25 July 2025: Articles 
Distinguishing Wernicke Encephalopathy from Artery of Percheron Infarction in a 43-Year-Old Man: A Case Report
Unusual clinical course, Challenging differential diagnosis
Syed Raza ABCDEF 1, Salma Mohamed AB 2,3, Nazia Naz S. Khan ABCDEF 2,3*DOI: 10.12659/AJCR.948636
Am J Case Rep 2025; 26:e948636






Abstract
BACKGROUND: Wernicke’s encephalopathy (WE) and Artery of Percheron (AOP) infarction share overlapping presentations, including mental status changes, ocular-motor signs, and similar thalamic MRI findings; but require distinct time-sensitive treatment, making prompt differentiation critical. WE results from thiamine deficiency, often due to alcohol use, causing oxidative damage in highly metabolically active brain regions. In contrast, an AOP infarction results from thrombotic occlusion of a rare perforating artery. The aim of this case report is to delineate the similarities and differences between WE and AOP infarction and to underscore the importance of early empiric thiamine replacement.
CASE REPORT: A 43-year-old man presented with altered mental status, fever, and generalized weakness. Non-contrast head computed tomography (CT) showed cerebellar hypoattenuation, prompting activation of a code stroke. The lesion was later deemed artifactual, and he was admitted for further evaluation. The following morning, the patient’s condition acutely changed, with new oculomotor abnormalities and worsening right lower extremity weakness. An urgent brain MRI demonstrated symmetric hyperintensities in the medial thalami. Uncertain whether the lesions represented an AOP infarction or WE, the team ordered a serum thiamine analysis, which returned low. Intravenous thiamine was initiated, resulting in rapid clinical improvement, and confirming WE as the final diagnosis.
CONCLUSIONS: WE can closely mimic AOP infarction both on clinical presentation and on radiologic appearance. High-dose thiamine is a low-risk, potentially lifesaving intervention, particularly when initial CT imaging is nondiagnostic and further imaging is pending. Empiric thiamine administration is especially warranted if MRI shows bilateral thalamic lesions of uncertain etiology.
Keywords: Stroke, Thiamine Deficiency, Wernicke Encephalopathy, cerebral infarction, Magnetic Resonance Imaging, Case Reports, Humans, Male, adult, Diagnosis, Differential, thiamine, Tomography, X-Ray Computed
Introduction
Thiamine is a naturally occurring vitamin found in grains, meats, fish, legumes, and other foods. It is essential for life, especially for brain function. Wernicke encephalopathy (WE) is an acute neurological emergency caused by a thiamine (vitamin B1) deficiency, associated with a mortality rate of 20% and the development of Korsakoff syndrome in 85% of survivors [1]. Based on postmortem autopsy studies, WE prevalence is 1–2% in the general population and 12–14% in patients with alcohol use disorder [1]. While clinicians most commonly encounter WE in the context of a patient with alcohol use disorder, other associated conditions include cancer, gastrointestinal surgery, and hyperemesis gravidarum [2]. Diagnosis is made clinically in patients presenting with 2 out of 4 of the Caine criteria: oculomotor abnormalities, cerebellar dysfunction, altered mental status or memory impairment, and dietary deficiency [3]. Magnetic resonance imaging (MRI) can also be used to support the diagnosis. Signs indicating WE include symmetric hyperintense T2 alterations in the medial thalami, periaqueductal gray matter, mamillary bodies, and tectal plate [4].
The pathophysiology of this condition is linked to thiamine’s essential role in cerebral glucose metabolism, mediated through various biochemical pathways that regulate energy metabolism. Thiamine deficiency leads to neuronal cell death via 3 mechanisms: cellular energy failure, oxidative stress, and N-methyl-D-aspartate (NMDA) receptor-mediated excitotoxicity. This cell death preferentially occurs in highly metabolically active regions of the brain including but not limited to the mammillary bodies, dorsomedial thalamus, ocular-motor nuclei, and cerebellum. Damage to these brain regions causes the classic triad associated with WE (altered mental status, ataxic gait, and ophthalmoplegia) [5]. Fortunately, treatment of WE is straightforward, with immediate parenteral administration of thiamine at doses ranging from 1000–1500 mg daily for 2–3 days, followed by 200 mg daily for an additional week [2].
