29 July 2025: Articles 
Modified Piggy-Back Technique for Orthotopic Liver Transplantation in a 67-Year-Old Woman with Situs Inversus Totalis: A Case Report
Congenital defects / diseases
Wen-rui Wu ABCDEF 1, Li Pang A 1, Fa-peng Zhang B 1, Ming-bin Feng C 1, Lei-bo XuDOI: 10.12659/AJCR.948098
Am J Case Rep 2025; 26:e948098






Abstract
BACKGROUND: Situs inversus totalis (SIT) is a rare congenital condition characterized by complete mirror-image reversal of the thoracic and abdominal organs. This anatomical anomaly poses unique challenges for major abdominal surgeries, particularly liver transplantation, due to altered vascular and visceral orientation. While successful liver transplantations in patients with SIT have been reported, technical guidance remains limited.
CASE REPORT: We report a case of a 67-year-old woman with end-stage liver disease due to idiopathic cirrhosis and complete SIT. She had a prior splenectomy, hepatocellular carcinoma treated with transarterial chemoembolization, and a preoperative MELD score of 40. A full-size graft from a donation after brain death donor was used. The transplantation was performed using a modified piggy-back technique, without venovenous bypass. Due to reversed anatomy, a wide triangular end-to-side cavo-caval anastomosis was applied to ensure venous outflow. The graft was positioned in the left upper quadrant, without fixation. Vascular and biliary anastomoses were completed without tension or kinking. Total operative time was 485 min, with minimal blood loss. Postoperative recovery was uneventful, and the patient was discharged on day 77. Six-month follow-up revealed no complications.
CONCLUSIONS: Liver transplantation in patients with SIT is feasible and safe when appropriate technical modifications are used. The modified piggy-back technique provides a reliable solution for venous reconstruction and graft stability in the context of reversed anatomy.
Keywords: Liver Transplantation, Situs Inversus, end-stage liver disease, Humans, Female, Liver Transplantation, Aged, Situs Inversus, Anastomosis, Surgical, End stage liver disease
Introduction
Liver transplantation is a life-saving procedure for patients with end-stage liver disease but presents unique challenges when performed on individuals with anatomical variations. One such rare variation is situs inversus totalis (SIT), a condition in which the normal arrangement of thoracic and abdominal organs is completely reversed [1]. Although SIT is generally asymptomatic, its complete visceral inversion introduces significant difficulties in surgical orientation, vascular access, and organ positioning, especially during complex procedures, such as liver transplantation. In the setting of SIT, liver transplantation is further complicated by atypical vessel trajectories, mirrored biliary anatomy, and spatial mismatch within the abdominal cavity. These factors increase the risk of intraoperative graft malrotation, vascular kinking, and postoperative complications, such as hepatic vein outflow obstruction or biliary stricture.
Several prior case reports have described successful liver transplantation in patients with SIT, describing different approaches to overcome anatomical challenges. These include strategies for graft orientation, vascular reconstruction, and recipient vessel preparation. For instance, Sankarankutty et al proposed a simplified method using cavo-caval anastomosis in reversed orientation [2], and Tucker et al detailed specific graft positioning techniques to avoid venous outflow obstruction [3]. A recent review has summarized reported cases of adult liver transplantation in patients with SIT in tabular form, highlighting the various surgical strategies and clinical outcomes described in the literature [4].
In our patient, preoperative imaging and intraoperative exploration confirmed SIT, including a left-sided liver, right-sided spleen and stomach, and dextrocardia. Despite this reversed organ orientation, no vascular or biliary anomalies were identified.
