12 June 2025: Articles 
Spontaneous Coronary Artery Dissection in a Young Man: A Case Report and Literature Review
Rare disease
Ashot Batikyan BCDEF 1*, Pavel Abalyan CEF 2, Hakob Harutyunyan DEF 3, Aleksan Khachatryan DF 4, Vahagn Tamazyan DE 3, Pawel BorkowskiDOI: 10.12659/AJCR.947717
Am J Case Rep 2025; 26:e947717






Abstract
BACKGROUND: Spontaneous coronary artery dissection is a rare and underdiagnosed cause of acute coronary syndrome, primarily affecting women. The occurrence of spontaneous coronary artery dissection in the context of the absence of traditional atherosclerotic risk factors raises questions about the role of physical exertion or other stressors as potential triggers. Early recognition through clinical assessment and imaging is essential, as the therapeutic approach for spontaneous coronary artery dissection differs significantly from the treatment of traditional atherosclerotic acute coronary syndrome. Conservative management is often preferred for hemodynamically stable patients because interventional procedures have increased prevalence of complications in these patients.
CASE REPORT: This case report highlights an uncommon presentation of spontaneous coronary artery dissection in a 28-year-old man who presented with non-ST-elevation myocardial infarction following physical exertion. The diagnosis of spontaneous coronary artery dissection was confirmed via coronary angiography, revealing the classic findings of dissection without significant atherosclerosis. Management was conservative, as the patient was hemodynamically stable, with close monitoring and medical therapy, including antiplatelet agents and beta-blockers.
CONCLUSIONS: This case challenges the prevailing gender assumptions associated with spontaneous coronary artery dissection and highlights the need for increased awareness of spontaneous coronary artery dissection in males. Additionally, it suggests the potential role of physical stressors in precipitating spontaneous coronary artery dissection. Further research into the pathophysiology of spontaneous coronary artery dissection in different populations is warranted.
Keywords: acute coronary syndrome, Cardiovascular Diseases, Coronary Angiography, Coronary Artery Disease, Dissection, Blood Vessel, Myocardial Infarction, Humans, Male, adult, Coronary Vessel Anomalies, Vascular Diseases
Introduction
Spontaneous coronary artery dissection (SCAD) is a rare condition characterized by dissection of a coronary artery that is neither iatrogenic nor associated with atherosclerosis or trauma [1,2]. Despite advancements in diagnostic techniques, SCAD often remains underdiagnosed. The initial report of SCAD was published in the British Medical Journal in 1931. The case involved a 42-year-old woman who experienced severe chest pain and died unexpectedly. An autopsy revealed a rupture of the dissecting right coronary artery as the cause of death [3]. Although SCAD typically affects females and is rare in males, we report a case of SCAD presenting as non-ST-elevation myocardial infarction (NSTEMI) in a 28-year-old man.
Case Report
A 28-year-old man with past medical history of gastroesophageal reflux disease presented with left-sided and substernal chest pain for 4 hours. The pain was constant, burning in quality, 7/10 in intensity, radiating to the left arm, associated with shortness of breath and diaphoresis, with no alleviating or aggravating factors. He started to have chest pain after feeling nauseous and vomiting while playing basketball indoors. He took aluminum hydroxide, magnesium hydroxide, and famotidine, with minimal relief of the pain. He had never felt similar pain before. He also reported lifting heavy weights before playing basketball. He denied any palpitations, dizziness, recent illnesses, or personal or family history of heart disease. He reported smoking marijuana daily and denied tobacco, alcohol, or drug use.
On presentation, he was in severe distress with hypertension of 150/100 and tachypnea of 27, heart rate was 74, and oxygen saturation was 100% on room air. Physical examination was unremarkable. He was given aspirin 162 mg and a nitroglycerin sublingual tablet, without alleviation of the chest pain. Subsequently, morphine was given, resulting in complete relief of the pain.
EKG on presentation revealed peaked T waves in V2–V4 (Figure 1). Troponin was mildly elevated at 0.156 (reference range: 0–0.09 ug/L) (Figure 2). Other laboratory tests on presentation are depicted in Table 1. Computed tomography angiography of the chest ruled out dissection of the thoracic aorta, pulmonary embolism, or any other pulmonary pathology.
A repeat EKG a few hours later showed T wave inversion in V3–V4 and J point elevation in V1–V2 (Figure 3). The repeat troponin test showed dynamic elevation from 0.156 to 0.548. The patient was completely pain-free. He was started on aspirin, ticagrelor, and heparin drip for NSTEMI.
With increasing troponin and dynamic EKG changes, together with transthoracic echocardiography showing regional wall motion abnormalities in the left anterior descending artery territory (Video 1), the patient was sent for urgent left heart catheterization which was suggestive of coronary artery dissection in the mid left anterior descending artery with superimposed thrombus and embolized thrombus to the apical vessel, in the left dominant system (Figure 4, Video 2). Coronary intravascular ultrasound confirmed the dissection by showing intramural hematoma and dissection flap.