In practice, patients in this demographic often present under complex circumstances, disheveled, potentially with head trauma, exhibiting nonspecific symptoms, and unable to provide a reliable history. In such cases, immediate thiamine replacement is recommended as a low-cost, low-risk, and preventive measure. However, clinicians must also consider Artery of Percheron (AOP) infarction, an anatomic variant of perforator stroke, which can mimic the classic WE triad and requires a fundamentally different management strategy. AOP is a rare anatomical variant found in 4–12% of the general population and accounts for 4–18% of all thalamic strokes. The AOP is a single bifurcating perforator that arises from the P1 segment of a posterior cerebral artery and supplies both thalami and, variably, the rostral midbrain. Occlusion of this artery can lead to a range of clinical presentations depending on infarct type. The most common ischemic pattern in AOP infarction – observed in 43% of cases – is a bilateral paramedian-thalamic and rostral midbrain infarction. Typical presentations include vertical-gaze palsy (63%), memory impairment (58%), and confusion (53%). Other less common presentations include aphasia, dysarthria, motor deficits, and cerebellar signs [6,7]. Diagnosis of AOP infarction is challenging due to the size of the affected anatomy but is best visualized as the midbrain ‘V’ sign on diffusion weighted imaging (DWI) or fluid-attenuated inversion recovery (FLAIR) MRI sequences. The midbrain ‘V’ sign is described as a V-shaped hyperintense signal along the pial surface of the midbrain at the interpeduncular fossa. This finding has a 67% sensitivity for AOP infarction detection [7]. Optimal treatment consists of thrombolytic therapy given within <4.5–6 hours, with thrombectomy not feasible given the diameter of the affected artery [8].
WE and AOP infarction can present with strikingly similar clinical and radiologic findings, including altered mental status, ophthalmoplegia, and bilateral thalamic signal changes on MRI. Distinguishing WE from AOP infarction is vital since timely administration of high-dose intravenous thiamine can be lifesaving in WE, while acute stroke therapies (eg, anticoagulation therapy, antiplatelet therapy, or – if indicated – thrombolysis) may be needed for AOP infarction. Multiple published case reports document the diagnostic difficulty in differentiating between WE and AOP infarction (or another stroke) and the consequent treatment delays. Bhan et al describe a 51-year-old man whose clinical presentation and bilateral thalamic hypodensities activated a stroke-code pathway; however, computed tomography (CT) perfusion, MRI findings, and clinical reversal with thiamine confirmed WE [9]. Conversely, Kaur et al reported a 60-year-old man whose symmetrical thalamic MRI lesions were first labeled as possible WE; however, the acute onset, hypertension, and a repeat DWI study displaying the mid-brain V-sign ultimately confirmed an AOP infarction, underscoring the reciprocal risk of mistaking stroke for thiamine deficiency [10].
The aim of this case report is to emphasize the importance of initiating empiric thiamine therapy alongside stroke evaluation in patients presented with altered mental status. Furthermore, if imaging demonstrates bilateral medial-thalamic lesions, clinicians should be equipped to differentiate between WE and AOP infarction.
Case Report
A 43-year-old man with a past medical history of major depressive disorder and recently confirmed COVID-19, presented to the emergency department (ED) with altered mental status, fever, and generalized weakness that began 3 days prior. The patient complained of headache, diffuse abdominal pain, dyspnea, and lethargy. The patient had no history of alcohol or recreational drug use. Vital signs at presentation included a blood pressure of 139/97 mmHg, heart rate of 122 beats per minute, temperature of 38.1°C, respiratory rate of 25 breaths per minute, and oxygen saturation of 95% on room air. Physical examination revealed mild respiratory distress and diffuse abdominal tenderness but was otherwise unremarkable. The following imaging studies were obtained at ED presentation: A CT head scan without contrast demonstrated hypoattenuation in the left cerebellar hemisphere. A CT angiogram of the head and neck with contrast was unremarkable. A CT scan of the abdomen and pelvis with contrast demonstrated abnormal wall thickening and mesocolonic infiltration of the sigmoid colon, mild associated sigmoid mesocolonic lymphadenopathy, and fat stranding in the presacral region (Figure 1). A CT chest scan for pulmonary embolism revealed an acute left-sided pulmonary embolus (Figure 2).
