21 July 2025: Articles 
Diagnosing Disseminated Peritoneal Leiomyomatosis: Malignancy-Like Presentation in a 59-Year-Old Woman
Challenging differential diagnosis, Rare disease
Changchao Xiao BEF 1, Haixing Ju BE 2*, Jun Cao BE 3DOI: 10.12659/AJCR.947246
Am J Case Rep 2025; 26:e947246






Abstract
BACKGROUND: Disseminated peritoneal leiomyomatosis (DPL), or leiomyomatosis peritoneal disseminata, is a benign condition that presents with multiple lower abdominal peritoneal nodules consisting of smooth muscle cells, which can slowly increase in size. The risk of malignant transformation is 2% to 5%. The mechanisms underlying the pathogenesis and malignancy of DPL are unclear and can be associated with a variety of factors. This report describes a 59-year-old woman presenting with multiple abdominal masses and a diagnosis of DPL.
CASE REPORT: This report describes a 59-year-old female patient who experienced abdominal pain and difficulty defecating. Proctoscopy showed intestinal stenosis and inflammatory changes. She may have had renal dysfunction. The medical history showed that the patient had uterine fibroids in the past and had undergone hysterectomy surgery. We cannot confirm whether the patient received hormone therapy before admission. Based on the results of histopathology and immunohistochemistry, it was considered to be a DPL. The patient died 6 months after surgery.
CONCLUSIONS: DPL is a rare disease that is difficult to diagnose and traditionally considered a benign condition. This report emphasizes the importance of understanding the presentation and distribution of DPL, as it can mimic the deposition of malignant tumors. This case also emphasizes the importance of diagnosing benign tumors through histopathology. The mechanism of malignant transformation of DPL is currently unclear, and it is of great significance to combine multiple detection methods in clinical practice to determine its malignancy.
Keywords: Diagnosis, Malignant Carcinoid Syndrome, Pathology, Humans, Female, Middle Aged, Leiomyomatosis, Peritoneal Neoplasms, Fatal Outcome, Diagnosis, Differential, Hysterectomy
Introduction
Disseminated peritoneal leiomyomatosis (DPL) is a rare benign disease, often giving the appearance of metastatic ovarian or peritoneal carcinoma. The risk of malignant transformation is 2% to 5%. Diagnostic methods include computed tomography (CT), ultrasound, magnetic resonance imaging (MRI), and histopathological evaluation, which are essential for assessing disease extent and guiding treatment. Management strategies encompass surgical intervention, with a focus on minimizing iatrogenic risks, conservative approaches for asymptomatic patients, and advancements in hormonal treatments [1,2]. In 1952, the case of multiple peritoneal leiomyomas was initially documented by Wilson and Peale [3]. The prevalence of DPL is estimated to be less than 1 in every 10 million individuals, with approximately 200 reported cases documented in the existing literature [4]. The cause of the disease is unclear, and several theories have been proposed for DPL, including hormonal stimulation, iatrogenic factors, and genetic predispositions. DPL typically occurs in premenopausal women and is traditionally considered a benign condition [5]. Therefore, the risk of malignant transformation is extremely low. There have been a limited number of cases reporting malignant transformation of DPL in previous literature [6–11]. Little is understood about the pathogenesis or potential for malignant transformation of this condition. In this report, we present a case of DPL in a middle-aged female patient. Additionally, we conducted a literature review to analyze the clinical features, diagnosis, and pathogenesis of malignant transformation.
Case Report
A 59-year-old woman presented to our hospital with difficulty in defecation. The patient had been experiencing tenesmus and persistent vague abdominal pain for the previous 6 months. At presentation, the patient had experienced more pronounced persistent abdominal pain than before, especially after meals. The patient had a blood creatinine level of 1255 umol/L, suggesting that she may have had renal dysfunction. Due to her previous clinical presentation of hydronephrosis, she underwent bilateral ureteral stent implantation 12 days before presenting at our hospital. Medical history revealed that she had had uterine myomas confirmed by ultrasound and MRI, and had undergone a hysterectomy.
