Call: 1.631.629.4328
Mon-Fri 10 am - 2 pm EST
24 July 2025: Articles 
Ectopic Adrenocortical Adenoma Causing Malignant Hypertension and Hypokalemia
Challenging differential diagnosis, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Xiaoyong HuDOI: 10.12659/AJCR.948022
Am J Case Rep 2025; 26:e948022






Abstract
BACKGROUND: Ectopic adrenocortical adenomas are rare and can produce aldosterone autonomously, causing resistant hypertension and hypokalemia. Atypical locations pose diagnostic challenges. This report describes a 45-year-old man with malignant hypertension and hypokalemia due to an aldosterone-producing ectopic adrenal adenoma located between the pancreas and left adrenal gland.
CASE REPORT: A 45-year-old man with a 9-year history of poorly controlled hypertension presented with dizziness, vomiting, and fatigue. On admission, blood pressure was 192/110 mmHg and serum potassium was 2.07 mmol/L. Physical examination revealed left ventricular hypertrophy and hypertensive end-organ damage. Laboratory test results showed elevated plasma aldosterone (47.61 ng/dL) and suppressed renin (0.04 ng/mL/h), yielding an aldosterone-to-renin ratio of 1190. Abdominal CT and MRI identified a 3-cm solid cystic mass between the pancreatic tail and lateral branch of the left adrenal gland. Cortisol circadian rhythm, dehydroepiandrosterone sulfate, and plasma metanephrines were within normal limits, excluding other functional adrenal tumors. The patient underwent complete surgical resection of the ectopic adrenal adenoma. Histopathology confirmed adrenal cortical adenoma with focal adrenal medullary hyperplasia. At 1-year follow-up, he had normal blood pressure and serum potassium levels on an antihypertensive regimen.
CONCLUSIONS: This case highlights a rare ectopic aldosterone-producing adrenal adenoma near the pancreas. A thorough biochemical and imaging workup was essential for diagnosis, and surgical resection achieved clinical resolution. Ectopic adrenal tumors should be considered in the differential diagnosis of resistant hypertension with hypokalemia when standard adrenal imaging is inconclusive.
Keywords: Adrenal Glands, Endocrine System Diseases, Hypertension, Hypokalemia, Pancreas, Aldosterone
Introduction
Hypertension accompanied by hypokalemia often indicates an aldosterone-mediated pathology, most commonly primary aldosteronism (Conn syndrome). Population-based data suggest that approximately 8% of patients with primary hypertension have primary aldosteronism [1]. Despite its prevalence, primary aldosteronism remains underdiagnosed and confers a disproportionately high risk of cardiovascular morbidity and mortality [2–4]. In most cases, primary aldosteronism is caused by an adrenocortical aldosterone-producing adenoma driven by somatic mutations that promote autonomous aldosterone secretion [3]. Even mild, asymptomatic hypokalemia (serum potassium 2.5–3.4 mEq/L) has been linked to increased cardiovascular events and higher all-cause mortality [5], highlighting the importance of early detection. Surgical resection of the overactive adrenal gland in unilateral primary aldosteronism results in biochemical cure for over 95% of patients, leading to normalization of blood pressure and potassium levels [6].
Primary aldosteronism prevalence is not uniform across all hypertensive populations. In unselected cohorts, 5% to 10% of patients with hypertension have primary aldosteronism, but this rises to 22% to 39% among those with stage III–IV hypertension and evidence of end-organ damage, such as grade III–IV hypertensive retinopathy or left ventricular hypertrophy [1,7]. Clinically, primary aldosteronism often presents as resistant hypertension, spontaneous hypokalemia, metabolic alkalosis, and target-organ injury, including left ventricular hypertrophy and proteinuria [2,8]. Initial screening is performed using the plasma aldosterone-to-renin ratio (ARR), and an elevated ARR requires confirmatory testing (eg, saline infusion or captopril challenge) to verify autonomous aldosterone production [2,8]. Once biochemical confirmation is obtained, imaging with computed tomography (CT) or magnetic resonance imaging (MRI) is used to localize the adenoma, and adrenal venous sampling is recommended when imaging is equivocal or bilateral disease is suspected [2,8]. Management depends on subtype: unilateral aldosterone-producing adenoma is treated by adrenalectomy, which yields long-term blood pressure improvement and cardiovascular risk reduction [6], whereas patients with bilateral adrenal hyperplasia or who are unfit for surgery receive mineralocorticoid receptor antagonists, with careful monitoring of serum potassium and blood pressure [8,9].
