14 December 2025: Articles 
Acquired Subglottic Stenosis in a 2-Month-Old Infant After Prolonged Intubation Associated With Pertussis Pneumonia: A Case Report
Unusual or unexpected effect of treatment, Rare disease
Yun-Gai Cheng ABCDEF 1, Xiao-Fen Tao BCD 1, Xu Dan ABF 1, Xue-Jing Li BCD 1, Lei Wu ABCD 1*, Xi-Ling Wu BDFG 1DOI: 10.12659/AJCR.948709
Am J Case Rep 2025; 26:e948709






Abstract
BACKGROUND: Subglottic stenosis (SGS) is a life-threatening airway narrowing often acquired after prolonged intubation in infants. Although severe cases have historically required open surgery, emerging endoscopic techniques such as laser therapy, balloon dilation, and cryotherapy provide less invasive alternatives with promising outcomes. This case report describes a 2-month-old female infant who developed subglottic stenosis after intubation and mechanical ventilation for acute respiratory failure due to pertussis pneumonia.
CASE REPORT: A 2-month-old female infant with a history of pertussis pneumonia requiring 10 days of intubation presented with respiratory distress and stridor. Diagnostic imaging and flexible laryngoscopy confirmed grade 3 SGS (Cotton-Myer classification). She underwent a multimodal endoscopic approach, including holmium laser ablation (0.5-1.0 J/pulse) for fibrotic tissue removal, balloon dilation (6 mm, 14 atmospheres) to expand the stenotic segment, and cryotherapy (-70°C) to minimize scar formation. Immediate post-procedural improvement was observed, and oxygen was gradually tapered by day 5. Follow-up fiber laryngoscopy at 1 month demonstrated sustained airway patency without restenosis.
CONCLUSIONS: This case supports the efficacy of combined endoscopic modalities for severe pediatric SGS, offering advantages over open surgery, including reduced morbidity and faster recovery. Long-term studies are needed to confirm durability, particularly for high-grade stenosis. Standardized protocols for laser settings, balloon sizing, and cryotherapy duration should be established to optimize outcomes.
Keywords: subglottic stenosis, Infant, Intubation, intratracheal, case report, Humans, Female, Infant, Laryngostenosis, Intubation, Intratracheal, Laryngoscopy, Whooping Cough, Laser Therapy
Introduction
Pertussis (whooping cough) remains a major global public health challenge caused by the human pathogen
The primary etiologies of acquired subglottic stenosis (SGS) in pediatric patients include intubation lasting longer than 7 to 10 days, inappropriate tube size, patient agitation leading to tube microtrauma, localized infection, and comorbidities such as gastroesophageal reflux disease or genetic syndromes such as Down syndrome [4–8]. Although the overall risk of SGS after neonatal intubation is approximately 1%, prolonged mechanical ventilation substantially increases this risk [9]. Severe cases may result in respiratory distress, recurrent croup, or complete airway obstruction warranting tracheotomy [10].
Management of SGS is guided by the Cotton-Myer grading system. Grades I and II stenosis can often be treated endoscopically using techniques such as balloon dilation, laser excision, or steroid injection. More severe Grades III and IV cases may require open surgical procedures, including laryngotracheal reconstruction or cricotracheal resection [11]. Recent advances favor multimodal endoscopic approaches incorporating holmium laser for precise ablation, balloon dilation for controlled expansion, and adjuvant cryotherapy to minimize scar recurrence [8,12,13]. Jiao et al reported treatment of 15 pediatric patients with SGS (ages 3 months to 3 years) using holmium laser and cryotherapy via flexible bronchoscopy; they achieved a 100% success rate without restenosis at the 6-month follow-up [13]. This case report describes a 2-month-old female infant who developed severe SGS (Grade 3) after intubation and mechanical ventilation for acute respiratory failure secondary to pertussis pneumonia; successful treatment was achieved via combined endoscopic modalities.