Due to the hypoattenuation and the patient’s generalized weakness, a code stroke was activated. The initial National Institutes of Health Stroke Scale (NIHSS) was 8, the last known well was 4 days prior to admission, and the Glasgow Coma Score was 13. The neurologic examination revealed that the patient was oriented to location and person but not to date, with no evidence of dysphagia or dysarthria. Extraocular movements, vertical gaze, and convergence were intact. Pupillary examination showed equal and reactive pupils bilaterally (3 mm to 4 mm), with no relative afferent pupillary defect. Facial strength was intact, as was sensory function in all 3 divisions of the trigeminal nerve. Motor examination demonstrated bilateral lower extremity weakness, with right-sided weakness slightly greater than the left. Upper extremity strength was preserved. Reflexes were normal, including the Babinski sign, with bilateral toes down. At this time the stroke team remained uncertain of the etiology, considering possibilities such as stroke versus toxic metabolic encephalopathy, given the presence of pulmonary embolism, sepsis markers (leukocytosis and fever), his abdomen and pelvis CT findings, and his recent COVID-19 infection. Upon further review, the cerebellar hypoattenuation was deemed an artifact. Neurology subsequently ordered a brain MRI and transthoracic echocardiogram, and initiated aspirin 81 mg, 40 mg atorvastatin, and therapeutic enoxaparin. The primary team started empiric antibiotics, including ceftriaxone and metronidazole, in light of a possible intra-abdominal infection.
The next morning during rounds, the patient’s condition acutely worsened. Cranial nerve examination revealed bilateral ophthalmoplegia characterized by impaired abduction in both eyes with end-gaze nystagmus and impaired adduction on horizontal gaze-findings consistent with bilateral cranial nerve (CN) VI palsies with possible involvement of the medial longitudinal fasciculus. Motor testing also revealed worsening of the previous right lower extremity weakness greater than the left. The interval NIHSS was 5 (2 for orientation questions; 1 for left lower extremity drift; 2 for right lower extremity weakness).
Consequently, a head-and-neck CT angiography (CTA) and a brain MRI with and without contrast were ordered. The CTA of the head and neck with contrast ruled out large vessel occlusion but showed scattered non-enlarged lymph nodes along the fascial planes of the neck bilaterally. The MRI brain with and without contrast demonstrated symmetric hyperintense T2 signal and diffusion restriction within the medial thalami, extending into the dorsal midbrain (Figure 3). Given the CTA and MRI findings, the team held a multidisciplinary discussion to determine whether the lesions represented an AOP infarction or WE, taking into account the acute change in neurologic examination, the patient’s hypercoagulable state, and the absence of alcohol use disorder. Further laboratory investigation revealed vitamin B1 (thiamine) at 25.4 nmol/L (reference range: 66–200 nmol/L) and vitamin B6 (pyridoxine) at 4.8 ng/mL (reference range: 5.0–30.0 ng/mL). At this point, the patient was started on a thiamine replacement protocol with 500 mg IV thiamine every 8 hours for the first 5 days, followed by 250 mg IV thiamine daily with an oral 100 mg thiamine tablet daily for another 2 days. Additionally, an autoimmune encephalopathy workup consisting of the Anti-Hu Neuronal Nuclear Antibody Test (ANNA-1), Anti-Ri Neuronal Nuclear Antibody Test (ANNA-2), and Anti-Yo Purkinje Cell Cytoplasmic Antibody Test (PCA-1) was conducted. ANNA-1, ANNA-2, and PCA-1 were all negative. Within 24 hours of starting the IV thiamine protocol, the patient’s mental status as well as ocular movements improved and continued to do so thereafter. Given the patient’s low thiamine levels, clinical improvement with supplementation, and MRI findings, the diagnosis of WE was made.