The patient subsequently was started on double antiplatelet therapy (aspirin and clopidogrel), continued on a heparin drip due to thrombus, and was started on a low-dose beta-blocker. Administration of glycoprotein IIb/IIIa inhibitors was deferred in accordance with institutional guidelines. Troponin reached a plateau and the patient continued to deny any chest pain. Head-to-pelvis imaging was pursued to look for any extra-coronary vascular abnormalities. Magnetic resonance imaging and magnetic resonance angiography of the brain as well as magnetic resonance angiography of the neck did not reveal any intracranial or extracranial vascular abnormality. The renal artery duplex scan was negative for any hemodynamically significant lesion or stenosis in the renal arteries. The patient was strongly advised to avoid strenuous exercise and weight lifting as well as to quit smoking marijuana.
Discussion
DEFINITION:
SCAD is characterized by the formation of an intramural hematoma, which occurs between the layers of the coronary artery wall, such as intima, media, and adventitia, resulting in the creation of a false lumen that is neither caused by medical intervention nor linked to atherosclerosis or injury [1,2].
EPIDEMIOLOGY:
The exact incidence and prevalence of SCAD remain unclear due to this condition being frequently underdiagnosed. It was thought to be a rare condition, but with the recent increase in awareness among physicians and enhanced diagnostic capabilities the incidence of SCAD has increased [4]. SCAD has been identified to be a cause of acute coronary syndrome (ACS) in up to 4% of cases [5–8] and is associated with up to 35% of myocardial infarction in females below the age of 50 [9].
Multiple studies showed a female predominance of up to 94% across the world [6,9–12], except in the Persian Gulf region, where it was reported that only 50% of patients with SCAD were female, but likely because of misdiagnosed or underdiagnosed cases [13,14]. The higher prevalence of SCAD in females may be linked to underlying predisposing arteriopathies that are either specific to women or found more frequently among them. According to a few studies, men presenting with SCAD tend to be younger than females [15,16]. However, many females with prior myocardial infarctions may not have been accurately diagnosed with SCAD, which creates a possibility that the true mean age of women with SCAD is younger than reported [14].
PATHOPHYSIOLOGY:
The exact provoking event for SCAD is still uncertain, and 2 primary hypotheses have been suggested to elucidate the underlying pathophysiological mechanisms. The first one, known as the “inside-out” hypothesis, suggests that blood infiltrates the subintimal space from the true lumen following the endothelial-intimal disruption, leading to a false lumen and resultant compression stenosis. The second hypothesis, referred to as the “outside-in” hypothesis, posits that a hematoma forms independently within the media, potentially due to the rupture of microvessels, causing a secondary separation between the intima and media, ultimately resulting in tearing into the true lumen in some patients. The “inside-out” hypothesis is the predominant mechanism involved in dissections of non-coronary vascular distributions [17].
Most SCAD cases are likely caused by an outside-in mechanism, as there is typically no communication observed between the true and false lumens in most SCAD cases, and serial angiograms taken shortly after SCAD demonstrate that intramural hematoma usually occurs before the onset of intimal dissection [18]. Moreover, optical coherence tomography (OCT) imaging indicates that the fenestrations are the result of the false lumen rupturing into the true lumen, not the reverse [19]. Additionally, abnormalities in the adventitial vasa vasorum have been noted in SCAD patients, which may play a role in the development of intramural hematoma [20].
RISK FACTORS:
Men and women presenting with SCAD have similar cardiovascular risk factors, which is reasonable, as SCAD is not related to atherosclerosis [14]. Non-coronary vasculopathies, particularly fibromuscular dysplasia [21,22], as well as peripartum status [11,12,23] and connective tissue diseases (Marfan syndrome, vascular Ehlers-Danlos syndrome, and Loeys-Dietz syndrome [23,24]) have been linked to SCAD. Physical and emotional stress are common triggers for SCAD. In a study of 168 SCAD patients, 40% reported experiencing extreme emotional stress, while 24% reported strenuous physical activity before the onset of SCAD as precipitating factors [11]. Emotional stress was more commonly identified in women as a trigger for SCAD, while men more frequently reported strenuous physical activities such as isometric exercises or weightlifting as a trigger for SCAD [14,15,23].
CLINICAL PRESENTATION:
Individuals who have survived SCAD and undergo initial assessment nearly always exhibit ACS accompanied by elevated troponin levels: up to 87% of patients present with ST-elevation myocardial infarction (STEMI) and up to 69% with NSTEMI [9,11,12,25,26]. In the study by Mcalister et al, the proportion of SCAD patients presenting with STEMI, ventricular arrhythmia, or reduced ejection fraction was comparable between males and females [14].