Ectopic adrenal adenomas, although rare, have been reported in a variety of anatomical locations, reinforcing the need for thorough imaging and biochemical assessment. Notable locations described in the literature include the renal hilum, gastric wall, liver, spine, and spinal canal [8–21]. For example, Nakamura et al reported an ectopic adrenal adenoma in the pancreas presenting as a solid pseudopapillary neoplasm with gastric varices and portal hypertension [20]. Additional cases include those in the renal sinus [12,15], gastric wall [13], and spinal region [11,17], and even instances of dual ectopic and intra-adrenal adenomas [21]. However, no prior report describes an aldosterone-producing adenoma located precisely between the pancreas and left adrenal gland.
This report describes a 45-year-old man with malignant hypertension and refractory hypokalemia due to an aldosterone-producing ectopic adrenal adenoma located between the pancreas and left adrenal gland, highlighting the clinical presentation, comprehensive diagnostic evaluation, and successful surgical intervention of this rare entity.
Case Report
A 45-year-old man with a 9-year history of poorly controlled hypertension – first diagnosed at age 36 years – presented with dizziness, vomiting, and intermittent fatigue. His blood pressure on admission was 192/110 mmHg, and laboratory testing revealed hypokalemia with a serum potassium level of 2.07 mmol/L (reference range: 3.5–5.0 mmol/L) (Table 1). He had no significant family history of cardiovascular disease but reported a history of smoking and elevated homocysteine levels. At presentation, he was taking sustained-release nifedipine intermittently; despite this, blood pressure control remained inadequate.
During hospitalization, antihypertensive therapy was intensified with the addition of losartan, bisoprolol, terazosin, and spironolactone. After correcting hypokalemia, an ARR was obtained while the patient remained on nifedipine and losartan, which may have influenced the ARR value.
On physical examination, his height was 173 cm and weight 66 kg (body mass index 22.05 kg/m2), with an abdominal circumference of 84 cm. Vital signs included temperature 36.4°C, heart rate 98 bpm, respiratory rate 20 breaths per min, and bilateral brachial blood pressures of 180/104 mmHg (right arm) and 178/102 mmHg (left arm). Cardiovascular assessment revealed a slightly displaced point of maximal impulse, consistent with left ventricular enlargement; cardiac rhythm was regular with no murmurs. The abdomen was soft and non-tender, without palpable masses, striae, or bruits; hepatosplenomegaly was absent. The thyroid gland was normal, and there was no jugular venous distension. Neurological examination showed intact cranial nerves and deep tendon reflexes, with no focal deficits or peripheral edema. These findings, together with his history of resistant hypertension and hypokalemia, raised strong suspicion for an underlying secondary cause, prompting further endocrine and imaging evaluation.
Laboratory evaluation demonstrated elevated plasma aldosterone of 47.61 ng/dL (reference range: 2.94–16.15 ng/dL) and suppressed plasma renin activity of 0.04 ng/mL/h (reference range: 0.20–2.50 ng/mL/h), resulting in an ARR of 1190 (Table 2). These values confirmed biochemical primary aldosteronism, despite ongoing nifedipine and losartan therapy. Cortisol circadian rhythm testing showed normal results (8: 00 AM, 17.9 μg/dL; 4: 00 PM, 12.8 μg/dL; midnight, 7.09 μg/dL). Dehydroepiandrosterone sulfate and thyroid function tests were within normal limits. Plasma metanephrine (26.00 ng/mL) and normetanephrine (73.68 ng/mL) levels were not elevated, excluding pheochromocytoma and cortisol-producing tumors. Genetic testing for KCNJ5, ATP1A1, and CACNA1D mutations was not performed, due to limited access and cost constraints.