After a 2-week admission, the patient was deemed stable for discharge to a local skilled nursing facility and was advised to continue apixaban 5 mg, aspirin 81 mg, atorvastatin 80 mg, and thiamine 100 mg, all once daily. Additionally, the patient was recommended to follow up with outpatient neurology for a repeat brain MRI, gastroenterology for an outpatient colonoscopy to investigate a possible malignancy given his abdomen and pelvis CT results, and cardiology for further evaluation of possible atrial fibrillation and review of the remaining laboratory studies.
Follow-up with cardiology, including outpatient monitoring, revealed no evidence of atrial fibrillation. At a neurology follow-up 2 months post-discharge, the patient reported improved cognitive function and physical recovery but had developed chronic gait instability, now requiring a walker despite previously being ambulatory without assistance. He denied new or ongoing focal deficits but noted mild global coordination issues and lumbar pain and weakness. Neurology recommended discontinuing aspirin, apixaban, and atorvastatin and emphasized physical therapy for gait and stability improvement. A repeat brain MRI 7 months after his initial presentation demonstrated subtle T2/FLAIR hyperintensities along the posterior medial thalami bilaterally, more prominent on the left and less intense than on prior imaging.
Discussion
This case report highlights the overlapping clinical and radiological presentations of WE and AOP infarction and reinforces the importance of empiric thiamine administration whenever WE is included in the differential diagnosis, as an inexpensive, low-risk, potentially lifesaving intervention. Both diagnoses are time sensitive as early thiamine administration prevents progression to Korsakoff and prompt stroke therapy limits irreversible ischemic injury.
Although meeting ≥2 Caine criteria yields a specificity of 87% for WE, the diagnosis must still be interpreted in the context of the patient’s history and imaging [2]. In WE, MRI typically shows symmetric T2/FLAIR hyperintensities in the medial thalami, mammillary bodies, tectal plate, and periaqueductal gray [11]. In contrast, there is no defined clinical presentation for AOP infarction but studies have identified that these patients often carry traditional stroke risk factors such as long-standing hypertension, atrial fibrillation, diabetes, or a prior cerebrovascular event, and may acutely present with systolic blood pressure >140 mmHg, depressed consciousness, and vertical-gaze palsies [6,12]. Radiologically, AOP infarction appears as T2/FLAIR hyperintensity with restricted diffusion on DWI and corresponding hypointensity on the apparent diffusion coefficient map, confined to a characteristic bilateral paramedian-thalamic territory. Four patterns are most frequently described: (1) bilateral paramedian-thalamic infarction with rostral midbrain involvement; (2) bilateral paramedian-thalamic infarction without midbrain involvement; (3) combined bilateral paramedian and anterior thalamic infarction with midbrain involvement; and (4) combined bilateral paramedian and anterior thalamic infarction without midbrain involvement [13]. It is important to note that a normal non-contrast CT of the head does not rule out WE nor AOP stroke. Due to the small caliber of the vessel and anatomic variability, follow-up imaging should include CTA, CT perfusion, and brain MRI with DWI and FLAIR sequences [7,11].
In this patient’s case, his risk factors included a prothrombotic state, as evidenced by a pulmonary embolism, and COVID-19 infection, along with medical history, clinical presentation, and CT head scan findings of hypoattenuation. These risk factors reasonably led the team to pursue a stroke pathway. It was only after his condition acutely changed during the following morning rounds that a brain MRI, repeat head-and-neck CT angiogram, and serum thiamine levels were obtained. Once the MRI results became available, there was further discussion on whether the lesions represented WE or an AOP infarction. In this patient’s case, obtaining a more complete nutrition and social history in the ED, as well as escalating to advanced imaging earlier, may have enabled earlier diagnosis and intervention while avoiding unnecessary imaging and treatment.