In a cohort of 196 patients with SCAD, the most common presenting symptoms were chest pain (96%) radiating to the arm (52%), followed by nausea, vomiting, chest pain radiating to the neck, diaphoresis, dyspnea, back pain, dizziness, fatigue, headache, and syncope [27].
Ventricular arrhythmias or sudden cardiac death were reported on the presentation of SCAD in up to 11% of reported series. However, these findings must be considered carefully, as they exclude individuals who either did not survive to undergo initial evaluation or whose SCAD was unrecognized or misdiagnosed [2].
DIAGNOSIS:
Early identification of SCAD during the initial stages of ACS is critical since its management and diagnostic approaches differ from those used for atherosclerotic coronary artery disease. SCAD suspicion typically arises based on clinical presentation and patient demographics, such as younger age, female sex, and lack of traditional cardiovascular risk factors. Coronary angiography should be performed without delay, especially in cases of STEMI, as it remains the standard for diagnosing SCAD despite limitations in visualizing the arterial wall [2,28]. Another limitation could be the increased prevalence of iatrogenic catheter-induced coronary artery dissection (3.4% vs <0.2% in patients without SCAD), probably because SCAD patients have underlying coronary vascular fragility [29,30].
SCAD traditionally was characterized by the presence of multiple radiolucent lumens along with extraluminal contrast staining [31]. Nevertheless, this characteristic description has been identified in only a small fraction of SCAD patients. Based on the new classification system for SCAD angiography, type 1 SCAD corresponds to the classic appearance of multiple radiolucent lumens or contrast staining of the arterial wall, type 2 is indicative of the presence of diffuse stenosis that varies in severity and length (typically exceeding 20 mm), and type 3 is focal or tubular stenosis, typically less than 30 mm in length and resembles atherosclerosis. Type 2 SCAD is further classified into 2 subtypes: 2A involves diffuse arterial narrowing bordered by normal segments proximally and distally to the intramural hematoma, while 2B involves diffuse narrowing that extends to the distal end of the artery [29,32,33].
SCAD occurred more commonly in the LAD artery both in men and women in multiple studies, and men tend to experience more SCAD in the circumflex artery and less so in the right coronary artery compared to women. This difference may help explain why men with SCAD are less likely than women to present with ischemic changes [14].
According to several studies, type 2 coronary dissection is the most prevalent form, accounting for up to 68% of cases, followed by type 1 (29.1%) and type 3 (3.4%) [11]. A few studies have found that type 1 SCAD occurs more frequently in men compared to women [16,34], although the study by Mcalister et al did not reproduce it [14].
Other important diagnostic tools for SCAD are intravascular ultrasonography and optical coherence tomography. They should be utilized only when angiographic findings are indeterminate (eg, type 3 or ambiguous lesions) and the diameter of the artery is sufficiently large to accommodate the imaging catheter, given the associated risks, including the worsening of the dissection [2].
Coronary computed tomography angiography (CCTA) is another imaging method used to evaluate SCAD in patients without high-risk features on presentation. However, compared to conventional angiography, CCTA has inferior spatial resolution, and a normal CCTA result does not rule out the possibility of SCAD [35,36]. CCTA could serve as a valuable non-invasive approach for monitoring patients after diagnosis of SCAD, particularly to evaluate vessel healing in dissections involving proximal or large-diameter coronary arteries [37–39].
TREATMENT:
There are no distinct recommendations for the management of SCAD based on sex have been established [14]. Disrupted and fragile coronary vessel walls can make revascularization difficult. Therefore, a conservative strategy is typically favored when revascularization is not required, particularly in hemodynamically stable patients who have adequate distal flow in the dissected coronary artery and show no signs of ongoing ischemia [1,2,23]. However, conservatively managed patients do carry a risk of progression of dissection, especially in patients with isolated intramural hematoma within the first 6 days [18].
In high-risk patients experiencing ongoing ischemia, involvement of left main artery, or hemodynamic instability, conservative therapy may not be suitable. In these cases, percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) should be considered. CABG is indicated for clinically unstable patients with left main involvement, those who have had unsuccessful PCI, or those with persistent symptoms despite conservative management [2]. Despite the substantial initial technical success rate and positive short-term outcomes with CABG as a primary treatment approach, there is a notable occurrence of graft failure over the long term [23,40].