Case Report
RECIPIENT AND DONOR CHARACTERISTICS:
The recipient was a 67-year-old female patient with complete SIT and a history of idiopathic liver cirrhosis. Over 20 years prior, she underwent splenectomy. In the previous 5 years, she experienced recurrent hand tremors, and in the previous year, she had episodes of melena. Five months prior to presentation, liver cancer was discovered, and she underwent 2 sessions of transarterial chemoembolization. Approximately 1.5 months prior to presentation, jaundice and anuria developed, requiring intensive care unit admission and evaluation for liver transplantation. She was 160 cm tall, weighed 67.5 kg, and had a body mass index of 26.4 kg/m2. Computed tomography (CT) imaging confirmed situs inversus with liver cirrhosis, portal hypertension, and 4 nodules in the left liver, suggestive of malignancy, with the largest measuring 28×24 mm (Figure 1). Cardiac ultrasound showed global heart enlargement and regional wall motion abnormalities. The diagnosis included liver failure, hepatic encephalopathy, gastrointestinal bleeding, liver malignancy, heart failure, and renal insufficiency, due to hepatorenal syndrome. The preoperative MELD score was 40. The full-size liver graft came from a 60-year-old male donor after brain death. The liver donation was posthumous and all organ donations were voluntary and altruistic.
SURGICAL PROCEDURE:
A Mercedes incision was used. Upon abdominal exploration, SIT was confirmed (Figure 2). Preoperative imaging and intraoperative exploration confirmed that, despite the mirrored anatomy, the hepatic artery (HA), portal vein (PV), and bile duct (BD) followed a typical configuration in their left-right reversed positions, with no associated vascular anomalies. The liver was markedly cirrhotic and atrophic, with extensive collateral circulation in the portal venous system. The mirrored anatomy introduced intraoperative orientation challenges. During explantation of the cirrhotic liver, particular care was required to identify and isolate vascular structures whose positions were reversed. The most technically demanding step was performing the caval anastomosis, which necessitated flipping the donor liver toward the patient’s left upper quadrant for optimal alignment. Other anastomoses proceeded smoothly once spatial relationships were adjusted. The porta hepatis was carefully dissected, and the HA, PV, and BD were ligated and divided. The recipient’s inferior vena cava (IVC) was preserved, and no vena-venous bypass was used. The donor structures, including the IVC, PV, and HA, were anastomosed to the corresponding recipient structures. A modified piggy-back technique was used, with a wide triangular end-to-side anastomosis of the IVC (Figure 3). The HA, PV, and BD were anastomosed end-to-end without tension. The liver graft was not fixed with sutures or devices. No T-tube or stent was used (Figure 4). Doppler ultrasound after surgery showed strong signals, and the liver appeared soft and healthy. The abdomen was successfully closed. The total surgical time was 485 min, with a cold ischemia time of 458 min and a clamping time of 67 min. Blood loss was approximately 400 mL.
The patient had an uneventful recovery after the transplant, with liver function approaching normal levels within 1 week. Urine output gradually resumed, and cardiac function improved. The patient was discharged on day 77 after surgery in good condition. Six months after transplantation, follow-up outpatient examinations showed normal results, with no vascular or biliary complications.
Compared with standard orthotopic liver transplantation, this case required specific technical modifications, due to the mirror-image anatomy of SIT. First, a modified piggy-back technique was used, involving a wide triangular end-to-side cavo-caval anastomosis to accommodate reversed venous orientation and ensure unobstructed outflow. Second, the donor liver was positioned with careful rotation toward the left upper quadrant, taking advantage of the space left by the right-sided stomach and spleen. No graft fixation was performed, as stability was achieved after vascular and biliary anastomoses. These adaptations allowed for safe anastomoses without tension or kinking, despite the reversed anatomy.
Discussion
This case provides practical insights into the technical planning and intraoperative decision-making required for successful liver transplantation in patients with SIT, which is a rare condition, with an incidence of approximately 1 in 10 000 [1]. Due to the complex congenital anatomical abnormalities present in SIT, liver transplantation in these patients presents unique technical challenges, and although early reports described it as a relative contraindication, due to technical difficulties, subsequent successful cases have demonstrated that it is no longer considered a contraindication per se [5,6]. To date, SIT remains rare, and experience with liver transplantation in adult recipients is limited. However, it is important to note that standard liver transplantation methods cannot be applied unchanged in patients with SIT. Several surgical modifications are required to accommodate the reversed anatomy, particularly in terms of graft positioning and vascular alignment.
