is consistent and intensive.Figure 3. Multiple blood vessels of small calibre in the tumor with focal blood effusions, hematoxylin-eosin stain, original magnification (OM) 100× (A). Angiomatous meningioma (CNS WHO grade 1), hyalinization of blood vessel wall, enffusion of erihrocytes, OM 400× (B). Eepithelial membanous antigen-positive expression in angiomatous meningioma (WHO grade 1), OM 400× (C). CD34 expression in blood vessels in angiomatous meningioma, WHO grade 1, OM 400× (D).Figure 4. The brain MRI 6 months after the surgery sequence T1 in the sagittal plane with contrast injection. In the right parietal lobe, at the site of excision, an irregularly shaped lesion 2.4×2.0×1.4 cm in antero-posterior×latero-lateral×cranio-caudal directions. Tissues of the lesion steadily and intensely accumulated contrast.Figure 5. The brain MRI 6 months after the surgery sequence T1 in the coronal plane with contrast injection. Recurrence of a convexity tumor above the right parietal lobe: atypical meningioma is suspectedFigure 6. Surgical area in right temporal region, resection of a recurrent tumor (A), dura mater of the brain (B).Figure 7. Surgical area after tumor evacuation. The tumor was completely evacuated at the site of the operation.Figure 8. An MRI of the head sequence T1 in the coronal plane following osteoplastic recraniotomy and removal of the tumor, zoomed in. Blood products were observed in the surgical site, with no signs of remaining tumor tissue. Extensive perifocal edema was noted.Figure 9. Atypical angiomatous meningioma (CNS WHO grade 2), with notably increased cellularity, original magnification (OM) 100× (A). Atypical angiomatous meningioma (WHO grade 2), note presence of mitotic figures (arrows) and increased tumor cellularity, OM 400× (B). Atypical angiomatous meningioma (WHO grade 2), note spindle shaped tumor cells, with overall increased tumor cellularity, and vascular network, OM 400× (C). Progesterone expression in atypical angiomatous meningioma (WHO grade 2), OM 400× (D). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133