At present, the pharmacological management of SCAD is not guided by any randomized controlled trials. Patients who undergo PCI should be given the standard dual antiplatelet therapy (DAPT), as outlined in American Heart Association NSTEMI guidelines [41]. However, for patients managed conservatively with SCAD, there is no universal agreement on the optimal use or duration of aspirin alone or DAPT. One suggested approach involves initiating DAPT for at least 2 to 4 weeks followed by continuing low-dose aspirin alone for 3 to 12 months to cover the period during which SCAD healing typically occurs. Ultimately, the decision on longer-duration antiplatelet therapy should be made based on weighing the benefits and risks, including other comorbidities and bleeding complications [41]. While systemic anticoagulation with heparin can potentially decrease the amount of thrombus, it also carries the risk of enlarging the intramural hematoma. Consequently, it should not be routine practice in SCAD unless there is a visible intraluminal thrombus or other reasons for systemic anticoagulation [17,41].
Beta-blockers and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers should be given to patients with left ventricular systolic disfunction. Additionally, beta-blockers might have a protective effect on SCAD recurrence. Since a link between hyperlipidemia and SCAD has not been established, lipid-lowering therapy is typically only considered for patients with pre-existing hyperlipidemia or those whose overall risk profile necessitates treatment based on primary prevention guidelines [41].
PROGNOSIS:
After hospital discharge, adverse cardiovascular events are relatively common in patients with SCAD. Long-term outcomes indicate that major adverse cardiac events (MACE) occur in about 30% of patients within 2–3 years [9,11,42], and up to 37% at 5–7 years. Kaplan-Meier estimates suggest that the MACE rate could reach 50% within 10 years, with recurrent SCAD being the primary cause of these events [11,23,25]. In different series, SCAD recured in up to 19% of patients, with a median time of up to 3.6 years after the index SCAD event [9,23,43,44].
The study by Mcalister et al found that men were significantly less inclined to report chest pain at subsequent clinic visits, visit the emergency department for chest pain, or require hospital readmission for chest pain after hospital discharge. The chest pain experienced after SCAD is likely multifactorial, including non-ischemic origin and microvascular dysfunction, which is more common in women. Although men with SCAD experience chest pain less frequently, there is no definitive evidence indicating differences in the rates of recurrent myocardial infarction, SCAD, or MACE between men and women [14,45].
Conclusions
This case report and literature review highlight the importance of heightened awareness of SCAD as a differential diagnosis in males, particularly young, healthy individuals without atherosclerotic risk factors experiencing ACS after physical stress. Continued research into the underlying pathophysiology of SCAD, including hormonal and mechanical factors in different populations, is necessary to optimize prevention strategies. Additionally, SCAD patients should be closely monitored after discharge, given the risk for recurrence.
Figures
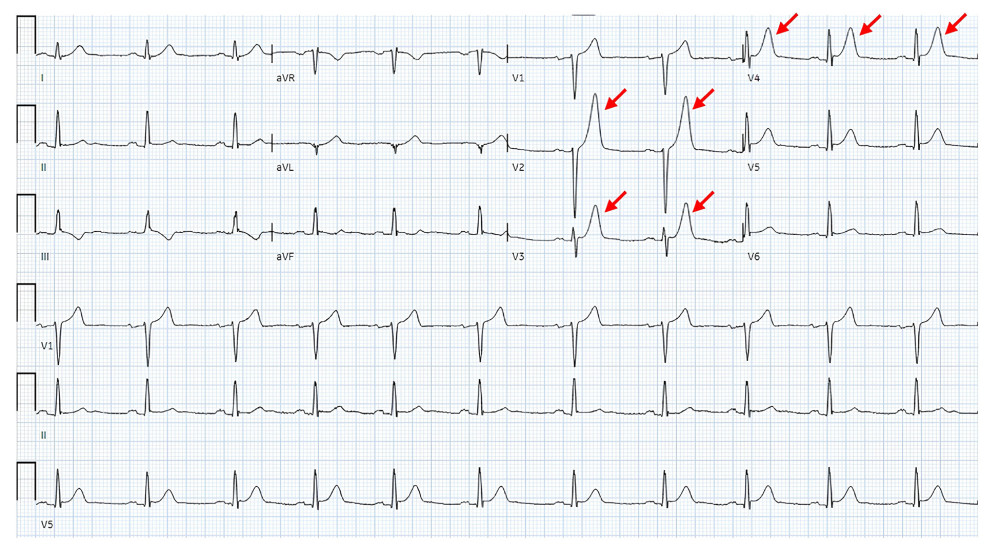 Figure 1. EKG on presentation; red arrows depicting peaked T waves.