Compared with the anatomy of the general population, the anatomical variations in patients with SIT often result in multiple vascular anomalies and organ malpositioning, including abnormal positioning and orientation of the liver graft and its vessels. When procuring the donor liver, it is essential to preserve the maximum length of the hepatic veins and the IVC, as well as to collect the iliac artery and vein grafts to ensure that all anastomoses can be adequately performed. The vascular and organ malpositioning in patients with SIT necessitate more precise and cautious anastomoses. Special attention must be paid to avoid twisting of the vessels during anastomosis, to prevent liver ischemia and other complications. Some authors have proposed using inflatable gastric balloons or tissue expanders to resolve vascular twisting, although these techniques remain experimental and their efficacy uncertain.
In the present case, to assess the positioning of the liver graft, we temporarily placed the donor liver into the surgical field and considered several potential positioning options: (1) rotating the donor liver 90° clockwise, positioning the anatomical right lobe in the recipient’s left upper abdomen [2]. In this configuration, the donor’s superior vena cava was anastomosed, and the IVC was connected to the recipient’s left IVC in an end-to-side technique. This method offered multiple advantages, including reducing pressure on the stomach from the right lobe of the liver, minimizing the risk of mismatched liver volume, preventing thrombus formation after venous anastomosis, and facilitating the anastomosis of the HA, PV, and BD. (2) A 180° counterclockwise rotation of the donor liver was performed from right to left, using reverse vena cava plasty [6]. (3) The standard orthotopic transplantation was performed [5]. The 2 main challenges of orthotopic liver transplantation in patients with SIT are, first, the requirement to position the larger right lobe of the donor liver over the right upper abdomen, and, second, the presence of a significant space in the left upper abdomen, which increases the risk of lateral displacement of the graft and torsion of the hepatic veins. The modified piggy-back technique was straightforward, quick, and most importantly, allowed the graft to be comfortably positioned in the left upper abdomen, avoiding vessel twisting or kinking and ensuring optimal venous drainage. Moreover, it provided flexibility in positioning the graft during HA and PV reconstruction. Given the patient’s prior splenectomy and after multiple attempts, orthotopic liver transplantation with the modified piggy-back technique was ultimately selected. After reconstructing the IVC, the HA, PV, and BD were all successfully anastomosed end-to-end without tension.
Several previous case reports have described different techniques for managing liver transplantation in patients with SIT. Tucker et al emphasized graft rotation strategies to optimize venous outflow and reduce torsion risk [3], while Sankarankutty et al reported success using a reversed cavo-caval anastomosis in a counter-rotated graft [2]. In contrast, we selected a standard orthotopic positioning combined with a modified piggy-back technique, which avoided excessive graft rotation and allowed the liver to be placed securely in the left upper quadrant. This approach simplified anastomosis, preserved normal anatomic relationships, and minimized the risk of kinking, particularly in a patient without vascular anomalies. The uneventful postoperative recovery and good short-term graft function observed in our patient are consistent with those reported in previous successful SIT transplantations [2,6].
In standard piggy-back liver transplantation, the donor’s suprahepatic IVC is anastomosed side-to-side with the recipient’s hepatic vein confluence. In this case, we used a modified version involving a wide, triangulated end-to-side cavo-caval anastomosis, which better accommodated the reversed venous anatomy of the patient with SIT. This approach ensured unobstructed hepatic venous outflow while maintaining graft stability, and minimized the risk of torsion or kinking associated with mirror-image orientation.
The choice between orthotopic positioning, 90° clockwise rotation, or 180° reverse orientation should be based on intraoperative findings. It depends on whether the graft fits well in the recipient’s cavity, whether vascular anastomoses can be performed without tension or kinking, and whether there is a risk of torsion.
Despite successful outcomes, liver transplantation in SIT carries unique risks. Intraoperative complications include graft malposition, hepatic vein outflow obstruction due to torsion, and difficulties in aligning arterial and biliary structures. Postoperatively, the risk of biliary stricture, venous thrombosis, and graft congestion that can be elevated due to subtle mismatches in anatomical orientation. Long-term follow-up is essential to monitor vascular patency and biliary drainage in such complex reconstructions.
