22 July 2025: Articles 
Leukemoid Reactions in Pancreatic Cancer: A Case Series
Challenging differential diagnosis, Management of emergency care, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Teng Huang BCDE 1, Tangchun Liu BCD 1, Siqi Liu BC 1, Zhengfei Yang AE 1*DOI: 10.12659/AJCR.948491
Am J Case Rep 2025; 26:e948491






Abstract
BACKGROUND: This article presents a rare case of pancreatic cancer complicated by a leukemoid reaction, alongside 4 similar cases treated at our hospital between 2016 and 2024. Leukemoid reactions are uncommon paraneoplastic manifestations, and their optimal management remains undefined. Herein, we systematically analyze the clinical characteristics and potential molecular mechanisms involved in the development and progression of tumor-associated leukemoid reactions, and summarize our diagnostic and therapeutic approaches.
CASE REPORT: We reviewed the records of 5 patients at our hospital who had malignancies complicated by leukemoid reactions. Medical histories, laboratory tests, imaging findings, bone marrow biopsy results, and treatment details were collected and analyzed. We explored the pathogenesis, diagnostic strategies, and treatment modalities for leukemoid reactions. A 52-year-old man with advanced pancreatic adenocarcinoma and a KRAS p.G12D mutation, developed extreme leukocytosis (96.22×10⁹ white blood cells/L) in the context of hepatic metastases. Despite broad-spectrum antimicrobial coverage, cytoreductive therapies, and supportive measures (bilirubin adsorption and plasma exchange, continuous veno-venous hemofiltration), his condition rapidly deteriorated, culminating in multi-organ failure. The 4 additional patients – 1 each with metastatic breast cancer, colon cancer, cholangiocarcinoma, and recurrent pancreatic cancer – exhibited similarly aggressive courses, with only transient stabilization observed in the breast cancer case.
CONCLUSIONS: Patients with malignancies complicated by leukemoid reaction generally have a poor prognosis. Clinicians should be alert to markedly elevated white blood cell counts, promptly investigate underlying causes, and initiate individualized treatments. Future research should focus on the molecular mechanisms driving the development and progression of leukemoid reactions and therapeutic interventions to enhance patient survival and clinical outcomes.
Keywords: Diagnosis, Leukemia, Pancreatic Neoplasms, Humans, Male, Middle Aged, Leukemoid Reaction, Adenocarcinoma, Female, Liver Neoplasms
Introduction
A leukemoid reaction is defined as a marked increase in peripheral white blood cell (WBC) counts, exceeding 50×109/L, due to non-leukemic factors, with no clonal features indicative of leukemia. Infection is the most common cause of leukemoid reactions, but when the leukemoid reaction is induced by a malignancy, it often implies advanced disease and portends a poor prognosis [1]. Although malignancies are not the most prevalent cause of leukemoid reactions, reports have documented leukemoid reactions associated with lung cancer, colorectal cancer, and melanoma [2–6]. However, leukemoid reactions concurrent with pancreatic cancer are rarely reported – no clear incidence data are available – and only 3 cases have been documented to date [7–9].
Herein we describe a rare case of pancreatic cancer complicated by a leukemoid reaction, and analyze the clinical features, diagnostic challenges, and therapeutic considerations. We also incorporate 4 additional cases treated at our hospital, together with a relevant literature review, to provide a reference for future clinical practice and research.
Case Report
PATIENT INFORMATION:
A 52-year-old man (Patient A in Table 1) was admitted to our hospital on 10 October 2024, with a 1-year history of pancreatic cancer. He presented with progressive abdominal distension and jaundice for the preceding 10 days.