Figure 1. EKG on presentation; red arrows depicting peaked T waves. 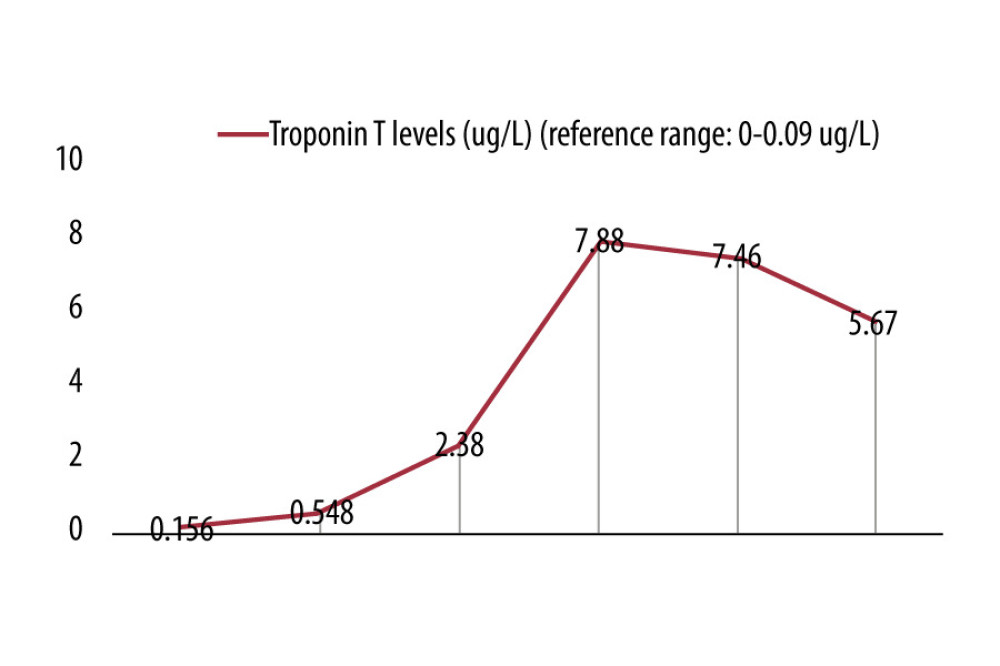 Figure 2. Graphical representation of troponin T levels.
Figure 2. Graphical representation of troponin T levels. 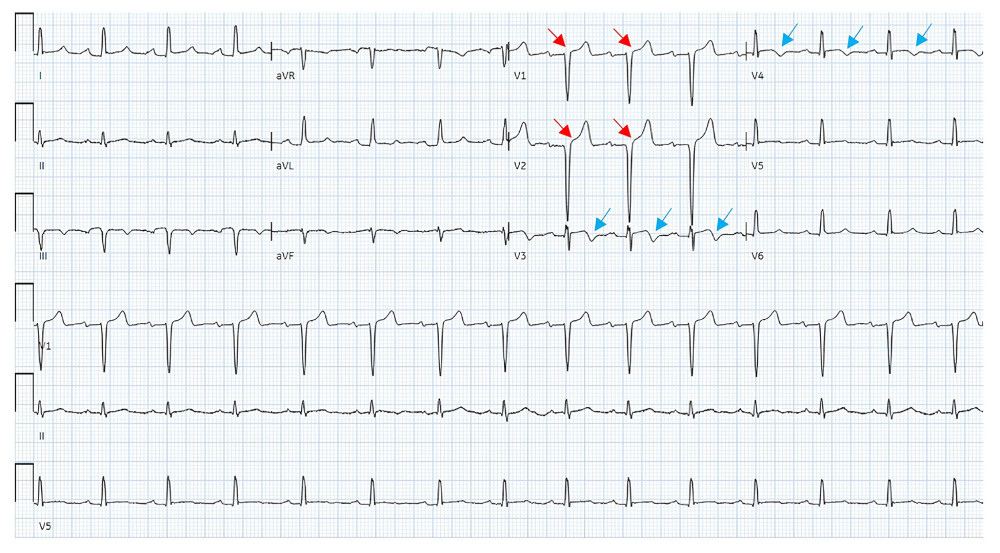 Figure 3. Red arrows depicting J point elevation of 1 mm in V1 and 2 mm in V2. Blue arrows depicting T wave inversions in V3 and V4.
Figure 3. Red arrows depicting J point elevation of 1 mm in V1 and 2 mm in V2. Blue arrows depicting T wave inversions in V3 and V4. 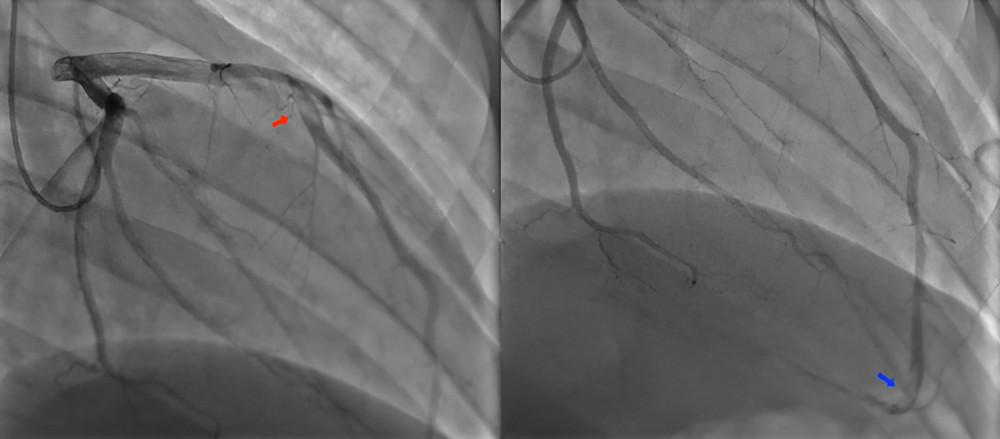 Figure 4. Coronary artery dissection in the mid left anterior descending (LAD) artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow).
