21 December 2025: Articles 
Allergic Bronchopulmonary Aspergillosis Presenting With Pulmonary Solid Lesions and Elevated Serum Carcinoembryonic Antigen Mimicking Lung Cancer
Unusual clinical course, Challenging differential diagnosis
Heling Wu BEF 1, Tiange Qu B 1, Shenwen Yi B 1, Jun Xu B 1, Fei Yu B 1, Liang Ye B 1*DOI: 10.12659/AJCR.947770
Am J Case Rep 2025; 26:e947770






Abstract
BACKGROUND: Allergic bronchopulmonary aspergillosis (ABPA) is a pulmonary disorder that occurs in patients allergic to Aspergillus species. It is typically characterized by reversible airway obstruction, transient pulmonary infiltrates, eosinophilia, and fever. Chest radiographs and high-resolution computed tomography (CT) are essential for diagnosis and differential diagnosis. Carcinoembryonic antigen (CEA), a tumor-specific marker, is often elevated in various malignant tumors but can also be increased in nonmalignant conditions. This overlap can result in misdiagnosis and unnecessary anxiety, leading to inappropriate clinical management. We report a case of ABPA presenting with pulmonary shadows that mimicked lung cancer, as well as elevated serum CEA levels. This report aims to enhance clinicians’ understanding of ABPA, improve diagnostic accuracy, and reduce the likelihood of misdiagnosis or missed diagnosis.
CASE REPORT: A 39-year-old woman with a history of bronchial asthma presented with a productive cough. Chest CT revealed solid lesions in the left upper pulmonary lobe with mediastinal lymphadenopathy. Her serum CEA level was elevated, raising suspicion of malignancy. A positron emission tomography-CT scan demonstrated increased fluorodeoxyglucose uptake in the lungs. However, a CT-guided percutaneous lung biopsy, combined with other relevant diagnostic tests, confirmed ABPA according to the International Society for Human and Animal Mycology (ISHAM) criteria. After corticosteroid therapy, both the radiographic findings and serum CEA levels improved.
CONCLUSIONS: To avoid unnecessary invasive procedures and misdiagnosis of malignancy, ABPA should be considered in the differential diagnosis of patients with asthma who present with pulmonary solid lesions and elevated serum CEA levels.
Keywords: Aspergillosis, Allergic Bronchopulmonary, Carcinoembryonic Antigen, Lung Diseases, Fungal, Humans, Diagnosis, Differential, Female, lung neoplasms, adult, Tomography, X-Ray Computed
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is a pulmonary disorder that occurs in patients allergic to
Case Report
CLINICAL PRESENTATION:
A 39-year-old woman with a history of bronchial asthma and a 6-month progression of dyspnea and wheezing presented to our department. She reported no fever, chest pain, orthopnea, hemoptysis, abdominal pain, bloating, or abnormal vaginal bleeding. She had previously received 2 courses of piperacillin–tazobactam combined with levofloxacin; however, her symptoms did not improve. She had no history of pulmonary tuberculosis, malignancy, or immunosuppressive therapy. Her menstrual cycles were regular, and she denied pregnancy preparation. On physical examination, her vital signs were as follows: temperature, 36.6°C; heart rate, 95 beats per minute; respiratory rate, 22 breaths per minute; oxygen saturation, 96% on room air; and blood pressure, 115/65 mmHg. No superficial lymphadenopathy was observed. Respiratory examination revealed tachypnea and harsh breath sounds with scattered inspiratory and expiratory wheezes. Cardiac examination demonstrated tachycardia with normal heart sounds and no audible murmur, rub, or gallop. The abdomen and extremities were unremarkable; neurological findings were normal.