Cardiac workup revealed grade 3 hypertension with target-organ damage: echocardiography showed left ventricular hypertrophy, with an ejection fraction of 47% and abnormal electrocardiogram findings; brain MRI detected multiple lacunar infarctions; and fundoscopy demonstrated grade II hypertensive retinopathy.
Abdominal CT (Figure 1) revealed a well-defined, 3-cm mass between the lower margin of the pancreas and the left lateral ramus of the adrenal gland; the right adrenal gland was normal. Although the radiology report did not document Hounsfield unit values, enhancement patterns and location suggested an adrenal-origin lesion. MRI (Figure 2) further characterized this as a solid-cystic mass in the same region, consistent with an ectopic adrenocortical adenoma.
Given the tumor’s unusual location and biochemical confirmation of primary aldosteronism, the patient underwent complete surgical resection by the general surgery team. The procedure was uneventful, with no intraoperative or postoperative complications. Although video documentation was not available due to institutional constraints, operative details were fully recorded in the medical record and corroborated by histopathology.
Histopathological examination (Figures 3, 4) confirmed an adrenal cortical adenoma with focal adrenal medullary hyperplasia. Immunohistochemistry revealed negative staining for cytokeratin, synaptophysin, chromogranin A, α-inhibin, calcitonin, vimentin, S-100, and GFAP; CD56 was positive. The Ki-67 index was low (2–3%), consistent with a benign adenoma. There was no clinical or laboratory evidence of multiple endocrine neoplasia syndromes; evaluation of the thyroid, pituitary, and parathyroid glands was unremarkable, and there was no pertinent family history.
Postoperatively, the patient’s blood pressure and serum potassium normalized rapidly. His antihypertensive regimen was simplified to sustained-release felodipine monotherapy. At the 1-year follow-up, he remained normotensive (120-130/70-80 mmHg) and normokalemic (3.6–4.2 mmol/L) on this regimen. Although repeat CT/MRI and hormonal testing were recommended, the patient declined further evaluations, due to financial limitations.
Discussion
NOVELTY AND UNIQUENESS OF THE CASE:
This report documents a highly unusual presentation of an ectopic adrenocortical adenoma in the peripancreatic region, a location seldom reported in the literature. Its anatomical position complicated the diagnostic process and could easily have been misinterpreted as a pancreatic or retroperitoneal tumor. The correct diagnosis was achieved through the integration of hormonal testing, high-resolution imaging, and intraoperative pathology.
INTEGRATION OF FINDINGS:
This case reinforces the critical role of comprehensive diagnostic workups in young hypertensive patients, particularly when standard adrenal imaging is inconclusive. The patient’s rapid clinical improvement following surgical resection further supports existing evidence that early recognition and management of functional adrenal tumors can lead to complete clinical remission.
IMPLICATIONS FOR PRACTICE:
Clinicians should consider ectopic adrenal tumors in the differential diagnosis of unexplained hypertension with hypokalemia, particularly when adrenal glands appear normal on imaging. Even in resource-limited settings, a stepwise evaluation combining biochemical testing, imaging, and surgical pathology can lead to successful diagnosis and curative treatment. This case highlights the value of a multidisciplinary approach and contributes to the broader understanding of atypical presentations of secondary hypertension.
Conclusions
Ectopic aldosterone-producing adrenal adenomas, although rare, should be considered in young patients with resistant hypertension and hypokalemia when standard adrenal imaging is inconclusive. In this case, an ectopic adrenocortical adenoma situated between the pancreas and left adrenal gland was identified through combined imaging, hormonal evaluation, and histopathology. Surgical resection led to prompt normalization of blood pressure and serum potassium, with sustained clinical stability at 12 months. Despite financial constraints limiting follow-up imaging and genetic testing, the diagnosis was supported by comprehensive clinical, biochemical, and pathological data. This case underscores the importance of maintaining a high index of suspicion for secondary hypertension, pursuing a thorough differential diagnosis, including cortisol-producing tumors and pheochromocytoma, and initiating early surgical management to achieve complete clinical remission.