Figure 4. Coronary artery dissection in the mid left anterior descending (LAD) artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow). 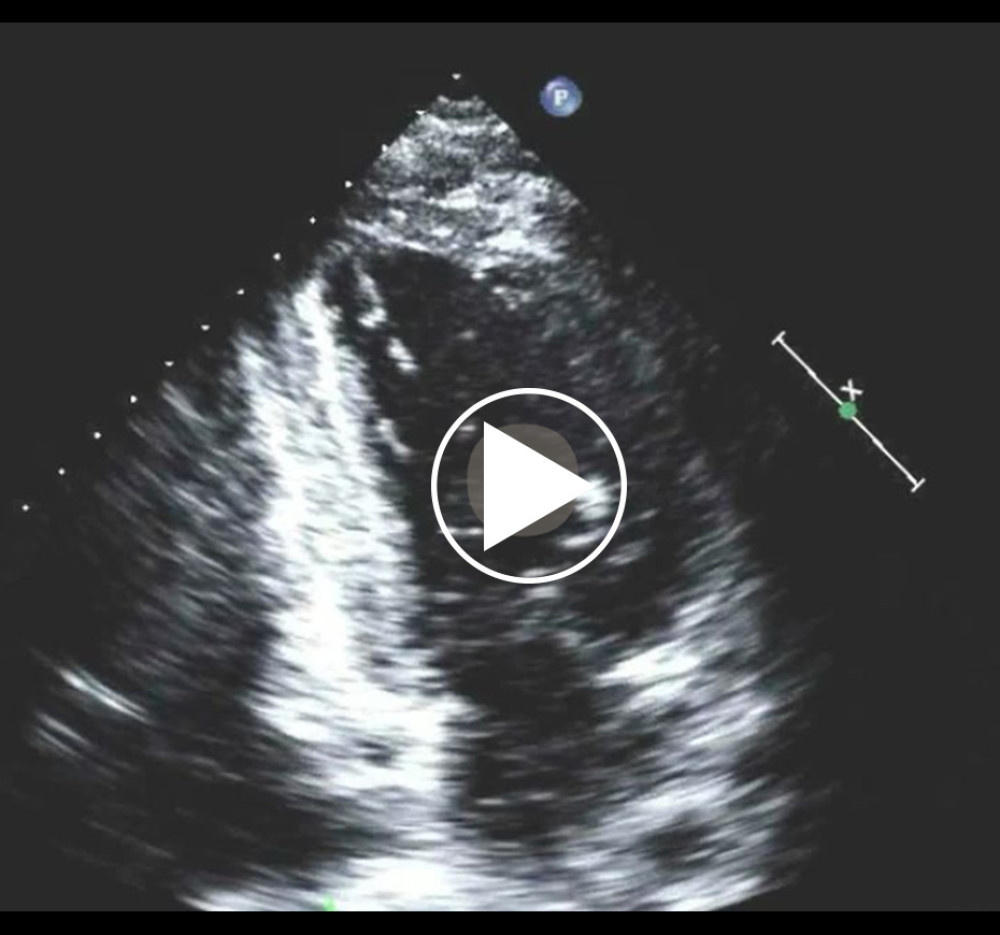 Video 1. Mid and apical inferoseptal, apical inferior, mid and apical anteroseptal, and apical hypokinesis. The ejection fraction was 50% calculated by biplane method of disks.
Video 1. Mid and apical inferoseptal, apical inferior, mid and apical anteroseptal, and apical hypokinesis. The ejection fraction was 50% calculated by biplane method of disks.  Video 2. Coronary artery dissection in the mid left anterior descending artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow).
Video 2. Coronary artery dissection in the mid left anterior descending artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow). 