Conclusions
This report demonstrates that liver transplantation in patients with SIT can be safely performed using technical adaptations tailored to reversed anatomy. The modified piggy-back technique proved effective for achieving stable graft positioning and tension-free venous outflow, supporting its applicability in complex anatomical variants.
Figures
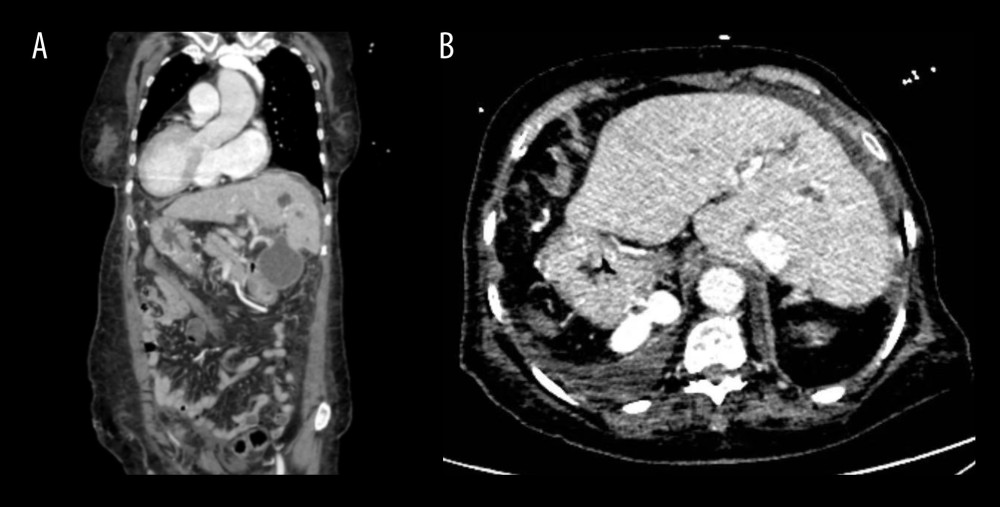 Figure 1. Preoperative imaging demonstrating situs inversus totalisThe left panel shows a coronal computed tomography view, and the right panel shows an axial view. The liver is visualized on the left side and the spleen on the right, consistent with complete mirror-image reversal of thoracic and abdominal organs.
Figure 1. Preoperative imaging demonstrating situs inversus totalisThe left panel shows a coronal computed tomography view, and the right panel shows an axial view. The liver is visualized on the left side and the spleen on the right, consistent with complete mirror-image reversal of thoracic and abdominal organs. 