PREVIOUS DIAGNOSIS AND TREATMENT:
In October 2023, the patient had unexplained abdominal distension and radiating back pain that worsened at night. After inadequate symptom relief at a local hospital, he was referred to our facility. Computed tomography (CT) imaging revealed a lesion in the pancreatic head, and laparoscopic biopsy confirmed pancreatic cancer (T4N/M1) with a
DISEASE RECURRENCE:
In July 2024, the disease recurred with newly discovered hepatic metastases. The patient underwent laparoscopic partial hepatectomy, and postoperative pathology revealed a poorly differentiated adenocarcinoma. Subsequently, he continued on NALIRIFOX chemotherapy without notable disease progression. In October 2024, the patient was admitted again with markedly increased abdominal distention and jaundice, accompanied by fatigue. On admission, the patient’s highest recorded axillary temperature was 37.2°C on admission and never exceeded 37.5°C during hospitalization. Laboratory tests showed a WBC count of 96.22×109/L (Figure 1) with 93% neutrophils, hemoglobin 78 g/L, platelet count 67×109/L, procalcitonin (PCT) 11.99 ng/mL, and C-reactive protein 126 mg/L, alongside severe liver function impairment (alanine transaminase (ALT) was 438 U/L, aspartate transaminase (AST) was 749 U/L, gamma-glutamyl transferase (GGT) was 194 U/L, alkaline phosphatase (ALP) was 338 U/L, total bilirubin was 121.4 μmol/L, direct bilirubin was 60.7 μmol/L); CT imaging demonstrated diffuse intra-/extra-hepatic duct dilation caused by extensive metastatic compression rather than a focal, drainable obstruction; and severely compromised coagulation [prothrombin time (PT) was 31.9 s, international normalized ratio (INR) was 2.91].
A bone marrow biopsy confirmed active myeloid hyperplasia without leukemic features, consistent with leukemoid reaction (Figure 2). Between July and October 2024, serial tumor-marker measurements demonstrated a parallel rise in several indicators of tumor burden: carcinoembryonic antigen increased from 11.3 ng/mL to 19.4 ng/mL, CA-125 from 54.8 U/mL to 519 U/mL, CYFRA21-1 from 1.85 ng/mL to 38.7 ng/mL, and neuron-specific enolase from 8.8 ng/mL to 356 ng/mL, whereas CA 19-9 remained below 2 U/mL and alpha fetoprotein stayed within the normal range. These escalating values closely paralleled the progression of hepatic metastases and the sharp surge in leukocyte counts. Despite broad-spectrum antibiotics (piperacillin-tazobactam), liver-protection therapy, fresh-frozen plasma transfusion, and bilirubin adsorption plus plasma exchange, the patient’s condition deteriorated rapidly.
On admission (Day 0, 10 October 2024), the patient had already met the criteria for acute liver failure, with severe metabolic acidosis and a leukemoid reaction; on the second day of admission (Day 1, 11 October 2024), AST exceeded 7000 U/L, INR rose to 5.94, and lactate to 16 mmol/L; creatinine climbed to 200 μmol/L with oliguria, prompting continuous veno-venous hemofiltration. Platelets fell to 39×109/L and fibrinogen to 1.13 g/L, consistent with disseminated intravascular coagulation (DIC).
On Day 2 (12 October 2024), the patient developed hypoxemic respiratory failure that required tracheal intubation and mechanical ventilation. Serum bilirubin remained markedly elevated and both GGT and ALP were high. Together with CT evidence of diffuse intra- and extra-hepatic bile-duct compression by bulky metastases, these findings indicated an intra-hepatic mixed cholestasis secondary to massive tumor infiltration, rather than a discrete, drainable obstruction. Because severe coagulopathy made endoscopic or percutaneous drainage hazardous, our team elected bilirubin adsorption and plasma exchange as a temporizing measure to limit cholangitis risk. Despite bilirubin adsorption and plasma exchange, continuous veno-venous hemofiltration and vaso-active support, the patient’s lactic acidosis remained refractory and hypotension progressed, culminating in multi-organ failure.
On Day 3 (13 October 2024), the patient suffered cardiocirculatory arrest, and resuscitation was declined by the family. The immediate cause of death was multi-organ failure dominated by fulminant hepatic failure secondary to massive hepatic metastasis, compounded by DIC, acute kidney injury, and suspected cholangitic sepsis.
In clinical practice, cases of tumor-associated leukemoid reaction have complex etiologies, and are often correlated with poor outcomes. To further investigate such presentations, we reviewed 4 additional patients – each with a different tumor type – who also experienced leukemoid reactions. We summarized the clinical manifestations, laboratory findings, diagnostic procedures, treatments, and outcomes for all 5 patients in Table 1.