INVESTIGATIONS:
Laboratory findings were as follows: erythrocyte sedimentation rate, 65 mm/h (reference range: <20 mm/h); hematocrit, 40% (reference range: 37–48%); white blood cell count, 10.22×109/L (reference range: 4–10×109/L); neutrophils, 5.92×109/L (reference range: 1.5–8×109/L); eosinophils, 1.69×109/L (reference range: 0.05–0.5×109/L); and C-reactive protein, 23.3 mg/L (reference range: <2.87 mg/L). Serum squamous cell carcinoma antigen and neuron-specific enolase concentrations were within normal limits. Liver transaminase levels were not significantly elevated; urea, creatinine, myocardial enzyme, and troponin levels were within normal ranges. The serum CEA concentration was 52.31 ng/mL (reference range: <5 ng/mL). The total serum IgE concentration was substantially elevated at 2,700 U/mL (reference range: 0–250 U/mL). Pulmonary function testing demonstrated moderate airflow obstruction (predicted forced expiratory volume in 1 s, 71%) without evidence of restriction (predicted vital capacity, 91%). Fractional exhaled nitric oxide was considerably elevated at 116 ppb (reference range: <25 ppb). A CT scan revealed solid lesions in the lingular segment of the left upper pulmonary lobe, containing low-density cystic areas, along with mediastinal lymphadenopathy (Figure 1). Based on these findings, pulmonary malignancy was suspected, and a positron emission tomography (PET)-CT scan was performed. The scan demonstrated a solid lesion in the lingular segment of the left upper lobe with increased fluorodeoxyglucose (FDG) uptake, for which malignancy could not be excluded. Enlarged mediastinal and bilateral hilar lymph nodes also exhibited increased FDG uptake, raising suspicion of possible metastasis.
DIAGNOSIS:
PET-CT showed considerably increased uptake in the pulmonary lesion, indicating a high likelihood of lung malignancy. A CT-guided percutaneous lung biopsy was subsequently performed, and histopathologic examination confirmed eosinophilic pneumonia (Figure 2). Photomicrographs demonstrated abundant eosinophil infiltration within the alveoli and interstitium, consistent with eosinophilic pneumonia. No malignant cells or bacterial or fungal organisms were identified. Electronic colonoscopy and gastroscopy revealed no abnormal findings. Gel diffusion testing revealed Aspergillus-specific IgE antibody positivity and Aspergillus fumigates-precipitating antibody positivity. The skin test for Aspergillus fumigatus also displayed positive results. Because there was no evidence of involvement of other organs such as the heart, kidneys, or gastrointestinal tract, and no histologic evidence suggested necrotizing vasculitis or extravascular granulomas, eosinophilic granulomatosis with polyangiitis was excluded. Chest CT scans also indicated no pulmonary fibrosis or involvement of the skin, nervous system, or other organs. The findings met the diagnostic criteria for ABPA established by the International Society for Human and Animal Mycology (ISHAM). Given that hypereosinophilic syndrome is a diagnosis of exclusion, the final diagnosis was ABPA.
TREATMENT AND FOLLOW-UP:
The patient was treated with prednisolone (0.5 mg/kg daily) for 15 days, resulting in rapid improvement of symptoms. Peripheral eosinophil counts sharply declined, and the serum CEA concentration decreased to 19.79 ng/mL. At the 6-month follow-up, the patient remained free of cough and wheezing; the serum CEA concentration had further declined to 3.15 ng/mL. Follow-up thoracic CT demonstrated robust resolution of shadows in the left upper lung (Figure 3).
Discussion
We have described a female patient who exhibited ABPA associated with elevated serum CEA levels. In this case, neoplastic disease was excluded based on tumor marker analysis, PET-CT findings, colonoscopy, and upper gastrointestinal endoscopy. Notably, serum CEA concentrations substantially decreased in parallel with clinical improvement after corticosteroid therapy.