Comparison with the 2 previously cited reports further underscores the diagnostic challenge. Bhan et al described a 51-year-old man who presented with dysarthria and confusion but no ocular findings; the Face, Arm, Speech, Time (FAST) criteria raised stroke alarm, and non-contrast CT showed bilateral thalamic hypodensities. Although CTA was normal, CT perfusion demonstrated hyper- rather than hypo-perfusion in the thalami, prompting consideration of WE. This diagnosis was later confirmed on FLAIR MRI [9]. In Kaur et al, a 60-year-old man with hypertension, diabetes, and alcohol use disorder arrived comatose with vertical-gaze palsy. His initial CT was unremarkable, but MRI revealed bilateral thalamic lesions, initially interpreted as WE and treated as such. After further discussion due to sudden cerebellar signs and vertical gaze palsy as well as rereview of the MRI images, the diagnosis was changed to AOP infarction [10].
This report is limited by its single patient design and lack of CT perfusion imaging. Nevertheless, this case report, along with the published examples reviewed, highlights the need to keep both stroke mimics and rare infarcts on the differential when confronted with a nondiagnostic initial CT. We suggest that while the standard stroke pathway is pursued, empiric administration of 500 mg intravenous thiamine to any patient with acute encephalopathy and ocular-motor abnormalities is a low-risk, potentially lifesaving step that can be initiated while advanced MRI sequences (DWI and FLAIR) are being arranged. Management can then be tailored once imaging and laboratory data clarify the diagnosis. Prospective studies should test the cost-effectiveness of this approach, its impact on door-to-diagnosis times and neurologic outcomes, and the value of targeted clinician education programs in reducing both missed WE cases and unnecessary thrombolysis.
Conclusions
WE and AOP infarction can present almost identically, with acute encephalopathy, ocular-motor abnormalities, and symmetric medial-thalamic lesions. Initial head CT is often nondiagnostic, and even on MRI, both conditions may show bilateral thalamic hyperintensities. Because definitive distinction takes time, empiric high-dose thiamine, a safe, inexpensive, and potentially lifesaving intervention, should be administered while advanced imaging and further workup are underway.
Figures
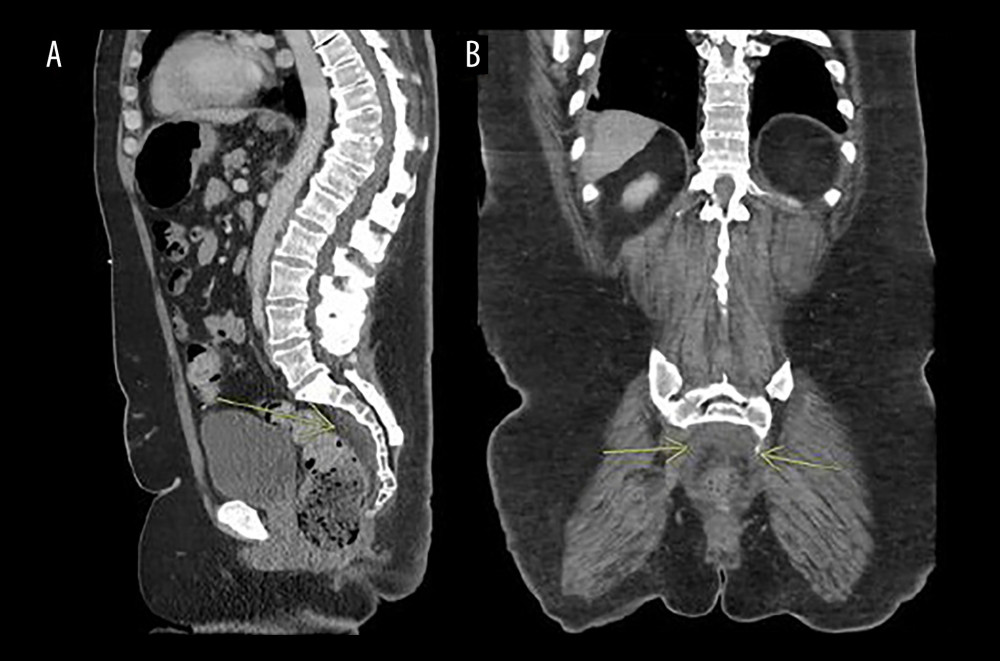 Figure 1. (A) Sagittal view of the computed tomography of the abdomen and pelvis with contrast, demonstrating fat stranding in the presacral region posterior to the rectosigmoid (yellow arrow). (B) Coronal view of the abdomen showing the same findings, for comparison.