Discussion
Overview of Leukemoid Reaction Cases in Our Hospital and Comparison with the Literature
CLINICAL FEATURES AND PROGNOSIS:
In addition to the pancreatic cancer case described herein, our hospital has managed 4 other cancer patients with leukemoid reactions: a patient with multiple metastases following breast cancer surgery, another with multiple metastases after combined treatment for splenic flexure colon cancer, another with cholangiocarcinoma complicated by cirrhosis, and another with recurrent pancreatic cancer post-surgery. These patients shared several features: peripheral WBC counts exceeding 50×109/L at diagnosis, bone marrow biopsy ruling out leukemia, and the fact that most were in advanced or metastatic stages.
Clinically, they exhibited marked leukocytosis alongside organ dysfunction (eg, liver failure, coagulopathy). Despite receiving antitumor, anti-infective, and multidisciplinary supportive therapies, most of these patients had poor outcomes. Only the patient with breast cancer showed a transient decline in WBC count and short-term stability following supportive care. This finding aligns with previous reports indicating that the presence of a tumor-associated leukemoid reaction usually suggests advanced or highly aggressive malignancies, with generally poor prognoses [1–9].
RARITY OF LEUKEMOID REACTION IN PANCREATIC CANCER: Tumor-associated leukemoid reaction is most commonly associated with lung cancer, colorectal cancer, and melanoma [2–6]. Few cases of pancreatic cancer complicated by leukemoid reaction have been reported [7–9]. In our current case and in another patient [7] with recurrent pancreatic cancer, extreme leukocytosis appeared in the late stage of the disease. This suggests that, upon progression to liver metastasis or widespread dissemination, pancreatic cancer cells may induce excessive proliferation of myeloid cells through the secretion of factors like granulocyte colony-stimulating factor (G-CSF), consistent with other case reports [8].
PROGNOSTIC OUTLIER: THE BREAST CANCER CASE: Paraneoplastic leukemoid reaction usually heralds a fatal course – 76% of patients die within 12 weeks [16] – and 4 of our 5 cases conformed to this pattern. The sole exception was the breast cancer patient, whose leukocyte count fell and disease stabilized. Two biologic features likely explain this respite. First, the tumor was hormone-receptor-positive (luminal) rather than triple-negative; luminal cancers grow more slowly and offer more therapeutic targets, whereas triple-negative breast cancer progresses rapidly and drives stronger granulocyte-stimulating-factor release [17]. Second, lower immunogenicity and intra-tumor heterogeneity in luminal disease may reduce pro-leukemoid cytokine output and enhance endocrine or chemotherapy responsiveness, allowing transient control of both tumor burden and WBC surge [18]. By contrast, the pancreatic cancer, colon cancer, and cholangiocarcinoma cases in our series lacked comparable treatment leverage and progressed unabated. This case underscores how intrinsic subtype and heterogeneity can modulate leukemoid reaction behavior and short-term prognosis.
CLINICAL SIGNIFICANCE:
Based on our cases and the literature, an unexplained surge in leukocyte count – especially for counts exceeding 50×109/L, and after excluding infections and other common causes – warrants a high index of suspicion for tumor-related leukemoid reaction. Once leukemia is ruled out via bone marrow examination and relevant genetic tests, a definitive diagnosis can be established. Given that leukemoid reaction often indicates aggressive tumor behavior in pancreatic cancer, early assessment of liver function, coagulation status, and metastatic progression is vital. The breast cancer “prognostic outlier” in our series illustrates that when the underlying tumor is both biologically less aggressive (hormone-receptor-positive, luminal subtype) and amenable to systemic therapy, successful disease control can be accompanied by a pronounced fall in leukocyte count and transient clinical stabilization. However, rapid tumor progression or multiple-organ failure is often fatal.
MECHANISMS OF LEUKEMOID REACTION INDUCTION AND THEIR RELEVANCE TO THE PRESENT CASES:
Prior studies suggest that malignant tumors can secrete various cytokines (eg, G-CSF, IL-6) that activate pathways such as JAK/STAT, inducing excessive proliferation of myeloid progenitor cells [10–15]. These mechanisms of leukemoid reaction induction, primarily inferred from basic research and limited case studies, still lack large-scale clinical validation.