ABPA, a severe respiratory complication in patients with asthma, may progress to irreversible pulmonary fibrosis without timely corticosteroid therapy. Imaging features of ABPA, including consolidations, mucus plugs [8], and pulmonary masses, often resemble those of malignant lesions. This overlap – both biochemical (elevated CEA) and radiologic – creates serious diagnostic challenges, as demonstrated in the present case, which initially met the criteria for suspected lung cancer. Such cases require a comprehensive differential diagnosis integrating bronchoscopy, biopsy, and serologic testing to avoid unnecessary invasive procedures. In this case, the plaque-like condensed shadows in the left upper lung, accompanied by mediastinal lymphadenopathy, were ultimately identified as mucus plugs obstructing the left lingular bronchus.
Although CEA is conventionally regarded as a tumor marker, elevated levels have been documented in nonneoplastic conditions such as ABPA [9]. Our observations are consistent with a Japanese study that showed increased CEA concentrations in patients with ABPA [7]. The mechanisms underlying this elevation may include mucus hypersecretion from hypertrophic bronchial glands that overproduce glycoproteins containing CEA; inflammatory exudation resulting from chronic airway inflammation that facilitates CEA leakage into the systemic circulation; and direct secretion of CEA by eosinophils [10]. These mechanisms are supported by the link between serum CEA levels and peripheral eosinophil counts observed in our patient. In the present case, the serum CEA concentration considerably declined after a 4-month course of prednisolone therapy, in parallel with substantial radiographic improvement. These findings suggest that serum CEA can serve as a biomarker for monitoring therapeutic response in ABPA.
After glucocorticoid treatment, the patient’s serum CEA concentration considerably decreased, accompanied by clinical improvement. However, glucocorticoid use suppresses immune function, which may predispose patients to recurrent or opportunistic infections [11]. Therefore, regular outpatient follow-up is essential, with appropriate adjustment of medication dosage. In cases of disease progression or complications such as hemoptysis, immediate symptomatic management should be instituted, and surgical intervention may be considered if necessary [12].
Conclusions
Patients with ABPA may present with nonspecific clinical features that progress insidiously, leading to severe pulmonary damage. Early diagnosis and timely treatment can greatly improve prognosis. ABPA should be included in the differential diagnosis of patients with asthma who display elevated serum CEA levels, irrespective of hilar and mediastinal lymphadenopathy status.
Figures
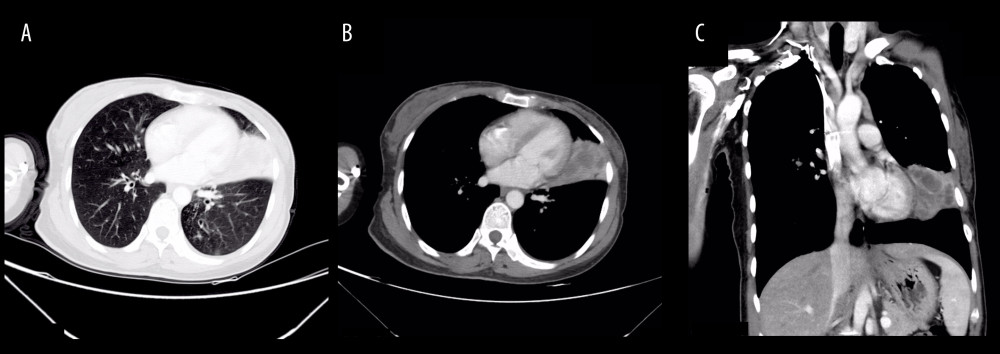 Figure 1. Computed tomography scan showing solid lesions in the lingular segment of the left upper pulmonary lobe. Low-density cystic shadows were observed within the lesions, accompanied by mediastinal lymphadenopathy (A: lung window; B: mediastinal window; C: coronal reconstruction).