References
1. Adlam D, Alfonso F, Maas A, Vrints CWriting Committee, European Society of Cardiology, acute cardiovascular care association, SCAD study group: A position paper on spontaneous coronary artery dissection: Eur Heart J, 2018; 39(36); 3353-68
2. Hayes SN, Kim ESH, Saw J, Spontaneous coronary artery dissection: Current state of the Science: A Scientific Statement from the American Heart Association: Circulation, 2018; 137(19); e523-e57
3. Hc P, Dissecting aneurysm of coronary artery in a woman aged 42: Br Med J, 1931; 1(3663); 667
4. Tweet MS, Gulati R, Hayes SN, Spontaneous coronary artery dissection: Curr Cardiol Rep, 2016; 18(7); 60
5. Nishiguchi T, Tanaka A, Ozaki Y, Prevalence of spontaneous coronary artery dissection in patients with acute coronary syndrome: Eur Heart J Acute Cardiovasc Care, 2016; 5(3); 263-70
6. Mortensen KH, Thuesen L, Kristensen IB, Christiansen EH, Spontaneous coronary artery dissection: A Western Denmark Heart Registry study: Catheter Cardiovasc Interv, 2009; 74(5); 710-17
7. Tokura M, Taguchi I, Kageyama M, Clinical features of spontaneous coronary artery dissection: J Cardiol, 2014; 63(2); 119-22
8. Rigatelli G, Rigatelli G, Rossi P, Docali G, Normal angiogram in acute coronary syndromes: The underestimated role of alternative substrates of myocardial ischemia: Int J Cardiovasc Imaging, 2004; 20(6); 471-75
9. Nakashima T, Noguchi T, Haruta S, Prognostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: A report from the Angina Pectoris-Myocardial Infarction Multicenter Investigators in Japan: Int J Cardiol, 2016; 207; 341-48
10. Vanzetto G, Berger-Coz E, Barone-Rochette G, Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: Results from a database of 11,605 patients: Eur J Cardiothorac Surg, 2009; 35(2); 250-54
11. Saw J, Aymong E, Sedlak T, Spontaneous coronary artery dissection: Association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes: Circ Cardiovasc Interv, 2014; 7(5); 645-55
12. Rogowski S, Maeder MT, Weilenmann D, Spontaneous coronary artery dissection: Angiographic follow-up and long-term clinical outcome in a predominantly medically treated population: Catheter Cardiovasc Interv, 2017; 89(1); 59-68
13. Daoulah A, Al-Faifi SM, Hurley WT, Spontaneous coronary artery dissection: Does being unemployed matter? Insights from the GSCAD Registry: Curr Cardiol Rev, 2021; 17(3); 328-39
14. McAlister C, Alfadhel M, Samuel R, Differences in demographics and outcomes between men and women with spontaneous coronary artery dissection: JACC Cardiovasc Interv, 2022; 15(20); 2052-61
15. Fahmy P, Prakash R, Starovoytov A, Pre-disposing and precipitating factors in men with spontaneous coronary artery dissection: JACC Cardiovasc Interv, 2016; 9(8); 866-68
16. Zilio F, Muraglia S, Morat F, Sex differences in clinical and angiographic characteristics in spontaneous coronary artery dissection: Future Cardiol, 2021; 17(4); 669-75
17. Waterbury TM, Tarantini G, Vogel B, Non-atherosclerotic causes of acute coronary syndromes: Nat Rev Cardiol, 2020; 17(4); 229-41
18. Waterbury TM, Tweet MS, Hayes SN, Early natural history of spontaneous coronary artery dissection: Circ Cardiovasc Interv, 2018; 11(9); e006772
19. Jackson R, Al-Hussaini A, Joseph S, Spontaneous coronary artery dissection: Pathophysiological insights from optical coherence tomography: JACC Cardiovasc Imaging, 2019; 12(12); 2475-88
20. Kwon TG, Gulati R, Matsuzawa Y, Proliferation of coronary adventitial vasa vasorum in patients with spontaneous coronary artery dissection: JACC Cardiovasc Imaging, 2016; 9(7); 891-92
21. Prasad M, Tweet MS, Hayes SN, Prevalence of extracoronary vascular abnormalities and fibromuscular dysplasia in patients with spontaneous coronary artery dissection: Am J Cardiol, 2015; 115(12); 1672-77
22. Saw J, Ricci D, Starovoytov A, Spontaneous coronary artery dissection: Prevalence of predisposing conditions including fibromuscular dysplasia in a tertiary center cohort: JACC Cardiovasc Interv, 2013; 6(1); 44-52
23. Tweet MS, Hayes SN, Pitta SR, Clinical features, management, and prognosis of spontaneous coronary artery dissection: Circulation, 2012; 126(5); 579-88
24. Henkin S, Negrotto SM, Tweet MS, Spontaneous coronary artery dissection and its association with heritable connective tissue disorders: Heart, 2016; 102(11); 876-81
25. Lettieri C, Zavalloni D, Rossini R, Management and long-term prognosis of spontaneous coronary artery dissection: Am J Cardiol, 2015; 116(1); 66-73