She did not have any previous history of cancer or other relevant medical conditions. Colonoscopy examination revealed a 10-cm stenosis at the entrance to the large intestine, with obvious mucosal congestion, stiffness, and disordered glandular structures occupying more than half of the abdominal cavity, and the endoscope could not pass through the lesion. Lower abdominal MRI revealed significant thickening of the bowel wall at the junction of the rectum and sigmoid colon and a mass high-density shadow at the left pelvic cavity (Figure 1). Positron emission tomography-CT (PET-CT) showed thickening of the rectum and sigmoid colon wall, with increased fludeoxyglucose (FDG) metabolism. The cells inside the lesion under the microscope were well-differentiated smooth muscle cells (Figure 2). However, other pathological studies found a small number of abnormal glandular cells and severe inflammatory changes in the rectal mucosal tissue. Additionally, there was an increase in FDG metabolism observed in the greater omentum, mesentery, cervix uteri, and left ischial area. The tumor marker test demonstrated elevated serum CA19-9 (79.49 U/mL; range <37), CA 50 (52.8 IU/mL; range <25), and CA 242 (57.9 IU/mL; range <20) levels. The CA125 was negative (13.67 U/mL, range <35). The immunohistochemical findings were CD117(−), DOG1(−), Des(+), SMA(+), Ki-67 (index 5%), S-100(−), h-cadesmon(+), Vim(+), SOX10(−), HMB45(−), Melan-A(−), ALK(D5F3) (−), ER(−), PR(−), ROS1(−), CK20(−), CDX-2(−), and SATB2(−). The diagnosis of DPL was considered in conjunction with her history and immunohistochemistry results; the patient had undergone surgery at another hospital. By 6 months after surgery, the patient had died.
Discussion
In this case, we believe that the etiology of DPL may have been related to various factors, such as changes in hormone levels and surgery. Although cases of malignant transformation are rare, they require adequate attention and more aggressive interventions in clinical practice. Most patients with DPL are asymptomatic, while a minority experience symptoms such as abdominal pain, abdominal distension, abnormal uterine bleeding, and even gastrointestinal manifestations [12,13]. Our patient had significant abdominal symptoms, and a proctoscopy revealed intestinal narrowing and inflammatory changes. Pathological examination showed a small number of abnormal glandular cells in the mucosa, which had not been documented in previous reports [14–16]. No specific serological markers had been found. The patient’s tumor marker test revealed elevated concentrations of CA19-9, CA 50, and CA 242; however, tumor markers were previously reported at normal levels in a similar case [17]. The underlying reasons for these increased values remain unknown. The tumors observed in previous cases of DPL with PET-CT scans showed mild to moderate affinity for FDG (SUVmax: 1.6–4.3) [18,19]. This can easily be confused with malignant tumors. A previously reported case of a 43-year-old woman who initially presented with right lower abdominal pain revealed the patient’s CT and MRI examinations showed multiple intraperitoneal soft tissue masses near the sigmoid mesentery, left accessory colon sulcus, and ascending colon. With the combination of peritoneal mass resection surgery, abdominal hysterectomy, and bilateral salpingectomy, the diagnosis of DPL was confirmed [20]. In addition, the case of a 41-year-old female patient with a history of laparoscopic myomectomy and pregnancy was reported. Multiple lumps were found in the patient’s abdomen, with no tenderness or other discomfort. Based on imaging examination and clinical manifestations, the preliminary diagnosis was gastrointestinal stromal tumor. However, pathological examination after surgery confirmed that it was DPL. The patient’s postoperative prognosis was good, and there was no recurrence during the follow-up period [4]. The clinical outcome for DPL is generally good; however, a study suggests that malignant transformation can occur in 2% to 5% of cases [21]. Only a limited number of reported cases have demonstrated DPL with malignant transformation, while the pathogenesis of this transformation remains unclear. Yamaguchi et al discovered a potential correlation between p53 overexpression and the development of malignancy [11]. Chiu et al suspect that epithelial-mesenchymal transition is a key process in malignant metastasis of DPL [17]. Currently, surgery is the mainstay of treatment. However, due to the rarity of DPL, there are no guidelines on the management of the disease; therefore, it is important to consider the unique circumstances of each patient when determining appropriate treatments. In some of the similar cases we presented earlier [4,20], the patients had a good prognosis without deterioration or recurrent metastasis, whereas the patient in this case had a very poor prognosis and a short overall survival after surgery. This case should cause clinicians to be more cautious about the diagnosis of patients with DPL, and to consider whether a more comprehensive examination is needed to confirm that there is no possibility of deterioration. Postoperative surveillance plays a crucial role in preventing malignant transformation.
Conclusions
In conclusion, this case demonstrates diagnostic challenges. The patient had previous clinical manifestations of hydronephrosis and had persistent non-specific gastrointestinal symptoms in the past 6 months, coupled with the uncertainty of imaging examinations, highlighting the possibility of misdiagnosis. This report emphasizes the importance of understanding the presentation and distribution of DPL, as it can mimic the deposition of malignant tumors. In clinical practice, it is necessary to integrate multiple detection methods, to confirm the benign or malignant nature of tumors.