Case Report
A 2-month-old girl was admitted to the intensive care unit of our hospital in September 2022 with a 6-day history of shortness of breath and cough, accompanied by hoarseness for 2 days. Approximately 1 month earlier, she had been hospitalized locally for pertussis, requiring intubation and mechanical ventilation for 10 days; she also received erythromycin injections for 2 weeks. She was the third child of unrelated healthy parents, born vaginally at 37+1 weeks of gestation without any medical complications at birth. Upon admission to the intensive care unit, her vital signs were as follows: body temperature, 36.9°C; heart rate, 204 beats/min; respiratory rate, 47 breaths/min; and blood pressure, 99/72 mmHg. Physical examination revealed no accessory breathing sounds and normal heart sounds on auscultation. Chest wall retraction was observed, but there was no hepatosplenomegaly. The patient developed hypoxemia and respiratory distress; therefore, oxygen therapy (2 L/min via nasal cannula) was administered. However, her symptoms did not considerably improve. To further clarify the etiology, a neck and chest computed tomography (CT) scan was performed. CT imaging revealed localized SGS, and the narrowest portion measured approximately 1.6 mm in width. A linear soft tissue structure was observed above the narrowest segment within the lumen (Figure 1A, 1B). Subsequent fiber laryngoscopy demonstrated severe SGS, characterized by a minute pinhole opening (Figure 1C). The patient was diagnosed with severe acquired SGS (Grade 3), likely secondary to prolonged intubation during her prior hospitalization for pertussis.
On hospital day 2, after departmental discussion, a multidisciplinary team (i.e., otolaryngologists, pulmonologists, and anesthesiologists) decided to perform balloon dilation airway plasty combined with holmium laser therapy and cryotherapy under general anesthesia. The patient received an initial loading dose of dexamethasone (1 μg/kg), followed by a maintenance infusion of 0.3 μg/kg/h. General anesthesia was maintained with 3% sevoflurane inhalation, remifentanil (0.2 μg/kg/min), intravenous methylprednisolone (30 mg), atropine (0.25 mg), and lidocaine (25 mg). After deep sedation and spontaneous respiration had been achieved, an additional 10 mg of etomidate were administered to deepen anesthesia. Laryngoscopy was then performed to expose the supraglottic and glottic larynx; this was followed by the insertion of a 4.9-mm outer diameter flexible bronchoscope (Olympus 260; Olympus Corp) into the subglottic region (Figure 2A) in accordance with our hospital’s protocol [14]. The holmium laser (0.5–1.0 J/pulse) was used to excise granulation and scar tissue precisely over multiple sessions, resulting in substantial enlargement of the subglottic lumen (Figure 2B). A 6.0-mm balloon was subsequently inflated to 14 atmospheres for 15 s and repeated twice (Figure 2C, 2D). Carbon dioxide cryotherapy was then applied to the treated area to reduce thermal injury, scar formation, and restenosis (Figure 2E). Cryotherapy (−70°C) was administered for 30 to 40 s at multiple sites and repeated twice. Postoperatively, the airway lumen showed considerable enlargement (Figure 2F), and the patient demonstrated clinically significant improvement in respiratory symptoms, including stridor, retractions, and dyspnea. Follow-up bronchoscopy with repeat balloon dilation and cryotherapy was performed on hospital day 4, revealing further improvement in subglottic patency and a clear airway (Figure 3A). The nasal tube was removed on hospital day 5, and the patient was discharged on hospital day 11. Weekly outpatient balloon dilation and cryotherapy sessions were conducted for 2 weeks (Figure 3B). One month after discharge, laryngoscopy showed no residual stenosis (Figure 3C), and the patient remained asymptomatic. Telephone follow-ups were conducted at approximately 6 and 12 months after discharge. The child remained free of respiratory symptoms and demonstrated normal growth and development. Due to the absence of clinical manifestations, the parents declined further imaging and endoscopic airway evaluations. All procedures were performed with parental consent.
Discussion
SGS remains a complex challenge in pediatric airway management, particularly in cases of acquired stenosis due to prolonged intubation [5,15]. This case report demonstrates the successful treatment of severe Grade 3 SGS in a 2-month-old infant through multimodal endoscopic therapy involving holmium laser, balloon dilation, and cryotherapy; durable resolution was achieved. This approach may offer advantages over conventional open surgery by reducing morbidity and expediting recovery. Careful selection of parameters such as laser energy, balloon size, and cryotherapy duration is essential to ensure procedural safety [5,13].
The patient’s presentation of stridor and respiratory distress after prolonged intubation for pertussis pneumonia closely aligns with the typical features of SGS described in previous reports [10,16]. Similar to the cohort study by Rodriguez et al [16], our patient developed stenosis after 10 days of intubation, consistent with evidence indicating an 8-fold increase in SGS risk when intubation exceeds 7 days [9]. Diagnostic confirmation via CT and laryngoscopy was consistent with current standards [17], whereas the use of precise CT measurements (1.6 mm) enabled more accurate quantification compared with conventional Cotton-Myer grading alone [11].