Figure 1. (A) Sagittal view of the computed tomography of the abdomen and pelvis with contrast, demonstrating fat stranding in the presacral region posterior to the rectosigmoid (yellow arrow). (B) Coronal view of the abdomen showing the same findings, for comparison. 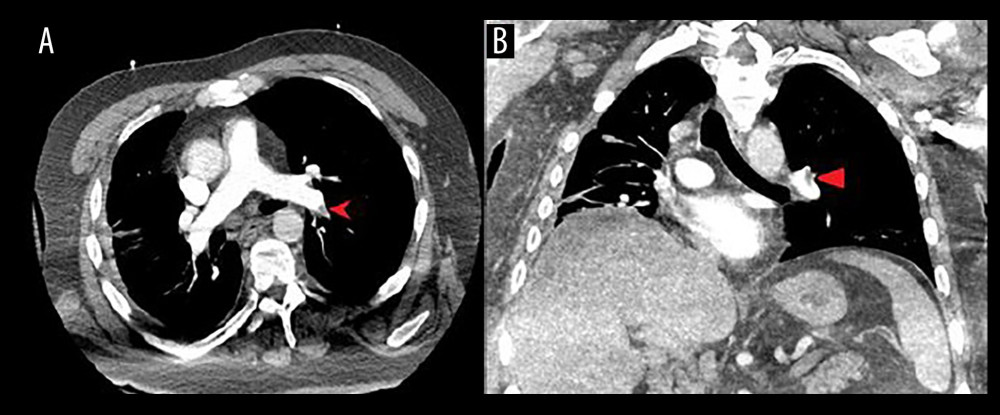 Figure 2. (A) Axial view of the chest showing a computed tomography angiography (CTA) with left-sided pulmonary embolism (left arrow). (B) Coronal view of the chest showing the same CTA, for comparison.
Figure 2. (A) Axial view of the chest showing a computed tomography angiography (CTA) with left-sided pulmonary embolism (left arrow). (B) Coronal view of the chest showing the same CTA, for comparison. 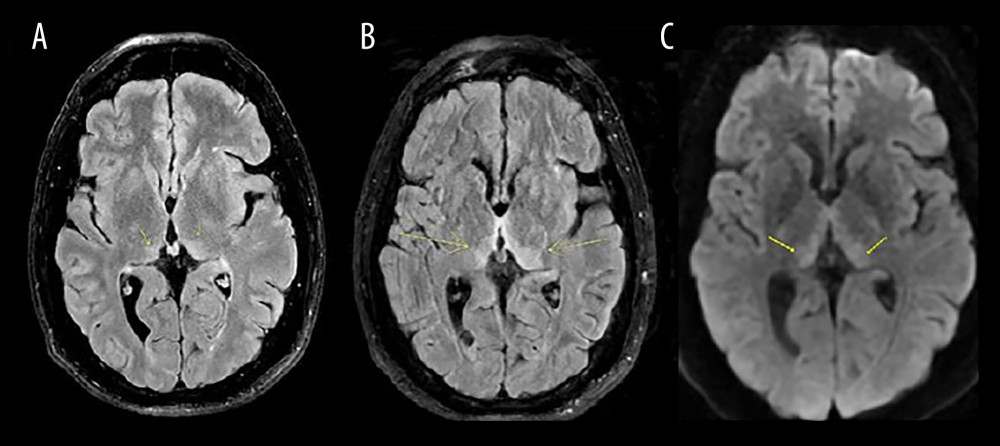 Figure 3. (A, B) Axial Fluid-Attenuated Inversion Recovery (FLAIR) magnetic resonance imaging (MRI) brain sequences with bilateral medial-thalamic changes and tectal/periaqueductal grey midbrain signal changes (yellow arrows). (C) Axial diffusion weighted imaging (DWI) brain MRI demonstrating corresponding areas of restricted diffusion.