In our cohort, serum G-CSF or IL-6 levels were not routinely measured, preventing direct confirmation of their roles in leukemoid reaction. Clinically, however, we noted that extreme leukocytosis often accompanied marked tumor burden or recurrence. Conversely, once the tumor was relatively well controlled, WBC counts tended to decline. This observation suggests that tumor-derived cytokines may critically influence leukemoid reaction development.
Future research should incorporate comprehensive cytokine monitoring and correlate these data with imaging, pathology, and therapeutic responses to clarify the cellular processes underlying leukemoid reactions in pancreatic and other gastrointestinal cancers, as well as to explore targeted interventions.
EARLY RECOGNITION AND DIFFERENTIAL DIAGNOSIS: In malignant tumor patients who present with a rapid rise in peripheral WBC count (>50×109/L), common causes (eg, infection, leukemia) must be excluded first [1,13]. Bone marrow biopsy and genetic tests (eg, the BCR-ABL1 fusion gene) are critical for ruling out myeloproliferative disorders.
ANTIMICROBIAL THERAPY: True paraneoplastic leukemoid reactions do not improve with antibiotics, so the definitive treatment remains tumor control [13]. Nevertheless, advanced-cancer patients who are functionally immunosuppressed – eg, recent multi-agent chemotherapy, acute liver failure, DIC, and hypoalbuminemia as in our index case – require early empiric broad-spectrum cover while occult infection is excluded, in line with sepsis guidance [19]. In Case 1, strong inflammatory markers (PCT 11.99 ng/mL, CRP 126 mg/L) and cholestatic jaundice prompted empiric piperacillin-tazobactam in accordance with international guidelines. The Tokyo Guidelines for Cholangitis [20] endorse first-line agent use for suspected biliary sepsis. The WBC fell from 96.2×109/L to 57.5×109/L after 3 doses, confirming a partial infectious component. However, persistent leukocytosis >50×109/L reflected the ongoing paraneoplastic drive. The practical approach in our clinical practice was to: (i) obtain cultures and inflammatory biomarkers promptly; (ii) initiate guideline-directed empiric antibiotics only when clinical or laboratory features suggest infection; and (iii) narrow or discontinue treatment once cultures are negative and the patient is stable, recognizing that persistent leukocytosis may indicate a leukemoid reaction rather than therapeutic failure.
COMPREHENSIVE TREATMENT STRATEGY: Because a leukemoid reaction often reflects advanced or highly aggressive tumor progression, prompt multidisciplinary collaboration is crucial. Treatment options may include chemotherapy, immunotherapy, targeted therapy, or cytoreductive surgery, accompanied by supportive measures such as anti-infective therapy, correction of electrolyte imbalances, organ function maintenance, and thrombosis prevention [4,11,14].
FUTURE RESEARCH DIRECTIONS:
Establishing monitoring models to dynamically assess the relationship between cytokine levels (eg, G-CSF, IL-6), leukocyte counts, and tumor burden will be essential. Investigating potential new targets for specifically blocking tumor-associated leukemoid reaction could further enhance survival and quality of life.
Conclusions
Pancreatic cancer complicated by leukemoid reaction is relatively rare but generally exhibits an aggressive clinical course and poor prognosis. Findings from the present case, along with 4 other similar cases at our hospital, indicate that when a cancer patient shows marked leukocytosis, early bone marrow and genetic testing are essential to exclude leukemia, and tumor progression-related leukemoid reaction should be considered. For high-risk populations, timely multidisciplinary intervention and enhanced monitoring may offer some improvement in outcomes. Further investigation into cytokines such as G-CSF is needed to strengthen the evidence base for accurate diagnosis and targeted treatment of this condition.