Our management strategy differed from conventional approaches in 3 key aspects. First, sequential holmium laser ablation (0.5–1.0 J/pulse) was utilized instead of CO2 laser, allowing flexible bronchoscopy delivery – a technique that enhances precision in pediatric airways [18,19]. Second, balloon dilation (6 mm, 14 atmospheres) was performed after laser ablation, rather than older bougienage techniques; this combined method achieves immediate patency rates of 85%, compared with 60% for single-modality interventions in similar reports [20,21]. Third, adjuvant cryotherapy (−70°C) was incorporated to reduce restenosis, with reported rates of 0% at 1 month vs 15% to 20% for laser-only treatments [13,22]. These refinements likely contributed to the patient’s rapid recovery (extubation within 5 days), which contrasted with the typical 10- to 14-day recovery period observed in open surgical series [5,12].
The clinical course in this case largely paralleled the outcomes reported by Jiao et al [13] using similar techniques, although their longer follow-up period (>6 months) provides stronger evidence of long-term durability. Our case extends these findings by demonstrating efficacy in a younger infant (2 months vs median 7 months) with more severe stenosis (Grade 3 vs Grade 2). However, as emphasized by Quesnel et al [21], successful management requires the collaboration of multidisciplinary teams and precise parameter selection, particularly in balloon sizing (approximately 1 mm larger than the age-appropriate endotracheal tube) to minimize the risk of tracheal injury [23].
Although the present report is limited by its short follow-up duration, absence of objective metrics for outcome evaluation, and inherent single-case bias, future research should aim to conduct randomized controlled trials comparing multimodal endoscopic therapy with single-modality interventions or open surgical approaches. Moreover, the establishment of standardized protocols for balloon sizing, laser parameters, and cryotherapy duration will be essential to enhance reproducibility and optimize treatment outcomes.
Conclusions
This case demonstrates that a combination of endoscopic modalities – holmium laser, balloon dilation, and cryotherapy – can effectively manage severe acquired SGS in infants, providing a less invasive alternative to conventional open surgery with faster recovery. This multimodal approach may be considered a primary treatment option for Grade 3 SGS, although validation through larger studies with extended follow-up is warranted to confirm long-term efficacy. Standardization of procedural parameters across institutions will be critical for ensuring consistent and reproducible results.
Figures
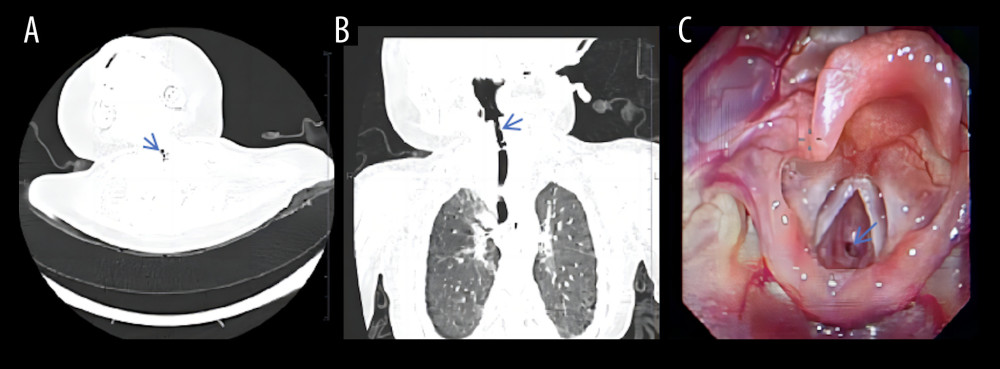 Figure 1. Neck and chest computed tomography scans (A, B) demonstrated localized subglottic stenosis. Fiber laryngoscopy (C) revealed severe subglottic stenosis with a pinhole-sized lumen.