Figures
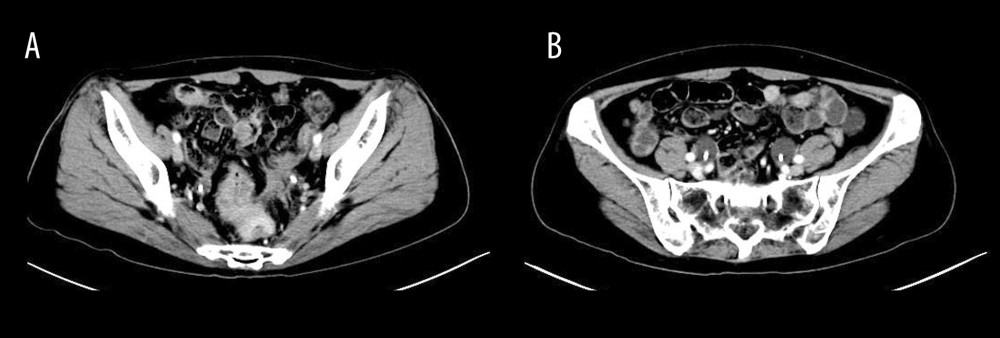 Figure 1. Magnetic resonance imaging of the lower abdomen showing several masses in the abdomen and pelvis.
Figure 1. Magnetic resonance imaging of the lower abdomen showing several masses in the abdomen and pelvis. 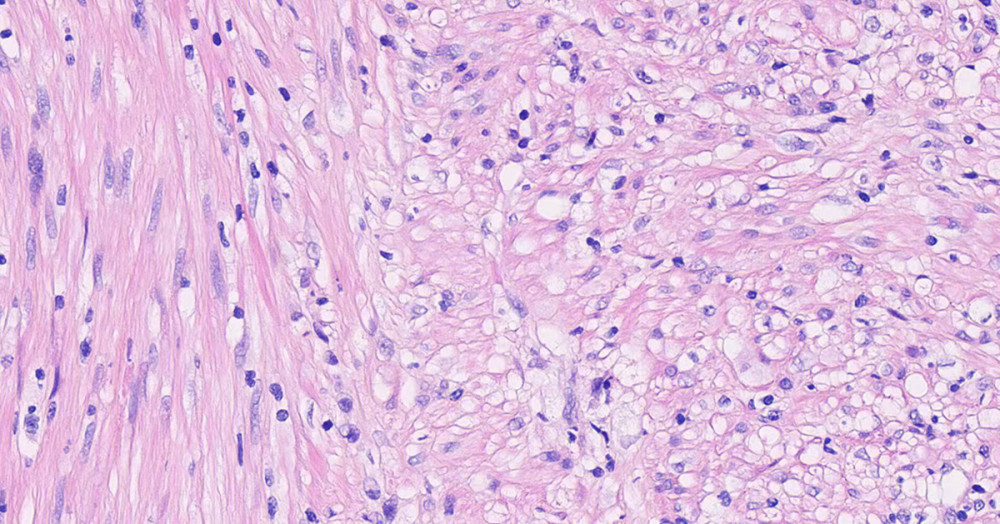 Figure 2. A photomicrograph of the histopathology of a peritoneal nodule in a 59-year-old woman presenting with disseminated peritoneal leiomyomatosis. Image shows well-differentiated smooth muscle cells in a cross-bundle, woven arrangement with long, bluntly rounded nuclei, no obvious cellular anisotropy, no or few nuclear schizophrenic images, and no necrosis, interstitial fibrosis, or vitreous degeneration. Hematoxylin and eosin staining, magnification ×60.