Figures
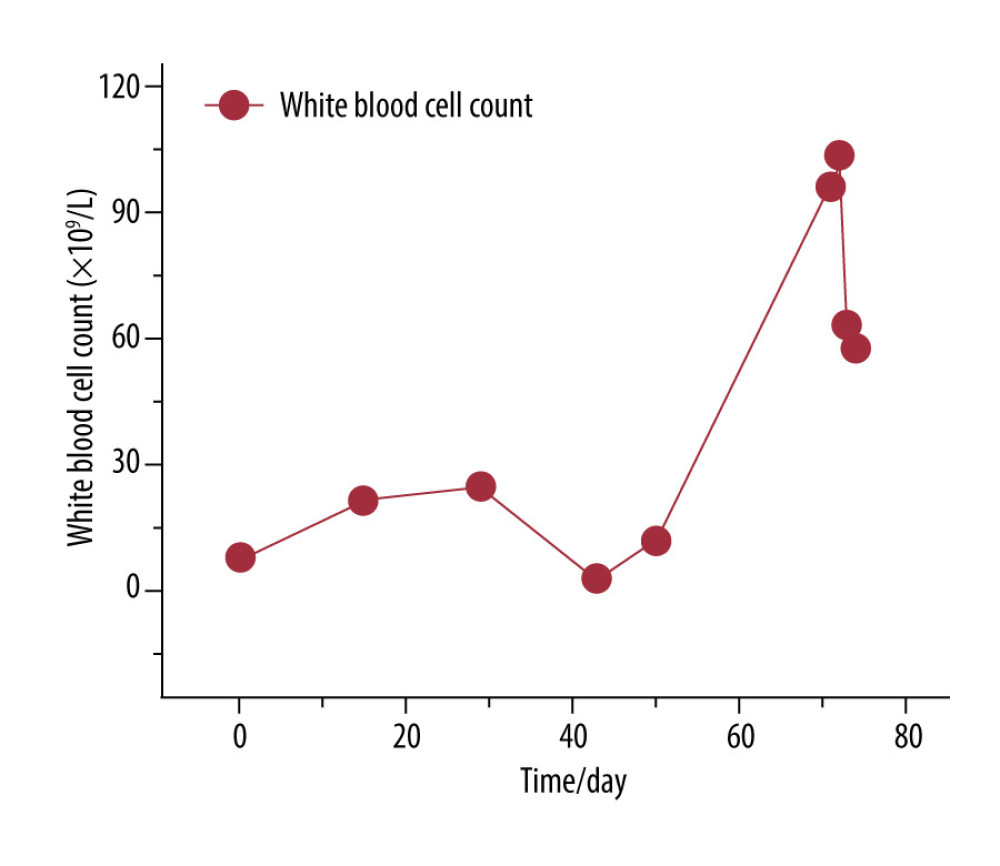 Figure 1. White blood cell (WBC) count in Patient A. The x-axis (Time/day) represents days since 31 July 2024 (Day 0), when hepatic metastases were first identified. The y-axis indicates the WBC count (×109/L). An initial rise in WBC count was observed from Day 0 to Day 30, followed by partial stabilization, then a marked increase after Day 51, corresponding to disease progression and clinical deterioration.
Figure 1. White blood cell (WBC) count in Patient A. The x-axis (Time/day) represents days since 31 July 2024 (Day 0), when hepatic metastases were first identified. The y-axis indicates the WBC count (×109/L). An initial rise in WBC count was observed from Day 0 to Day 30, followed by partial stabilization, then a marked increase after Day 51, corresponding to disease progression and clinical deterioration. 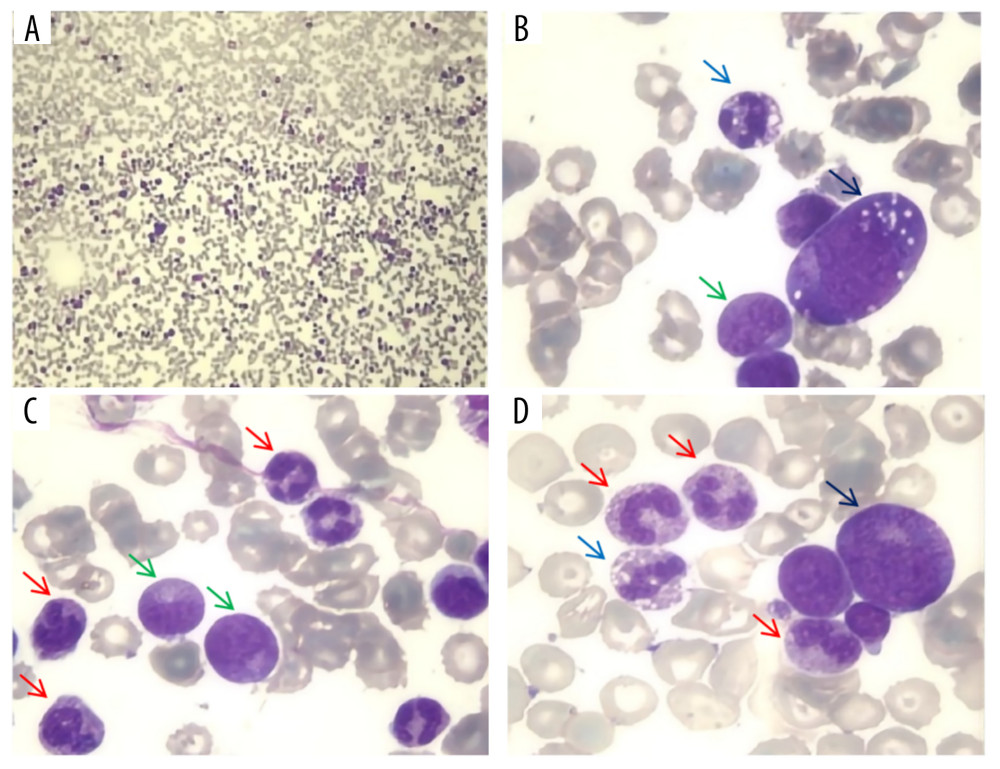 Figure 2. Bone marrow biopsy in Patient A. Under 4× magnification (A), a high cell density was observed, with prominent granulocytic proliferation – predominantly neutrophils – indicating active myeloid hyperplasia. The remaining images at 40× magnification (B–D) reveal an increased number of segmented neutrophils (red arrows), some exhibiting vacuolation (blue arrows), along with metamyelocytes (green arrows) and promyelocytes (black arrows). Overall, the bone marrow demonstrated active hematopoiesis with marked proliferation of segmented and immature granulocytes, without any abnormal increase in blasts or nuclear atypia. Key