Figure 1. Neck and chest computed tomography scans (A, B) demonstrated localized subglottic stenosis. Fiber laryngoscopy (C) revealed severe subglottic stenosis with a pinhole-sized lumen. 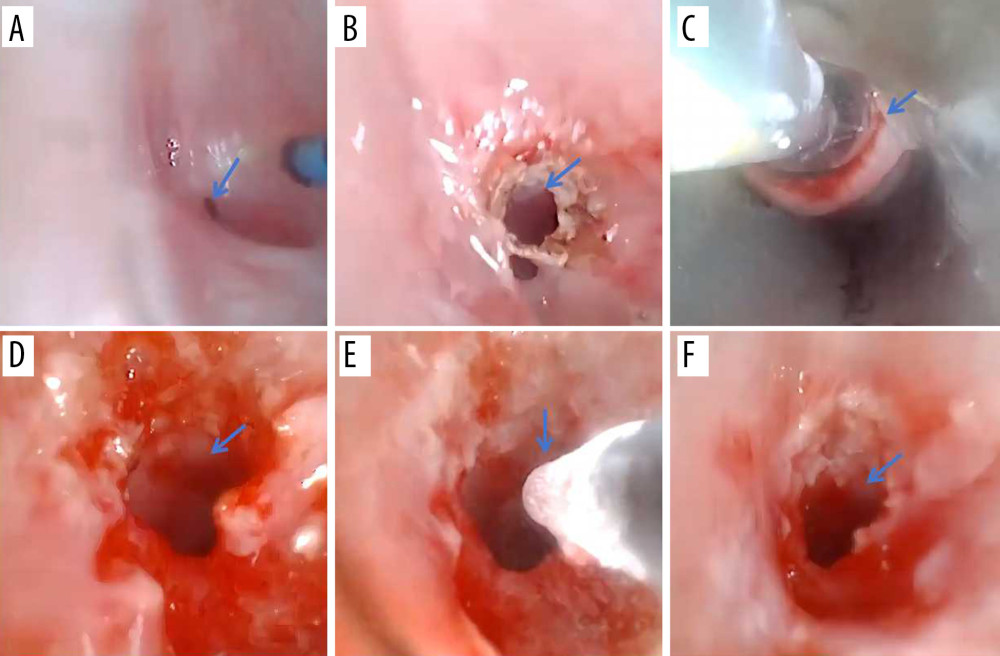 Figure 2. Bronchoscopic interventional treatment of subglottic stenosis and postoperative airway. (A) Bronchoscopy before therapy revealed airway stenosis. (B–E) Holmium laser, balloon dilation, and cryotherapy were performed to treat the stenotic region. (F) After the first intervention, the airway lumen was considerably enlarged.
Figure 2. Bronchoscopic interventional treatment of subglottic stenosis and postoperative airway. (A) Bronchoscopy before therapy revealed airway stenosis. (B–E) Holmium laser, balloon dilation, and cryotherapy were performed to treat the stenotic region. (F) After the first intervention, the airway lumen was considerably enlarged. 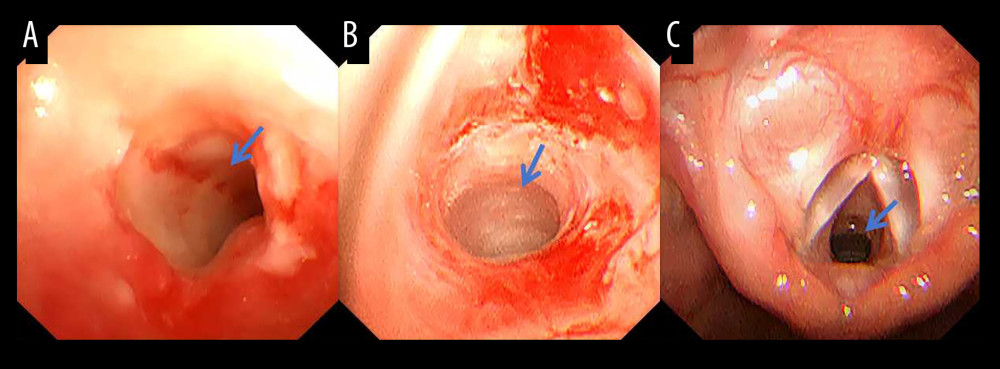 Figure 3. (A) Bronchoscopy on postoperative day 4 and (B) 2 weeks later revealed clinically significant improvement in airway patency. (C) One month postoperatively, fiber laryngoscopy showed complete resolution of stenosis
Figure 3. (A) Bronchoscopy on postoperative day 4 and (B) 2 weeks later revealed clinically significant improvement in airway patency. (C) One month postoperatively, fiber laryngoscopy showed complete resolution of stenosis References
1. World Health Organization: Laboratory manual for the diagnosis of whooping cough caused by Bordetella pertussis-Bordetella parapertussis. Update 2014 [Internet], 2014, Geneva, WHO [cited 2020 Jan 7]. Available from: https://www.who.int/publications/i/item/laboratory-manual-for-the-diagnosis-of-whooping-cough-caused-by-bordetella-pertussis-bordetella-parapertussis.-update-2014
2. Lauria AM, Zabbo CP, Pertussis: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing [cited 2025 Sep 10]. Available from:http://www.ncbi.nlm.nih.gov/books/NBK519008/
3. Aldas S, Ersoy M, Ozmen BO, A pediatric health problem increasing with migration: pertussis reloading: Int J Infect Dis, 2025; 160; 108040
4. Cakir E, Atabek AA, Calim OF, Post-intubation subglottic stenosis in children: Analysis of clinical features and risk factors: Pediatr Int, 2020; 62(3); 386-89
5. Oh SK, Park KN, Lee SW, Long-term results of endoscopic dilatation for tracheal and subglottic stenosis: Clin Exp Otorhinolaryngol, 2014; 7(4); 324-28
6. Meneghini L, Zadra N, Metrangolo S, Narne S, Giusti FPost-intubation subglottal stenosis in children: risk factors and prevention in pediatric intensive care: Minerva Anestesiol, 2000; 66(6); 467-71 [in Italian]
7. Stamm D, Floret D, Stamm CSubglottal stenosis following intubation in children: Arch Fr Pediatr, 1993; 50(1); 21-25 [in French]
8. Jagpal N, Sommerfeldt J, Shabbir N, Subglottic stenosis: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing [cited 2025 Sep 10]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK563265/
9. Marston AP, White DR, Subglottic stenosis: Clin Perinatol, 2018; 45(4); 787-804