Figures
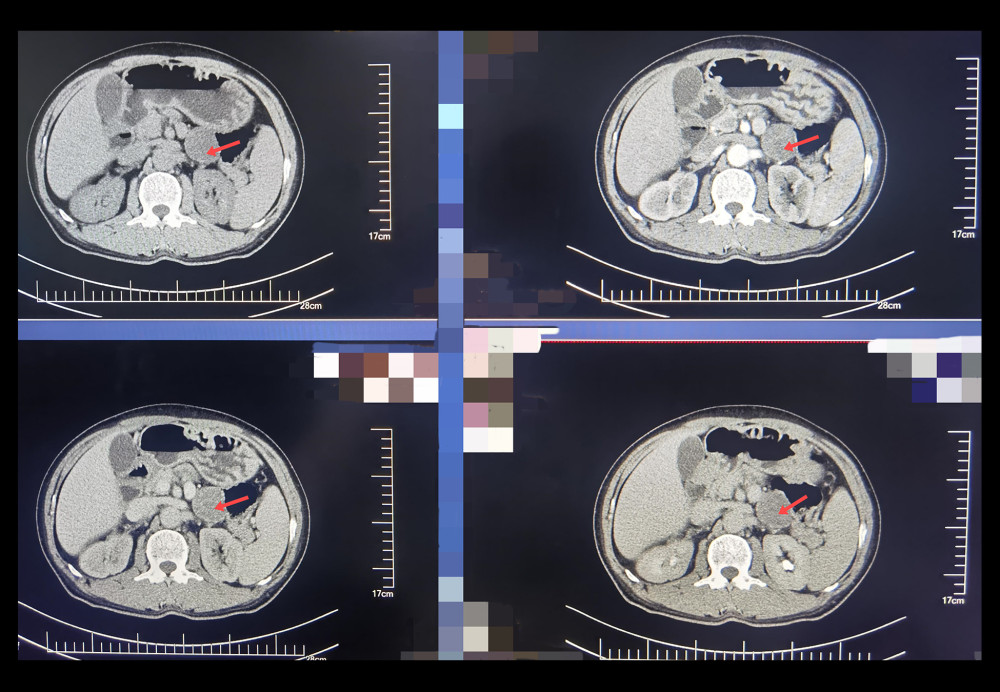 Figure 1. Contrast-enhanced computed tomography axial image demonstrating a 3-cm hyper-enhancing ectopic adrenal lesion (arrow) situated between the pancreatic tail and left adrenal remnant.