Figure 1. Computed tomography scan showing solid lesions in the lingular segment of the left upper pulmonary lobe. Low-density cystic shadows were observed within the lesions, accompanied by mediastinal lymphadenopathy (A: lung window; B: mediastinal window; C: coronal reconstruction). 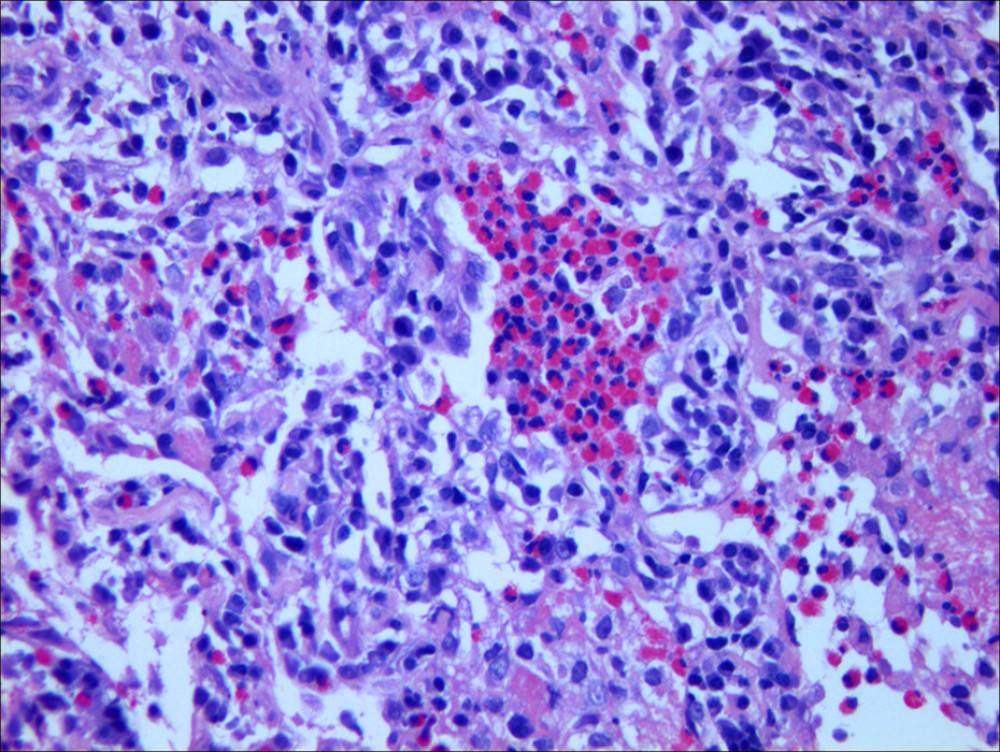 Figure 2. Photomicrograph showing eosinophilic infiltration in the alveoli and interstitium, consistent with eosinophilic pneumonia. Images obtained after hematoxylin and eosin staining at 200× magnification.
Figure 2. Photomicrograph showing eosinophilic infiltration in the alveoli and interstitium, consistent with eosinophilic pneumonia. Images obtained after hematoxylin and eosin staining at 200× magnification. 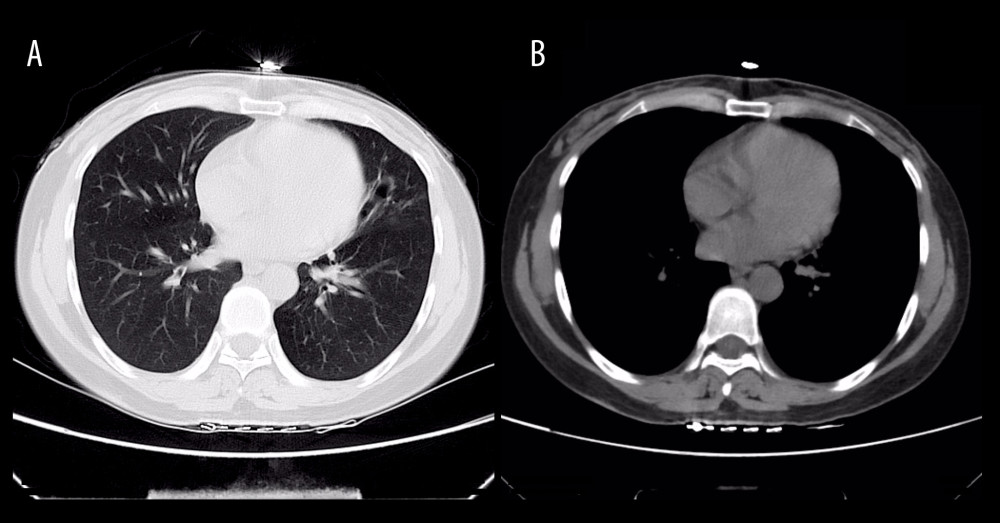 Figure 3. Computed tomography scan demonstrating resolution of lesions in the lingular segment of the left upper lobe (A: lung window; B: mediastinal window).