diagnostic features of a leukemoid reaction include a markedly elevated neutrophil count and reduced but morphologically normal erythroid lineage cells, in contrast to leukemia, which typically shows a high proportion of blasts and aberrant nuclear chromatin. The annotations showing segmented neutrophils, neutrophil vacuolation, and immature granulocytes clearly illustrate microscopic hallmarks of a leukemoid reaction, supporting the clinical diagnosis.
Figure 2. Bone marrow biopsy in Patient A. Under 4× magnification (A), a high cell density was observed, with prominent granulocytic proliferation – predominantly neutrophils – indicating active myeloid hyperplasia. The remaining images at 40× magnification (B–D) reveal an increased number of segmented neutrophils (red arrows), some exhibiting vacuolation (blue arrows), along with metamyelocytes (green arrows) and promyelocytes (black arrows). Overall, the bone marrow demonstrated active hematopoiesis with marked proliferation of segmented and immature granulocytes, without any abnormal increase in blasts or nuclear atypia. Key diagnostic features of a leukemoid reaction include a markedly elevated neutrophil count and reduced but morphologically normal erythroid lineage cells, in contrast to leukemia, which typically shows a high proportion of blasts and aberrant nuclear chromatin. The annotations showing segmented neutrophils, neutrophil vacuolation, and immature granulocytes clearly illustrate microscopic hallmarks of a leukemoid reaction, supporting the clinical diagnosis. 