Figure 3. (A, B) Axial Fluid-Attenuated Inversion Recovery (FLAIR) magnetic resonance imaging (MRI) brain sequences with bilateral medial-thalamic changes and tectal/periaqueductal grey midbrain signal changes (yellow arrows). (C) Axial diffusion weighted imaging (DWI) brain MRI demonstrating corresponding areas of restricted diffusion. References
1. Kopelman MD, Thomson AD, Guerrini I, Marshall EJ, The Korsakoff syndrome: Clinical aspects, psychology, and treatment: Alcohol Alcohol, 2009; 44(2); 148-54
2. Galvin R, Bråthen G, Ivashynka A, EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy: Eur J Neurol, 2010; 17(12); 1408-18
3. Caine D, Halliday GM, Kril JJ, Harper CG, Operational criteria for the classification of chronic alcoholics: Identification of Wernicke’s encephalopathy: J Neurol Neurosurg Psychiatry, 1997; 62(1); 51-60
4. Vasan S, Kumar A, Wernicke encephalopathy. [Updated 2023 Aug 14]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK470344/
5. Butterworth RF, Thiamin deficiency and brain disorders: Nutr Res Rev, 2003; 16(2); 277-84
6. Kichloo A, Jamal SM, Zain EA, Artery of Percheron infarction: A short review: J Investig Med High Impact Case Rep, 2019; 7; 2324709619867355
7. Lazzaro NA, Wright B, Castillo M, Artery of Percheron infarction: Imaging patterns and clinical spectrum: Am J Neuroradiol, 2010; 31(7); 1283-89
8. Zhang B, Wang X, Gang C, Wang J, Acute Percheron infarction: A precision learning: BMC Neurol, 2022; 22(1); 207
9. Bhan A, Advani R, Kurz KD, Wernicke’s encephalopathy mimicking acute onset stroke diagnosed by CT perfusion: Case Rep Neurol Med, 2014; 2014; 673230
10. Kaur H, Mohan G, Sharma V, Artery of Percheron infarct: A case report: Int J Res Med Sci, 2018; 6(3); 1035-38
11. Zuccoli G, Pipitone N, Neuroimaging findings in acute Wernicke’s encephalopathy: Review of the literature: Am J Roentgenol, 2009; 192(2); 501-8
12. Ikramuddin SS, Coburn JA, Ramezani S, Streib C, Artery of Percheron infarction: Clinical presentation and outcomes: Neurol Clin Pract, 2024; 14(2); e200266
13. Arauz A, Patiño-Rodríguez HM, Vargas-González JC, Clinical spectrum of artery of Percheron infarct: Clinical–radiological correlations: J Stroke Cerebrovasc Dis, 2014; 23(5); 1083-88
Figures
Figure 1. (A) Sagittal view of the computed tomography of the abdomen and pelvis with contrast, demonstrating fat stranding in the presacral region posterior to the rectosigmoid (yellow arrow). (B) Coronal view of the abdomen showing the same findings, for comparison.Figure 2. (A) Axial view of the chest showing a computed tomography angiography (CTA) with left-sided pulmonary embolism (left arrow). (B) Coronal view of the chest showing the same CTA, for comparison.Figure 3. (A, B) Axial Fluid-Attenuated Inversion Recovery (FLAIR) magnetic resonance imaging (MRI) brain sequences with bilateral medial-thalamic changes and tectal/periaqueductal grey midbrain signal changes (yellow arrows). (C) Axial diffusion weighted imaging (DWI) brain MRI demonstrating corresponding areas of restricted diffusion. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133