26. Rashid HN, Wong DT, Wijesekera H, Incidence and characterisation of spontaneous coronary artery dissection as a cause of acute coronary syndrome – a single-centre Australian experience: Int J Cardiol, 2016; 202; 336-38
27. Luong C, Starovoytov A, Heydari M, Clinical presentation of patients with spontaneous coronary artery dissection: Catheter Cardiovasc Interv, 2017; 89(7); 1149-54
28. Saw J, Coronary angiogram classification of spontaneous coronary artery dissection: Catheter Cardiovasc Interv, 2014; 84(7); 1115-22
29. Prakash R, Starovoytov A, Heydari M, Catheter-induced iatrogenic coronary artery dissection in patients with spontaneous coronary artery dissection: JACC Cardiovasc Interv, 2016; 9(17); 1851-53
30. Awadalla H, Sabet S, El Sebaie A, Catheter-induced left main dissection incidence, predisposition and therapeutic strategies experience from two sides of the hemisphere: J Invasive Cardiol, 2005; 17(4); 233-36
31. Rogers JH, Lasala JM, Coronary artery dissection and perforation complicating percutaneous coronary intervention: J Invasive Cardiol, 2004; 16(9); 493-99
32. Paulo M, Sandoval J, Lennie V, Combined use of OCT and IVUS in spontaneous coronary artery dissection: JACC Cardiovasc Imaging, 2013; 6(7); 830-32
33. Saw J, Mancini GB, Humphries K, Angiographic appearance of spontaneous coronary artery dissection with intramural hematoma proven on intracoronary imaging: Catheter Cardiovasc Interv, 2016; 87(2); E54-61
34. Sharma S, Kaadan MI, Duran JM, Risk factors, imaging findings, and sex differences in spontaneous coronary artery dissection: Am J Cardiol, 2019; 123(11); 1783-87
35. Eleid MF, Tweet MS, Young PM, Spontaneous coronary artery dissection: Challenges of coronary computed tomography angiography: Eur Heart J Acute Cardiovasc Care, 2018; 7(7); 609-13
36. Tweet MS, Akhtar NJ, Hayes SN, Spontaneous coronary artery dissection: Acute findings on coronary computed tomography angiography: Eur Heart J Acute Cardiovasc Care, 2019; 8(5); 467-75
37. Roura G, Ariza-Solé A, Rodriguez-Caballero IF, Noninvasive follow-up of patients with spontaneous coronary artery dissection with CT angiography: JACC Cardiovasc Imaging, 2016; 9(7); 896-97
38. Tweet MS, Gulati R, Williamson EE, Multimodality imaging for spontaneous coronary artery dissection in women: JACC Cardiovasc Imaging, 2016; 9(4); 436-50
39. Guo LQ, Wasfy MM, Hedgire S, Multimodality imaging of spontaneous coronary artery dissection: case studies of the Massachusetts General Hospital: Coron Artery Dis, 2016; 27(1); 70-71
40. Tweet MS, Eleid MF, Best PJ, Spontaneous coronary artery dissection: Revascularization versus conservative therapy: Circ Cardiovasc Interv, 2014; 7(6); 777-86
41. Hayes SN, Tweet MS, Adlam D, Spontaneous coronary artery dissection: JACC state-of-the-art review: J Am Coll Cardiol, 2020; 76(8); 961-84
42. Saw J, Humphries K, Aymong E, Spontaneous coronary artery dissection: Clinical outcomes and risk of recurrence: J Am Coll Cardiol, 2017; 70(9); 1148-58
43. Eleid MF, Guddeti RR, Tweet MS, Coronary artery tortuosity in spontaneous coronary artery dissection: Angiographic characteristics and clinical implications: Circ Cardiovasc Interv, 2014; 7(5); 656-62
44. Main A, Prakash R, Starovoytov A, Characteristics of extension and de novo recurrent spontaneous coronary artery dissection: EuroIntervention, 2017; 13(12); e1454-e59
45. Sedlak T, Starovoytov A, Humphries K, Saw J, Coronary flow reserve in patients with prior spontaneous coronary artery dissection and recurrent angina: J Am Heart Assoc, 2020; 9(16); e015834
Figures
Figure 1. EKG on presentation; red arrows depicting peaked T waves.Figure 2. Graphical representation of troponin T levels.Figure 3. Red arrows depicting J point elevation of 1 mm in V1 and 2 mm in V2. Blue arrows depicting T wave inversions in V3 and V4.Figure 4. Coronary artery dissection in the mid left anterior descending (LAD) artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow).Video 1. Mid and apical inferoseptal, apical inferior, mid and apical anteroseptal, and apical hypokinesis. The ejection fraction was 50% calculated by biplane method of disks.Video 2. Coronary artery dissection in the mid left anterior descending artery with superimposed thrombus (red arrow) and embolized thrombus to the apical vessel, in a left dominant system (blue arrow). In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133