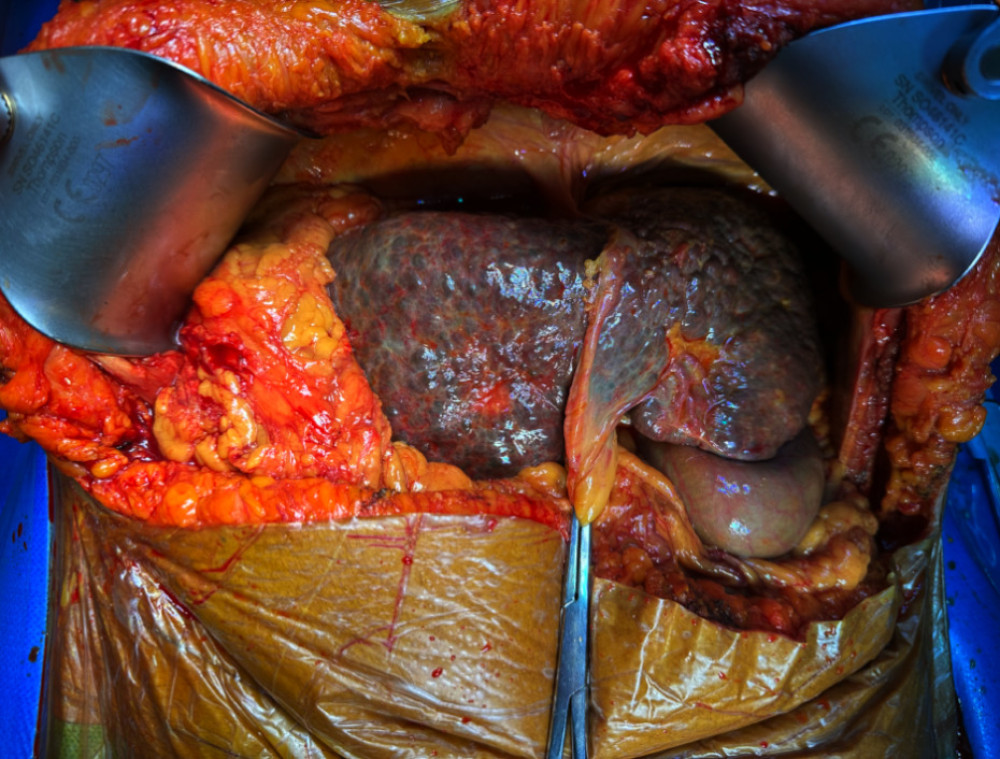 Figure 2. Intraoperative confirmation of situs inversus totalisSurgical view showing reversed organ orientation, with the liver located in the left upper quadrant and the stomach and spleen on the right. No vascular anomalies were observed.
Figure 2. Intraoperative confirmation of situs inversus totalisSurgical view showing reversed organ orientation, with the liver located in the left upper quadrant and the stomach and spleen on the right. No vascular anomalies were observed. 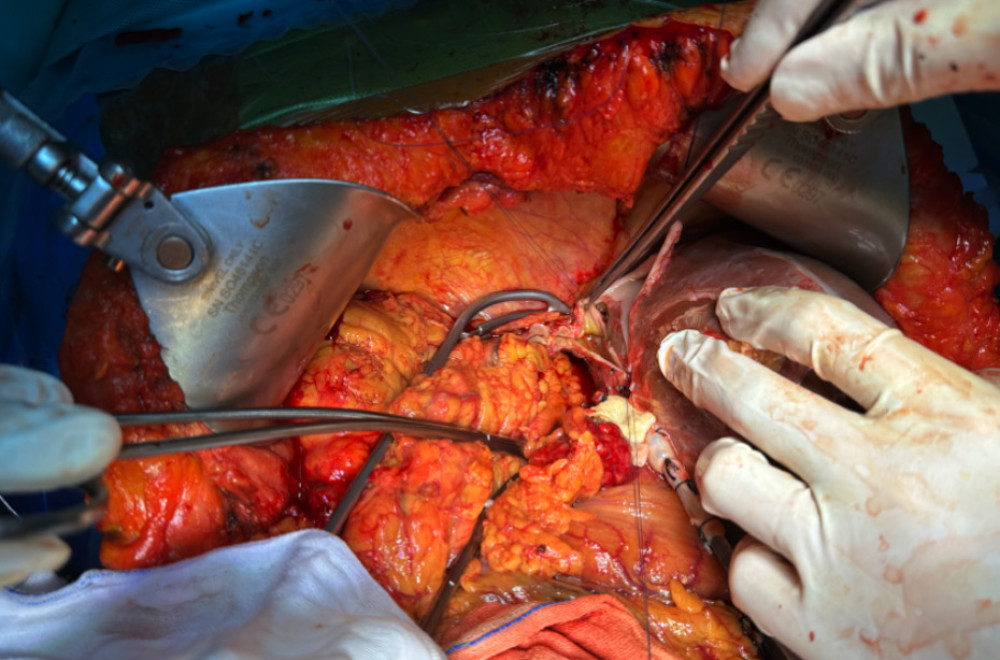 Figure 3. Modified piggy-back technique for venous outflow reconstructionThe donor suprahepatic inferior vena cava was anastomosed to the recipient inferior vena cava in an end-to-side fashion using a wide triangular opening, allowing for tension-free venous drainage in the context of reversed anatomy.