Figure 1. Contrast-enhanced computed tomography axial image demonstrating a 3-cm hyper-enhancing ectopic adrenal lesion (arrow) situated between the pancreatic tail and left adrenal remnant. 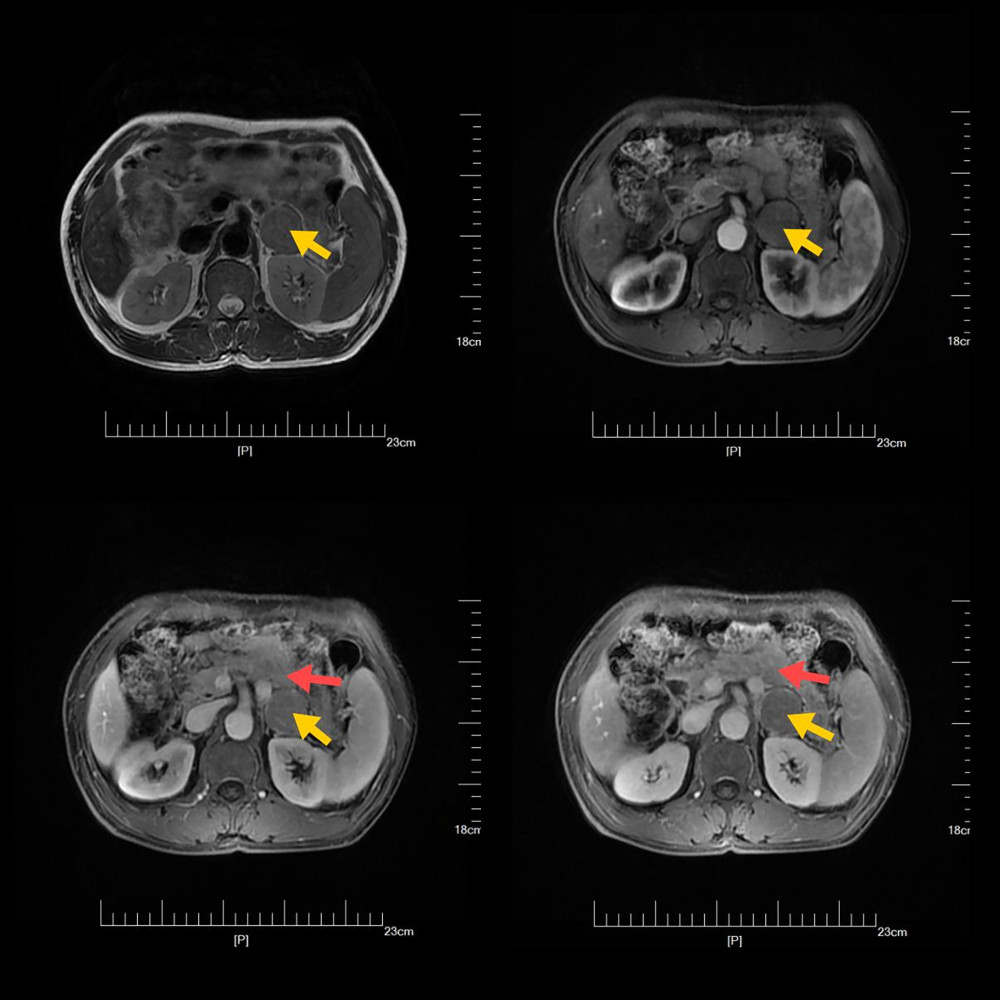 Figure 2. Magnetic resonance imaging T2-weighted coronal image showing a hyperintense mass (arrow) located between the lower margin of the pancreas and the lateral branch of the left adrenal gland.
Figure 2. Magnetic resonance imaging T2-weighted coronal image showing a hyperintense mass (arrow) located between the lower margin of the pancreas and the lateral branch of the left adrenal gland.  Figure 3. Histopathological features of adrenal cortical adenoma with focal medullary hyperplasia. (A–F) Hematoxylin and eosin staining of adrenal tumor tissue sections demonstrates a clear zonal distinction between oncocytic and lipid-rich clear cells. (A, C, E) Low (100×), intermediate (200×), and high magnification (400×) views showing oncocytic cells with eosinophilic, granular cytoplasm, and sparse lipid droplets (black arrows). These cells are arranged in solid nests and trabeculae. (B, D, F) Corresponding magnifications highlighting lipid-rich clear cells (black arrows), characterized by vacuolated, optically clear cytoplasm and peripherally displaced nuclei. Notably, focal adrenal medullary hyperplasia is observed interspersed among cortical elements, indicating mixed histological features.