10. Hanlon K, Boesch RP, Jacobs I, Subglottic stenosis: Curr Probl Pediatr Adolesc Health Care, 2018; 48(4); 129-35
11. Myer CM, O’Connor DM, Cotton RT, Proposed grading system for subglottic stenosis based on endotracheal tube sizes: Ann Otol Rhinol Laryngol, 1994; 103(4); 319-23
12. Maresh A, Preciado DA, O’Connell AP, Zalzal GH, A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis: JAMA Otolaryngol Head Neck Surg, 2014; 140(10); 901-5
13. Jiao A, Liu F, Lerner AD, Effective treatment of post-intubation subglottic stenosis in children with holmium laser therapy and cryotherapy via flexible bronchoscopy: Pediatr Investig, 2019; 3(1); 9-16
14. Wu L, Sha MC, Wu XL, Primary intratracheal neurilemmoma in a 10-year-old girl: A case report: World J Clin Cases, 2021; 9(29); 8888-93
15. Talwar R, Virk JS, Bajaj Y, Paediatric subglottic stenosis – have things changed? Our experience from a developing tertiary referral centre: Int J Pediatr Otorhinolaryngol, 2015; 79(12); 2020-22
16. Rodríguez H, Cuestas G, Botto H, Post-intubation subglottic stenosis in children. Diagnosis, treatment and prevention of moderate and severe stenosis: Acta Otorrinolaringol Esp, 2013; 64(5); 339-44
17. Jefferson ND, Cohen AP, Rutter MJ, Subglottic stenosis: Semin Pediatr Surg, 2016; 25(3); 138-43
18. Fong M, Clarke K, Cron C, Clinical applications of the holmium: YAG laser in disorders of the paediatric airway: J Otolaryngol, 1999; 28(6); 337-43
19. Verret D, Jategaonkar A, Helman S, Holmium laser for endoscopic treatment of benign tracheal stenosis: Int Arch Otorhinolaryngol, 2018; 22(3); 203-7
20. Durden F, Sobol SE, Balloon laryngoplasty as a primary treatment for subglottic stenosis: Arch Otolaryngol Head Neck Surg, 2007; 133(8); 772-75
21. Quesnel AM, Lee GS, Nuss RC, Minimally invasive endoscopic management of subglottic stenosis in children: success and failure: Int J Pediatr Otorhinolaryngol, 2011; 75(5); 652-56
22. Lawlor CM, Shah RK, A novel and promising addition to the treatment arsenal for post-intubation subglottic stenosis: Holmium laser ablation and cryotherapy via flexible bronchoscopy: Pediatr Investig, 2019; 3(1); 17-18
23. Sharma SD, Gupta SL, Wyatt M, Safe balloon sizing for endoscopic dilatation of subglottic stenosis in children: J Laryngol Otol, 2017; 131(3); 268-72
Figures
Figure 1. Neck and chest computed tomography scans (A, B) demonstrated localized subglottic stenosis. Fiber laryngoscopy (C) revealed severe subglottic stenosis with a pinhole-sized lumen.Figure 2. Bronchoscopic interventional treatment of subglottic stenosis and postoperative airway. (A) Bronchoscopy before therapy revealed airway stenosis. (B–E) Holmium laser, balloon dilation, and cryotherapy were performed to treat the stenotic region. (F) After the first intervention, the airway lumen was considerably enlarged.Figure 3. (A) Bronchoscopy on postoperative day 4 and (B) 2 weeks later revealed clinically significant improvement in airway patency. (C) One month postoperatively, fiber laryngoscopy showed complete resolution of stenosis In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133