References
1. Potasman I, Grupper M, Leukemoid reaction: spectrum and prognosis of 173 adult patients: Clin Infect Dis, 2013; 57(11); e177-e81
2. Abukhiran I, Mott SL, Bellizzi AM, Boukhar SA, Paraneoplastic leukemoid reaction: Case report and review of the literature: Pathol Res Pract, 2021; 217; 153295
3. Chahine Z, Samhouri Y, Jayakrishnan T, Monga D, Leukemoid reaction causing arterial thrombus in a patient with lung adenocarcinoma: BMJ Case Rep, 2020; 13(10); e235389
4. Ellison TA, Mandal K, Leukemoid reaction: Case report: J Thorac Cardiovasc Surg, 2018; 155(4); e117-e18
5. Kasuga I, Makino S, Kiyokawa H, Tumor-related leukocytosis is linked with poor prognosis in patients with lung carcinoma: Cancer, 2001; 92(9); 2399-405
6. Zhang XW, Wald A, Salzmann M, Cytokine alterations during paraneoplastic neutrophilia and leukemoid reaction in patients with advanced melanoma: Cancer Immunol Immunother, 2023; 72(2); 509-13
7. Dos Santos M, Bouhier K, Dao M-T, Paraneoplastic leukemoid reaction in pancreatic cancer: A case report: World J Gastrointest Oncol, 2015; 7(10); 259-62
8. Joshita S, Nakazawa K, Sugiyama Y, Granulocyte-colony stimulating factor-producing pancreatic adenosquamous carcinoma showing aggressive clinical course: Intern Med, 2009; 48(9); 687-91
9. Qureshi KM, Raman AK, Tan D, Fakih MG, Leukemoid reaction in pancreatic cancer: A case report and review of the literature: J Pancreas, 2006; 7(6); 631-34
10. Azzam O, Hewavitharana CH, Fermoyle S, Prentice D, Paraneoplastic leukemoid reaction in a localised squamous cell oesophageal cancer with paracrine G-CSF production: BMJ Case Rep, 2020; 13(10); e235069
11. Zhao H, Wu L, Yan G, Inflammation and tumor progression: Signaling pathways and targeted intervention: Signal Transduct Target Ther, 2021; 6(1); 263
12. Lou E, Goodwin J, Howell DN, A G-CSF-secreting adrenal carcinoma with rhabdoid-like differentiation causing leukocytosis: Nature Rev Urol, 2009; 6(7); 392-97
13. Sakka V, Tsiodras S, Giamarellos-Bourboulis EJ, Giamarellou H, An update on the etiology and diagnostic evaluation of a leukemoid reaction: Eur J Intern Med, 2006; 17(6); 394-98
14. Wilcox RA, Cancer-associated myeloproliferation: Old association, new therapeutic target: Mayo Clin Proc, 2010; 85(7); 656-63
15. Izumo W, Furukawa K, Katsuragawa H, Granulocyte-colony stimulating factor-producing gallbladder carcinoma-include analysis all case reports: A case report: Int J Surg Case Rep, 2016; 21; 87-90
16. Granger JM, Kontoyiannis DP, Etiology and outcome of extreme leukocytosis in 758 nonhematologic cancer patients: A retrospective, single-institution study: Cancer, 2009; 115(17); 3919-23
17. Stanton SE, Adams S, Disis ML, Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes: A systematic review: JAMA Oncol, 2016; 2(10); 1354-60
18. Zhang A, Miao K, Sun H, Deng CX, Tumor heterogeneity reshapes the tumor microenvironment to influence drug resistance: Int J Biol Sci, 2022; 18(7); 3019-33
19. Evans L, Rhodes A, Alhazzani W, Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021: Intensive Care Med, 2021; 47(11); 1181-47
20. Miura F, Okamoto K, Takada T, Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis: J Hepatobiliary Pancreat Sci, 2018; 25(1); 31-40
Figures
Figure 1. White blood cell (WBC) count in Patient A. The x-axis (Time/day) represents days since 31 July 2024 (Day 0), when hepatic metastases were first identified. The y-axis indicates the WBC count (×109/L). An initial rise in WBC count was observed from Day 0 to Day 30, followed by partial stabilization, then a marked increase after Day 51, corresponding to disease progression and clinical deterioration.Figure 2. Bone marrow biopsy in Patient A. Under 4× magnification (A), a high cell density was observed, with prominent granulocytic proliferation – predominantly neutrophils – indicating active myeloid hyperplasia. The remaining images at 40× magnification (B–D) reveal an increased number of segmented neutrophils (red arrows), some exhibiting vacuolation (blue arrows), along with metamyelocytes (green arrows) and promyelocytes (black arrows). Overall, the bone marrow demonstrated active hematopoiesis with marked proliferation of segmented and immature granulocytes, without any abnormal increase in blasts or nuclear atypia. Key diagnostic features of a leukemoid reaction include a markedly elevated neutrophil count and reduced but morphologically normal erythroid lineage cells, in contrast to leukemia, which typically shows a high proportion of blasts and aberrant nuclear chromatin. The annotations showing segmented neutrophils, neutrophil vacuolation, and immature granulocytes clearly illustrate microscopic hallmarks of a leukemoid reaction, supporting the clinical diagnosis. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133