Figure 3. Histopathological features of adrenal cortical adenoma with focal medullary hyperplasia. (A–F) Hematoxylin and eosin staining of adrenal tumor tissue sections demonstrates a clear zonal distinction between oncocytic and lipid-rich clear cells. (A, C, E) Low (100×), intermediate (200×), and high magnification (400×) views showing oncocytic cells with eosinophilic, granular cytoplasm, and sparse lipid droplets (black arrows). These cells are arranged in solid nests and trabeculae. (B, D, F) Corresponding magnifications highlighting lipid-rich clear cells (black arrows), characterized by vacuolated, optically clear cytoplasm and peripherally displaced nuclei. Notably, focal adrenal medullary hyperplasia is observed interspersed among cortical elements, indicating mixed histological features.  Figure 4. Immunohistochemical characterization of adrenal cortical adenoma. (A) Hematoxylin and eosin staining showing preserved adrenal architecture with cortical neoplastic proliferation. (B–K) Immunohistochemical staining profiles of the tumor tissue: (B) CD56 shows positive membranous staining, suggestive of neuroendocrine differentiation. (C–H) Negative immunoreactivity for chromogranin A, calcitonin, epithelial membrane antigen, glial fibrillary acidic protein, Ki-67 (low proliferative index), and S-100, respectively, supporting a benign cortical origin. (I) Vimentin shows diffuse cytoplasmic positivity, consistent with mesenchymal expression in adrenal cortical tumors. (J) α-Inhibin staining is negative, further excluding adrenal cortical carcinoma. (K) Synaptophysin is negative, ruling out medullary neoplasms. Together, these findings confirm the diagnosis of a benign adrenal cortical adenoma with focal medullary hyperplasia and exclude other cortical and medullary neoplasms.
Figure 4. Immunohistochemical characterization of adrenal cortical adenoma. (A) Hematoxylin and eosin staining showing preserved adrenal architecture with cortical neoplastic proliferation. (B–K) Immunohistochemical staining profiles of the tumor tissue: (B) CD56 shows positive membranous staining, suggestive of neuroendocrine differentiation. (C–H) Negative immunoreactivity for chromogranin A, calcitonin, epithelial membrane antigen, glial fibrillary acidic protein, Ki-67 (low proliferative index), and S-100, respectively, supporting a benign cortical origin. (I) Vimentin shows diffuse cytoplasmic positivity, consistent with mesenchymal expression in adrenal cortical tumors. (J) α-Inhibin staining is negative, further excluding adrenal cortical carcinoma. (K) Synaptophysin is negative, ruling out medullary neoplasms. Together, these findings confirm the diagnosis of a benign adrenal cortical adenoma with focal medullary hyperplasia and exclude other cortical and medullary neoplasms. 


References
1. Voulgaris N, Tyfoxylou E, Vlachou S, Prevalence of primary aldosteronism across the stages of hypertension based on a new combined overnight test: Horm Metab Res, 2021; 53(7); 461-69
2. Hundemer GL, Imsirovic H, Vaidya A, Screening rates for primary aldosteronism among individuals with hypertension plus hypokalemia: A population-based retrospective cohort study: Hypertension, 2022; 79; 178-86
3. Gong S, Sun N, Meyer LS, Primary aldosteronism: Spatial multiomics mapping of genotype-dependent heterogeneity and tumor expansion of aldosterone-producing adenomas: Hypertension, 2023; 80; 1555-67
4. Kantauskaite M, Fürst G, Minko P, How acute renal failure led to the diagnosis of aortic coarctation: J Hypertens, 2023; 41(3); 520-24
5. Kovesdy CP, Matsushita K, Sang Y, Serum potassium and adverse outcomes across the range of kidney function: A CKD Prognosis Consortium meta-analysis: Eur Heart J, 2018; 39; 1535-42
6. Williams TA, Reincke M, Pathophysiology and histopathology of primary aldosteronism: Trends Endocrinol Metab, 2022; 33(1); 36-49
7. Brum de Sousa E, do Mar Menezes M, Cordeiro AM, A case report of primary aldosteronism and extensive hypertension-mediated organ damage: Cureus, 2024; 16(2); e53818
8. Funder JW, Carey RM, Mantero F, The management of primary aldosteronism: Case detection, diagnosis, and treatment: An endocrine society clinical practice guideline: J Clin Endocrinol Metab, 2016; 101; 1889-916