Figure 3. Modified piggy-back technique for venous outflow reconstructionThe donor suprahepatic inferior vena cava was anastomosed to the recipient inferior vena cava in an end-to-side fashion using a wide triangular opening, allowing for tension-free venous drainage in the context of reversed anatomy. 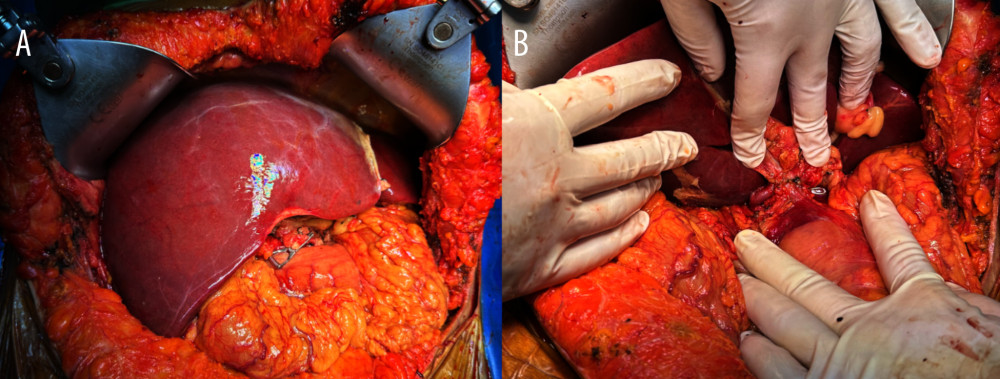 Figure 4. Biliary reconstruction and final graft positioning(A) Intraoperative view of the donor liver prior to bile duct reconstruction. (B) Final view of the hepatic hilum showing completed anastomoses of the hepatic artery, portal vein, and bile duct, with no signs of twisting or compression.
Figure 4. Biliary reconstruction and final graft positioning(A) Intraoperative view of the donor liver prior to bile duct reconstruction. (B) Final view of the hepatic hilum showing completed anastomoses of the hepatic artery, portal vein, and bile duct, with no signs of twisting or compression. References
1. Eitler K, Bibok A, Telkes G, Situs inversus totalis: Int J Gen Med, 2022; 15; 2437-49
2. Sankarankutty AK, Cagnolati D, Kemp R, How to do liver transplantation in situs inversus totalis: ANZ J Surg, 2015; 85(3); 187-88
3. Tucker O, Prachalias A, Kane P, Rela M, Graft positioning at liver transplantation in situs inversus: Liver Transpl, 2006; 12(11); 1720-22
4. Shamsaeefar A, Masjedi F, Roozbeh J, Liver and pancreas transplantation in adult donor and recipients with situs inversus totalis: J Med Case Rep, 2024; 18(1); 398
5. Na BG, Hwang S, Ahn CS, Deceased donor liver transplantation in an adult recipient with situs inversus totalis: Ann Hepatobiliary Pancreat Surg, 2020; 24(3); 319-25
6. Rayhill SC, Scott D, Orloff S, Orthotopic, but reversed implantation of the liver allograft in situs inversus totalis – a simple new approach to a difficult problem: Am J Transplant, 2009; 9(7); 1602-6
Figures
Figure 1. Preoperative imaging demonstrating situs inversus totalisThe left panel shows a coronal computed tomography view, and the right panel shows an axial view. The liver is visualized on the left side and the spleen on the right, consistent with complete mirror-image reversal of thoracic and abdominal organs.Figure 2. Intraoperative confirmation of situs inversus totalisSurgical view showing reversed organ orientation, with the liver located in the left upper quadrant and the stomach and spleen on the right. No vascular anomalies were observed.Figure 3. Modified piggy-back technique for venous outflow reconstructionThe donor suprahepatic inferior vena cava was anastomosed to the recipient inferior vena cava in an end-to-side fashion using a wide triangular opening, allowing for tension-free venous drainage in the context of reversed anatomy.Figure 4. Biliary reconstruction and final graft positioning(A) Intraoperative view of the donor liver prior to bile duct reconstruction. (B) Final view of the hepatic hilum showing completed anastomoses of the hepatic artery, portal vein, and bile duct, with no signs of twisting or compression. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133