Figure 3. Computed tomography scan demonstrating resolution of lesions in the lingular segment of the left upper lobe (A: lung window; B: mediastinal window). References
1. Agarwal R, Allergic bronchopulmonary aspergillosis: Chest, 2009; 135(3); 805-26
2. Moss RB, Treatment options in severe fungal asthma and allergic bronchopulmonary aspergillosis: Eur Respir J, 2014; 43(5); 1487-500
3. Ward S, Heyneman L, Lee MJ, Accuracy of CT in the diagnosis of allergic bronchopulmonary aspergillosis in asthmatic patients: Am J Roentgenol, 1999; 173(4); 937-42
4. Akolkar D, Patil D, Page R, Circulating ensembles of tumor-associated cells in gastrointestinal cancers: J Clin Oncol, 2020; 38(4 Suppl); 808
5. Guida F, Sun N, Bantis LE, Assessment of lung cancer risk on the basis of a biomarker panel of circulating proteins: JAMA Oncol, 2018; 4(10); e182078
6. Tsuburai T, Kawabata Y, Tsurikisawa NCase of eosinophilic bronchitis and bronchiolitis associated with increased level of serum CEA in asthmatics: Nihon Kokyuki Gakkai Zasshi, 2006; 44(10); 742-48 [in Japanese]
7. Noguchi T, Yamamoto K, Moriyama G, Evaluation of serum levels of carcinoembryonic antigen in allergic bronchopulmonary aspergillosis: J Nippon Med Sch, 2013; 80(6); 404-9
8. Lowes D, Chishimba L, Greaves M, Denning DW, Development of chronic pulmonary aspergillosis in adult asthmatics with ABPA: Respir Med, 2015; 109(12); 1509-15
9. Grunnet M, Sorensen JB, Carcinoembryonic antigen (CEA) as tumor marker in lung cancer: Lung Cancer, 2012; 76(2); 138-43
10. Yang Y, Gao Q, Jin Y, Eosinophils may serve as CEA-secreting cells for allergic bronchopulmonary aspergillosis (ABPA) patients: Sci Rep, 2021; 11(1); 4025
11. Dixit D, Kuete NT, Bene P, Invasive pulmonary aspergillosis with hydropneumothorax in a patient taking high-dose glucocorticoids: Am J Case Rep, 2020; 21; e928499
12. Yoneoka R, Takeda K, Kasai H, A 65-year-old man with refractory hemoptysis associated with chronic progressive pulmonary aspergillosis who failed to respond to combined endobronchial occlusion and bronchial artery embolization: A case report and literature review: Am J Case Rep, 2023; 25; e942422
Figures
Figure 1. Computed tomography scan showing solid lesions in the lingular segment of the left upper pulmonary lobe. Low-density cystic shadows were observed within the lesions, accompanied by mediastinal lymphadenopathy (A: lung window; B: mediastinal window; C: coronal reconstruction).Figure 2. Photomicrograph showing eosinophilic infiltration in the alveoli and interstitium, consistent with eosinophilic pneumonia. Images obtained after hematoxylin and eosin staining at 200× magnification.Figure 3. Computed tomography scan demonstrating resolution of lesions in the lingular segment of the left upper lobe (A: lung window; B: mediastinal window). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133