Figure 2. A photomicrograph of the histopathology of a peritoneal nodule in a 59-year-old woman presenting with disseminated peritoneal leiomyomatosis. Image shows well-differentiated smooth muscle cells in a cross-bundle, woven arrangement with long, bluntly rounded nuclei, no obvious cellular anisotropy, no or few nuclear schizophrenic images, and no necrosis, interstitial fibrosis, or vitreous degeneration. Hematoxylin and eosin staining, magnification ×60. References
1. Soni S, Pareek P, Narayan S, Disseminated peritoneal leiomyomatosis: An unusual presentation of intra-abdominal lesion mimicking disseminated malignancy: Med Pharm Rep, 2020; 93(1); 113-16
2. Bucuri CE, Ciortea R, Malutan AM, Disseminated peritoneal leiomyomatosis – a challenging diagnosis-mimicking malignancy scoping review of the last 14 years: Biomedicines, 2024; 12(8); 1749
3. Thang NM, Thien DH, Huyen , Leiomyomatosis peritonealis dissemianata five years after laparoscopic uterine myomectomy: A case report: Ann Med Surg (Lond), 2021; 66; 102377
4. Liu X, Hu Y, Chen L, Zhou Q, Disseminated peritoneal leiomyomatosis: A case report and review of the literature: J Int Med Res, 2021; 49(8); 3000605211033194
5. Morgan ED, Kahiye M, Kule I, Disseminated peritoneal leiomyomatosis as an incidental finding: A case report: Clin Case Rep, 2022; 10(3); e05541
6. Shaukat I, Yassin S, Paudel A, Unusual presentation of parasitic leiomyoma; A tale of twists and turns: J Community Hosp Intern Med Perspect, 2019; 9(2); 168-70
7. Żyła MM, Dzieniecka M, Kostrzewa M, Leiomyomatosis peritonealis disseminata of unusual course with malignant transformation: Case report: Acta Obstet Gynecol Scand, 2015; 94(2); 220-23
8. Wen CY, Lee HS, Lin JT, Yu CC, Disseminated peritoneal leiomyomatosis with malignant transformation involving right ureter: A case report: World J Clin Cases, 2022; 10(5); 1639-44
9. Sharma P, Chaturvedi KU, Gupta R, Nigam S, Leiomyomatosis peritonealis disseminata with malignant change in a post-menopausal woman: Gynecol Oncol, 2004; 95(3); 742-45
10. Syed M, Parida B, Mankeshwar T, Patil A, Imaging findings in a rare case of leiomyomatosis peritonealis disseminata with malignant transformation: Pol J Radiol, 2017; 82; 426-30
11. Barone A, Ambrosio MR, Rocca BJ, Leiomyomatosis peritonealis disseminata: An additional case: Eur J Gynaecol Oncol, 2014; 35(2); 188-91
12. Izi Z, Outznit M, Cherraqi A, Tbouda M, Disseminated peritoneal leiomyomatosis: A case report: Radiol Case Rep, 2023; 18(6); 2237-40
13. Lee M, Morey G, Lopez H, Bass R, Ferra S, Disseminated peritoneal leiomyomatosis mimicking carcinomatosis: A case report: Int J Surg Case Rep, 2024; 120; 109908
14. La Greca G, Colarossi C, Di Mattia P, Endomyometriosis of the rectum with disseminated peritoneal leiomyomatosis 8 years after laparoscopic myomectomy: A case report: Front Surg, 2021; 8; 666147
15. Huang SF, Wen CY, Liao CI, Leiomyomatosis peritonealis disseminata mimicking peritoneal carcinomatosis 13 years after laparoscopic uterine myomectomy: A case report: Int J Surg Case Rep, 2021; 81; 105745
16. Bayrak S, Pasaoglu E, Cakar E, Disseminated peritoneal leiomyomatosis with chronic constipation: A case report: J Med Case Rep, 2014; 8; 114
17. Chiu HC, Wu MY, Li CH, Epithelial-mesenchymal transition with malignant transformation leading multiple metastasis from disseminated peritoneal leiomyomatosis: J Clin Med, 2018; 7(8); 207
18. Talebian Yazdi A, De Smet K, Antic M, Leiomyomatosis peritonealis disseminata in a 50-year-old woman: imaging findings: JBR-BTR, 2010; 93(4); 193-95
19. Khoo ACH, Lim SY, 18F-fluorodeoxyglucose positron emission tomography-computed tomography imaging of leiomyomatosis peritonealis disseminata: World J Nucl Med, 2021; 20(3); 322-23
20. Hiremath SB, Benjamin G, Gautam AA, Disseminated peritoneal leiomyomatosis: A rare cause of enigmatic peritoneal masses: BJR Case Rep, 2016; 2(3); 20150252
21. Surmacki P, Sporny S, Tosiak A, Lasota J, Disseminated peritoneal leiomyomatosis coexisting with leiomyoma of the uterine body: Arch Gynecol Obstet, 2006; 273(5); 301-3
Figures
Figure 1. Magnetic resonance imaging of the lower abdomen showing several masses in the abdomen and pelvis.Figure 2. A photomicrograph of the histopathology of a peritoneal nodule in a 59-year-old woman presenting with disseminated peritoneal leiomyomatosis. Image shows well-differentiated smooth muscle cells in a cross-bundle, woven arrangement with long, bluntly rounded nuclei, no obvious cellular anisotropy, no or few nuclear schizophrenic images, and no necrosis, interstitial fibrosis, or vitreous degeneration. Hematoxylin and eosin staining, magnification ×60. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133