9. Xie Z, Zhu H, A rare case of mitral regurgitation caused by primary aldosteronism: Eur Heart J, 2023; 44; 1960
10. Clase CM, Carrero J-J, Ellison DH, Potassium homeostasis and management of dyskalemia in kidney diseases: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference: Kidney Int, 2020; 97; 42-61
11. Makino K, Kojima R, Nakamura H, Ectopic adrenal cortical adenoma in the spinal region: Case report and review of the literature: Brain Tumor Pathol, 2010; 27; 121-25
12. Zhang J, Liu B, Song N, An ectopic adreocortical adenoma of the renal sinus: A case report and literature review: BMC Urol, 2016; 16; 3
13. Ren P-T, Ectopic adrenal cortical adenoma in the gastric wall: Case report: World J Gastroenterol, 2013; 19; 778
14. Kepes JJ, O’Boynick P, Jones S, Adrenal cortical adenoma in the spinal canal of an 8-year-old girl: Am J Surg Pathol, 1990; 14; 481-84
15. Liu Y, Jiang Y-F, Wang Y-L, Ectopic adrenocortical adenoma in the renal hilum: A case report and literature review: Diagn Pathol, 2016; 11; 40
16. Chen J, Wan X, Lu Y, An ectopic adrenocortical oncocytic adenoma in the liver highly mimicking hepatocellular carcinoma: case report and literature review: Diagn Pathol, 2021; 16; 58
17. Nemir J, Štenger M, Jakovčević A, Adrenal cortical adenoma in the spinal canal: A case report and review of the literature: J Neurol Surg A Cent Eur Neurosurg, 2020; 81; 71-74
18. Cardinalli IA, de Oliveira-Filho AG, Mastellaro MJ, A unique case of synchronous functional adrenocortical adenoma and myelolipoma within the ectopic adrenal cortex in a child with Beckwith-Wiedemann syndrome: Pathol Res Pract, 2012; 208; 189-94
19. Park WY, Seo H, Choi KU, Three cases of adrenocortical tumors mistaken for hepatocellular carcinomas/diagnostic pitfalls and differential diagnosis: Ann Diagn Pathol, 2017; 31; 9-13
20. Nakamura S, Takayama Y, Kuboki Y, A case of solid pseudopapillary neoplasm of the pancreas presenting with left-sided extrahepatic portal hypertension: Intern Med, 2010; 49(16); 1749-53
21. Choukair D, Beuschlein F, Zwermann O, Virilization of a young girl caused by concomitant ectopic and intra-adrenal adenomas of the adrenal cortex: Horm Res Paediatr, 2013; 79; 318-22
22. Chen N, He X, Feng Y, Effects of resistance training in healthy older people with sarcopenia: A systematic review and meta-analysis of randomized controlled trials: Eur Rev Aging Phys Act, 2021; 18(1); 23
23. Nakamura H, Vo P, Kanakis I, Aggrecanase-selective tissue inhibitor of metalloproteinase-3 (TIMP3) protects articular cartilage in a surgical mouse model of osteoarthritis: Sci Rep, 2020; 10; 9288
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.949682
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950225
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950627
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.950448
Most Viewed Current Articles
07 Dec 2021 : Case report  17,462,920
17,462,920
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  164,298
164,298
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
112,928
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
59,069
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133
Your Privacy
We use cookies to ensure the functionality of our website, to personalize content and advertising, to provide social media features, and to analyze our traffic. If you allow us to do so, we also inform our social media, advertising and analysis partners about your use of our website, You can decise for yourself which categories you you want to deny or allow. Please note that based on your settings not all functionalities of the site are available. View our privacy policy.
Your Privacy
We use cookies to ensure the functionality of our website, to personalize content and advertising, to provide social media features, and to analyze our traffic. If you allow us to do so, we also inform our social media, advertising and analysis partners about your use of our website, You can decise for yourself which categories you you want to deny or allow. Please note that based on your settings not all functionalities of the site are available. View our privacy policy.